
Abstract
Objectives:
Surgical management of small renal masses can be challenging in frail patients and thus modalities such as radiofrequency ablation (RFA) have emerged as valid alternative options. The aim of the current study was to present mid-term oncological and functional results on a series of patients with cT1a renal cell carcinomas (RCCs) who were unfit for surgery and underwent RFA using ultrasound guidance under local anesthesia.
Methods:
Data from patients fulfilling the study selection criteria were retrospectively collected. RENAL nephrometry score was used for tumor description. Parametric tests were used for data analysis and survival curves were estimated using the Kaplan–Meier method.
Results:
Overall, 32 patients (mean±standard deviation age, 72.4 ± 7.6 years) with biopsy-proven RCCs (tumor size, 23.75 ± 10.44 mm and RENAL score, 5.28 ± 1.33) underwent 32 RFA sessions. Twenty-seven patients (84.4%) had low complexity masses and five patients had masses of intermediate complexity (15.6%) according to RENAL score categorization. Over a follow-up period of 22.1 ± 13.7 months, one case of primary treatment failure was recognized (primary technical success 97.0%), and overall, three patients were diagnosed with residual disease (primary technique effectiveness 90.6%). No major complications occurred during the postprocedure 90-day follow up, while no difference was found in serum creatinine and estimated glomerular filtration rate pre and post procedure. Patients with intermediate-complexity renal lesions had shorter time to recurrence in comparison to low-complexity masses (p = 0.002). All patients were alive at the time of study data analysis without diagnosed metastases.
Conclusions:
Percutaneous RFA of small RCCs using ultrasound-based guidance under local anesthesia can be an effective alternative method for managing patients who are unfit for surgery.
Introduction
An increasing trend in incidental detection of small renal masses has been observed, mainly due to the widespread use of abdominal imaging, such as sonography and computed tomography (CT) [Boss et al. 2007; Jayson and Sanders, 1998; Ljungberg et al. 2010]. Current clinical guidelines recommend surgical excision of renal masses and specifically highlight the benefits of partial nephrectomy over radical nephrectomy as it has been proven to offer similar oncological outcomes for lesions up to 7 cm, while at the same time it preserves adequate renal function [Campbell et al. 2009; Ljungberg et al. 2010].
While nephron-sparing surgical techniques are encouraged for patients with T1a and T1b tumors, specific concern has been expressed for management of these lesions in patients of advanced age or those with severe comorbidities that make them unsuitable for surgery [Baillargeon-Gagné et al. 2010; Choueiri et al. 2011]. Active surveillance of incidental small renal masses has been proposed for some patients as it has been proven that rates of lesion growth and metastatic progression are low in this specific group [Conti et al. 2015; Danzig et al. 2015].
In addition, ablative modalities that include cryoablation and radiofrequency ablation (RFA) have emerged as valid alternatives for small renal mass management in patients who are poor candidates for surgery [Heuer et al. 2010; Kunkle and Uzzo, 2008; Kutikov et al. 2009; Van Poppel et al. 2011]. RFA can be performed using ultrasound or CT guidance and various methods of ablation technique have been presented. Several studies have shown diverse findings in oncological outcomes and in safety and functional parameters, such as operation-associated complications and degree of impairment of renal function after treatment. The latest reports on RFA reveal satisfactory mid- and long-term results [Chang et al. 2015; Hiraoka et al. 2009; Iannuccilli et al. 2015; McClure et al. 2014; Psutka et al. 2013; Takaki et al. 2010; Thompson et al. 2015]; however, due to the lack of sufficient evidence, no specific recommendation regarding ablation techniques for small renal masses can be given so far.
The aim of the current study was to present mid-term oncological and functional results on a series of patients with T1a renal masses who were poor candidates for surgery and underwent RFA using exclusively ultrasound guidance.
Material and methods
Study design and population
From January 2011 to December 2014, a total of 32 patients underwent ultrasound-guided percutaneous RFA for small renal tumors under the approval of the ethical committee of the University Hospital of Larissa. Study inclusion criteria were age over 18 years, diagnosis of a solitary renal mass up to 3.5 cm in maximum diameter and inoperability (defined as American Society of Anesthesiologists (ASA) score >3 due to severe comorbidities that did not allow general anesthesia) or patients’ refusal to undergo surgery.
Patients with nonbiopsy-proven renal cell carcinomas (RCCs) were excluded according to study protocol. Preoperatively, patients underwent imaging with contrast-enhanced CT of the abdomen, chest CT and laboratory screening that included complete blood count, coagulation testing and serum creatinine. A thorough explanation of the procedure was offered to all patients, possible outcomes and complications were analyzed and patients were included in the study after written consent was obtained.
Description of procedure
All study patients underwent ultrasound-guided percutaneous RFA by two staff urologists. Thirty minutes before the procedure, 100 mg of pethidine HCl (intramuscularly) and diazepam (0.1 mg/kg orally) were administered to all patients. Patients were placed in the prone position and the appropriate site of puncture was selected under ultrasonic guidance. Infiltration of the skin and injection of 2% lignocaine along the direction of the intended puncture was performed with a 21-gauge Chiba needle using a free-hand technique [Aravantinos et al. 2007]. A single dose of intravenous antibiotic (usually second-generation cephalosporin) was also administered as prophylaxis. Intravenous midazolam was administrated by an anesthesiologist upon demand of the patient. During the procedure, heart rate, arterial pressure, ventilation frequency and peripheral oxygen saturation were monitored continuously.
At the time of ablation of the renal tumor a biopsy was performed in all patients with an 18 G core biopsy needle. At least two core biopsies of each tumor were taken. Consequently, a 17 G needle electrode was inserted into the renal lesion under continuous ultrasound guidance. RFA was performed with impedance-controlled pulsed current from a 200 W RF3004 generator. The needle has an insulated active edge in various lengths, depending on the diameter of the targeted mass. Needles with an active edge of 0.5 cm/1.0 cm/2.0 cm and 3.0 cm are available for lesions of 1 cm/1.5 cm/2.5 cm and 3.5 cm maximal diameter.
Follow up
Four weeks after the procedure, imaging with contrast-enhanced CT or magnetic resonance imaging of the abdomen was performed to evaluate treatment efficacy and exclude residual tumor. The follow-up protocol additionally included imaging at 6 and 12 months postoperatively, and then annually, to evaluate possible residual tumor at treatment site. In accordance with the current recommendations for image-guided tumor ablation outcomes [Ahmed et al. 2014], ‘residual tumor’ is the presence of enhanced tissue (increase of at least 20 Hounsfield units on CT imaging, after intravenous administration of contrast) at the treatment site. Thus, the absence of residual tumor at first follow-up imaging after the procedure defines ‘complete ablation’. In this study, the term ‘residual tumor’ is used regardless of the time of diagnosis, as recommended terminology suggests that tissue enhancement within the treatment site can be explained by treatment-spared viable tumor cells. ‘Primary technical success’ is the proportion of treatments that led to complete ablation on the first follow-up evaluation, while ‘primary technique effectiveness’ is the proportion of treatments that led to complete ablation over the whole follow-up period.
Data collection and statistical analysis
Patients’ medical records were reviewed and demographic characteristics (age, sex), tumor characteristics (tumor size, location, number of tumors and biopsy pathology), renal function and perioperative and postoperative parameters and complications were gathered for statistical analysis. Complications were recorded using the Clavien–Dindo classification system and renal function was assessed by estimated glomerular filtration rate (eGFR) calculation using the Cockcroft–Gault calculator [Clavien et al. 2009; Cockcroft and Gault, 1976].
The RENAL nephrometry scoring system was retrospectively applied to all patients, based on available data [Kutikov and Uzzo, 2009]. The RENAL score evaluates and gives points or descriptors to anatomic parameters of renal masses (maximal radius, endophytic/exophytic location, nearness to collecting system, laterality and location of lesions). CT imaging was studied in detail and the relevant scores were given by two independent reviewers; in the case of disagreement, an additional reviewer was recruited so as to finally have two identical RENAL scores. According to its current format, the RENAL score ranges from 4 to 12, and complexity of renal masses can be categorized as low (score 4–6), moderate (7–9) or high (10–12).
SPSS software was used for statistical analysis (version 12, SPSS Inc., Chicago, IL, USA). Continuous variables with normal distribution are presented as mean±standard deviation (SD), while categorical variables are presented as proportions. The paired t test was used to analyze patients’ continuous data before and after the procedure. Fisher’s exact test was used to compare categorical variables. Residual tumor-free survival was calculated using Kaplan–Meier analysis and comparisons were made using log-rank analysis. The level of statistical significance for all statistical tests was set to 0.05.
Results
Demographic and basic clinical and laboratory parameters of patients included in the present study are shown in Table 1. In total, 32 patients were included (27 men, 5 women, 84.4% and 15.6%, respectively), with a mean±SD age of 72.4 ± 7.6 years (minimum 55, maximum 85 years), mean±SD tumor size of 23.75 ± 10.44 mm (minimum 6.0, maximum 35.00 mm) and mean±SD RENAL score of 5.28 ± 1.33. According to the RENAL score categorization, 27 patients (84.4%) had low complexity masses and 5 patients had masses of intermediate complexity (15.6%); no high complexity masses were included in study patients. Tumor-specific characteristics are provided in Table 2.
Demographic and clinical characteristics of included patients.

ASA, American Society of Anesthesiologists.
Characteristics of renal masses in study patients.
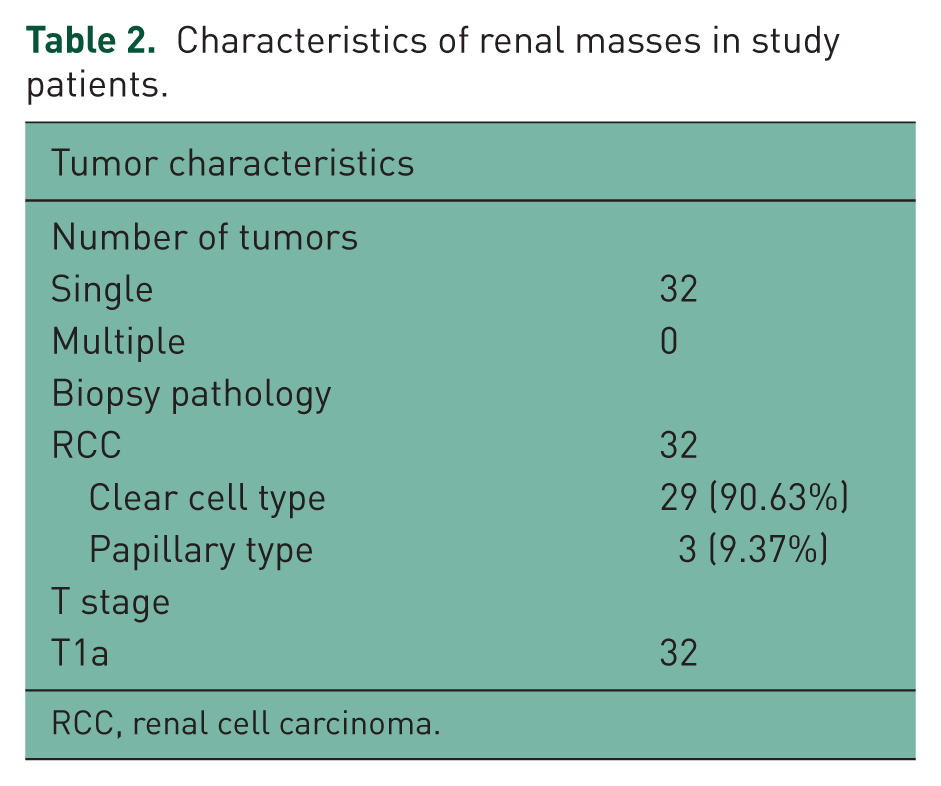
RCC, renal cell carcinoma.
In terms of intraoperative parameters, ablation power was increased from 60 to 140 W with a mean power of 100 W used per ablation cycle. The mean ablation time was 10 min (6 min–12 max) and the mean temperature reached was 80°C (67°C min–94°C max). All study patients underwent a single session of RFA as the tumor size of our patients did not exceed 3.5 cm, the maximal tumor size that can be completely ablated in one session by a single electrode needle insertion.
The mean±SD follow-up duration was 22.1 ± 13.7 months. During the follow-up period, three patients (9.4%) were diagnosed with residual disease; of these patients, one was characterized as primary treatment failure and two as local disease progression (mean time to progression 15 ± 12.7 months). Therefore, primary technical success was 97.0% and primary technique effectiveness over the follow-up period was 90.6%. All three patients diagnosed with residual disease underwent repeat RFA, but data from repeat ablations were excluded from the present analysis.
Figure 1 presents the overall cumulative incidence of residual tumor detected at the site of RFA. A significant association was revealed between the RENAL nephrometry score classification and cumulative incidence of residual tumor at the ablation site (p = 0.002) (Figure 2). All patients were alive at the time of study data analysis with no metastases diagnosed.

Residual tumor-free survival in study patients.

Residual tumor-free survival in study patients according to RENAL classification.
During the postprocedure 90-day follow up, no major complications were observed. Three minor complications were recorded: two perinephric hematomas not requiring intervention (Clavien grade I) and one case of urinary tract infection managed with antibiotic treatment (Clavien grade II). With regard to the impact of the RFA procedure on renal function, no difference was found in serum creatinine levels and eGFR pre and 3 months post procedure (p > 0.05).
Discussion
According to current clinical guidelines, surgical excision of cT1 renal tumors remains the gold standard treatment approach, with nephron-sparing techniques being highlighted, as they offer disease control and preservation of renal function in comparison to radical nephrectomy [Campbell et al. 2009; Ljungberg et al. 2010]. However, surgical intervention can be challenging, and sometimes impossible, in high-risk patients with significant comorbidities. Thus, alternative ways of management of renal masses have been introduced, such as RFA or cryotherapy, that combine local disease control and minimally invasive techniques in an effort to effectively overcome surgery-associated morbidity and mortality [Klatte et al. 2014; Sun et al. 2012]. RFA, either ultrasound or CT guided, has been used as nephron-sparing treatment for small renal tumors, with growing literature presenting acceptable oncologic and functional outcomes in selected patients.
The experience of ultrasound-guided RFA for cT1a renal masses performed by urologists is presented in the current study. According to our findings, RFA, in relation to mid-term results, seems to effectively offer oncological control for renal masses up to 3.5 cm, without compromising patients’ safety and renal function. Also in the present study, renal masses of intermediate complexity, based on RENAL nephrometry score assessment, seem to have shorter time to recurrence, in comparison with low-complexity masses.
In our study, with median follow up of 24 months, 91% of enrolled patients had no recurrence of disease, while complete ablation after the first session of RFA was achieved in 97% of patients. While the study follow-up time is relatively short, a recent report by Iannuccilli and colleagues on 14-year experience of RFA has demonstrated that the majority of recurrences were detected within the first 24 months after the procedure, with a significant number being diagnosed within the first 3 months after RFA sessions [Iannuccilli et al. 2015]. These long-term findings further confirmed the previously shown bimodal pattern of residual tumor diagnosis over the follow-up period [Ferakis et al. 2010; Levinson et al. 2008; Varkarakis et al. 2005]. Nevertheless, several reports of mid- and long-term outcomes of ultrasound- or CT-guided RFA for renal masses have shown excellent oncological outcomes, with recurrence-free and cancer-specific survival rates exceeding 90% [Chang et al. 2015; Hiraoka et al. 2009; Iannuccilli et al. 2015; McClure et al. 2014; Psutka et al. 2013; Takaki et al. 2010; Thompson et al. 2015].
The complexity of renal masses, as depicted by RENAL nephrometry score, was shown to correlate with the time to recurrence. Specifically, patients with intermediate renal masses had shorter time to recurrence in comparison with those diagnosed with renal masses of low complexity. A previous study by Schmit and colleagues on renal mass ablation showed a significant association between the RENAL score classification and overall local treatment failure, with high-complexity tumors having the highest rate of local recurrences compared with low- and intermediate-complexity lesions [Schmit et al. 2013]. However, criticism on this study focused on the lack of differentiation between RFA and cryoablation techniques. Recently, Gahan and colleagues proposed a modification in RENAL nephrometry score, and specifically to the size variable, to increase its performance on predicting the outcomes of ablation procedures [Gahan et al. 2015]. In Gahan’s study, high-complexity tumors again seem to be more likely to fail than low- or intermediate-complexity tumors. However, none of our patients had high-complexity lesions according to the standard RENAL score. It has to be mentioned though that one out of the three patients with disease recurrence in our study would be reclassified as having a high-complexity tumor if the modified RENAL score was applied.
According to our results, no major complications occurred, both intra- and postoperatively. A low 90-day rate of minor complications is presented, which can be attributed, to a degree, to the solitary and small size tumors as defined by the highly selective inclusion criteria of our study. It has to be noted, however, that all percutaneous procedures were performed under ultrasound guidance by urologists, instead of CT guidance by radiologists, and under local anesthesia rather than sedation, in a sample of patients with significant comorbidities. At the same time, no difference was found with regard to renal function before and after all RFA sessions in study patients, indicating that the procedure had no impact on renal function and can indeed be regarded as nephron sparing. Similar results of preservation of renal function have been shown, even in patients with solitary kidneys undergoing RFA for renal tumors [Hoffmann et al. 2010; Levinson et al. 2008; Olweny et al. 2012].
Apart from the patients included in the protocol and analyzed in the present study, special mention has to be made on seven additional patients diagnosed with renal masses, but with a negative biopsy result. The limitations of the percutaneous biopsy procedure for renal masses were discussed with the patients and their relatives. Five patients decided to follow an active surveillance protocol with an indication for a repeat biopsy if any evidence of progression was noted. The remaining two patients chose to have a repeat biopsy; both patients received a second negative result and similarly entered a surveillance protocol. To date, all seven patients remain stable, without any indications for radiographic or clinical progression of the lesions.
Study limitations include its retrospective design, the relatively low number of patients recruited resulting in few patients with recurrences, the relatively short follow up and the fact that only cT1a tumors were managed with percutaneous RFA. At the same time, however, this study presents satisfactory oncological and functional results for patients who were unfit for surgery and managed exclusively by urologists using ultrasound for guidance, widely available in urological departments, and under local anesthesia instead of sedation. Moreover, a subjective evaluation and standardized stratification of complexity of all renal lesions is presented using the RENAL nephrometry score.
Conclusion
The current study findings show that percutaneous RFA of small renal cell tumors using exclusively ultrasound-based guidance under local anesthesia can be an effective method for managing patients who are unfit for surgery. Mid-term oncological results were satisfactory, the safety profile of the procedure was acceptable and adequate preservation of renal function was obtained. Patients with intermediate complexity of renal lesions according to RENAL nephrometry score had shorter time to recurrence in comparison to those with low-complexity masses. Nevertheless, further studies with larger numbers of patients are needed to verify our results.
Footnotes
Acknowledgements
Mr Christos Zacharis provided technical assistance during the procedures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.