
Abstract
Objective
To compare the efficacy of two different treatment approaches for auricular pseudocyst.
Methods
This retrospective study reviewed data from patients with auricular pseudocyst that were treated with either anterior wall resection plus radiofrequency ablation compression (surgical group) or simple aspiration and compression suturing (control group). The following outcomes were compared between the two groups: therapeutic response (cure, good or none), duration of postoperative medication (antibiotics) use, duration of postoperative pain, duration of recovery of appearance and rate of complications (infection, auricular thickening, incision swelling and recurrence).
Results
A total of 386 patients were enrolled in the study: 218 in the surgical group and 168 in the control group. Duration of postoperative medication use, duration of postoperative pain, duration of recovery of appearance and rate of postoperative complications were significantly lower in the surgical group compared with the control group. The overall therapeutic response (cure and good response) was significantly greater in the surgical group than in the control group.
Conclusion
Auricular pseudocyst can be effectively treated by both of these methods, but anterior wall resection plus radiofrequency ablation compression might be more effective.
Introduction
Auricular pseudocyst, also known as perichondritis of the auricle, is one of the most common otological diseases. 1 Patients with auricular pseudocyst present with a focal noninflammatory cystic swelling on the pinna. The cystic mass is often filled with yellowish or colourless fluid.2,3 Several approaches have been suggested to treat auricular pseudocyst, such as physical therapy, intracystic drug injection, aspiration, gypsum-based compression and anterior wall resection.1–4 Inappropriate treatment may cause infection and serious cosmetic complications. 5
This present study retrospectively compared the therapeutic outcomes of patients with auricular pseudocyst that were treated with either anterior wall resection plus radiofrequency ablation compression or simple aspiration and compression suturing.
Patients and methods
Patient population
This retrospective study reviewed data from consecutive outpatients with auricular pseudocyst that were treated at the Department of Otolaryngology, Head and Neck Surgery, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi Province, China between March 2010 and March 2018. All of the patients presented with evident outer-ear swelling affecting either the scaphoid or the triangular fossa of the ear. Patients had either undergone anterior wall resection plus radiofrequency ablation compression (surgical group) or simple aspiration and compression suturing (control group). All patients had not been treated with other methods.
This study was approved by the Institutional Human Experiment and Ethics Committee of the Second Hospital Affiliated to Xi’an Jiaotong University, Xi’an, Shaanxi Province, China (no. 2013-142). Written informed consent was obtained from each patient.
Study treatment
For the surgical group that underwent anterior wall resection, patients were placed in the supine position with the affected ear facing up. After disinfection of the cystic auricular lesions, local anaesthesia was performed with 1% lidocaine for 5 min. An incision was made on the top surface of the auricular cyst, which was followed by dissection of the subcutaneous tissue. The anterior cartilage was exposed. After drainage, the floating cartilage was excised. Radiofrequency ablation of cystic lesions was carried out (EVAC◊ 70 XTRA HP COBLATION Wand; Arthrocare Corporation, Austin, TX, USA). After removal of the involved tissues, interrupted suturing of the incision was undertaken (Figure 1). The surgical area was covered with a pressure bandage for 3 days. Oral administration of antibiotics was given to each patient for 7 days postoperatively (500 mg clarithromycin orally once a day).

Representative photographs showing the surgical procedure used in patients with auricular pseudocyst that were treated with anterior wall resection plus radiofrequency ablation compression (surgical group): (a) preoperative appearance of the ear; (b) intraoperative procedure; (c) postoperative appearance of the ear showing the sutures. The colour version of this figure is available at: http://imr.sagepub.com
For the control group that underwent simple aspiration and compression suturing, a 5-ml syringe was inserted at the low point of the most obvious bulge of the cyst to facilitate drainage. The front and back of the auricle were padded with oil gauze and the pseudocyst area was sutured using a U-shaped suture of line 0 and pressurized through the whole auricle layer. The front and back capsule walls were closely compressed so that there was no residue. Oral administration of antibiotics was given to each patient for 7 days postoperatively (500 mg clarithromycin orally once a day). The dressing was changed the next day and the suture was removed 8–10 days after the procedure.
Therapeutic outcomes
The duration of postoperative medication administration (i.e. oral administration of antibiotics) was recorded for all study participants. The pain levels were recorded once daily using a visual analogue scale (0–10) for 10 days. The rate of complications (infection, auricular thickening, incision swelling and recurrence) was determined for 1 year. In terms of therapeutic response at 1 year, a clinical cure was defined as complete resolution of the clinical symptoms and signs; a good response was defined as a substantial reduction in the size of the cyst; and no response was defined as no shrinkage of the cyst and thickening of the auricle that resulted in auricle deformity. The overall response (OR) rate was calculated using the formula: OR = (patients with a cure + patients with a good response)/total cases × 100%.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 16.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Data are presented as mean ± SD and n of patients (%). A Wilcoxon rank sum test was used to compare the therapeutic response between the two groups. The duration outcomes were compared using the Student’s t-test. The rate of postoperative complications and recurrence were compared using χ2-test. A P-value < 0.05 was regarded as statistically significant.
Results
This retrospective study reviewed the data from 386 patients with auricular pseudocyst: 218 patients underwent anterior wall resection plus radiofrequency ablation compression (surgical group) and 168 underwent simple aspiration and compression suturing (control group). The overall study cohort had a mean ± SD age of 39 ± 9.1 years (range, 20–68 years). There was no statistically significant difference in age and sex distribution between the two groups. The duration of postoperative medication administration, duration of pain and duration of the recovery of appearance of the ear were significantly lower in the surgical group than in the control group (P < 0.001 for all comparisons; Table 1).
Comparison of treatment-related outcomes in patients with auricular pseudocyst that were treated with either anterior wall resection plus radiofrequency ablation compression (surgical group) or simple aspiration and compression suturing (control group).
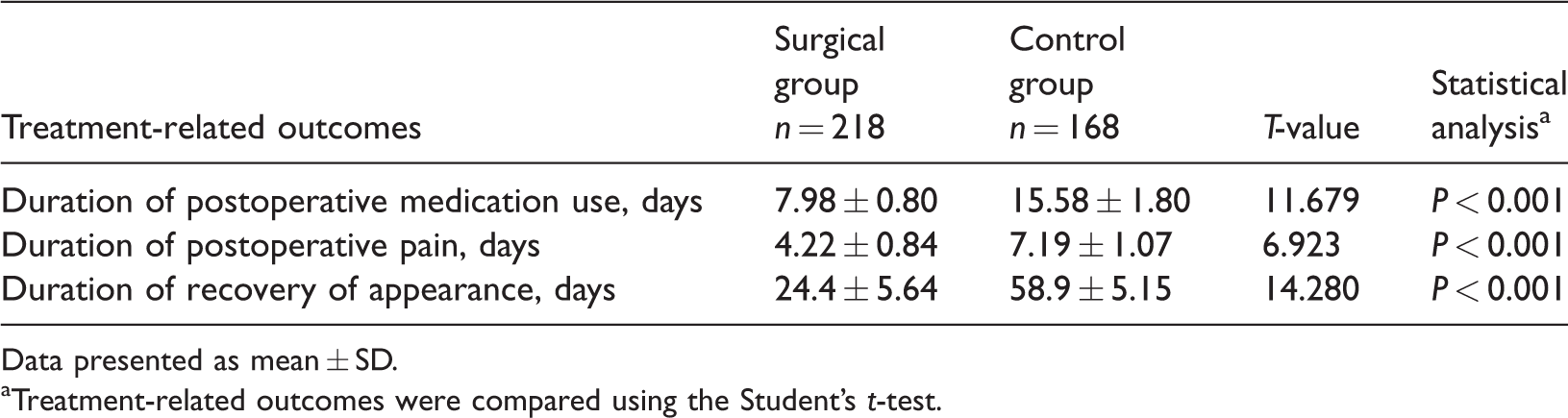
Data presented as mean ± SD.
aTreatment-related outcomes were compared using the Student’s t-test.
In terms of therapeutic response, the overall response rate was 99.08% (216 of 218 patients) in the surgical group compared with 84.52% (142 of 168 patients) in the control group (P < 0.05; Table 2).
Comparison of therapeutic outcomes in patients with auricular pseudocyst that were treated with either anterior wall resection plus radiofrequency ablation compression (surgical group) or simple aspiration and compression suturing (control group).

Data are presented as n of patients (%).
Overall response rate was calculated using the formula: OR = (patients with a cure + patients with a good response)/total cases × 100%; P < 0.05 for between group comparison using Wilcoxon rank sum test.
The rates of postoperative complications and recurrence were significantly reduced in the surgical group compared with the control group (P < 0.001 for all comparisons; Table 3).
Rates of postoperative complications in patients with auricular pseudocyst that were treated with either anterior wall resection plus radiofrequency ablation compression (surgical group) or simple aspiration and compression suturing (control group).

Data are presented as n of patients (%).
aBetween-group comparisons were undertaken using χ2-test.
Discussion
Auricular pseudocyst frequently occurs in adult males. 6 It has been suggested that auricular pseudocyst is caused by damage to the auricular cartilage. 7 However, the pathogenesis of this disorder remains unclear. Abnormal embryonic development may result in an unlined intracartilaginous cavity, consequently leading to pseudocyst of the auricle. 6 Alternatively, auricular pseudocyst may result from microvascular obstruction secondary to mechanical injury of the ear. 8 Treatment options for auricular pseudocyst include physical therapy, intracystic drug injection, aspiration, gypsum-based compression and anterior wall resection.1–3,7,9 The goal of the treatment of auricular pseudocyst is to recover the normal anatomic morphology of the auricle and to prevent recurrence. Auricular pseudocyst can be treated via multiple punctures and aspiration of the fluid; or an incision can be made over the cyst and the fluid then drained. 10 , 11 Although external application of drugs and cryotherapy may not cause traumatic injury, these therapies are time-consuming and have limited therapeutic efficacy. 12 Simple aspiration therapy is associated with high recurrence and severe complications such as cartilage hyperplasia and infection. 13 Therefore, more effective therapies are needed to treat auricular pseudocyst.
Previous pathological analysis demonstrated that the fluid in the auricular pseudocyst was mainly derived from the inflammatory perichondrium. 14 The outer perichondrium gets thicker and induces cartilage synthesis. 4 The cyst is composed of newly synthesized cartilage, auricular cartilage and fluid. 15 When the perichondrium differentiates into cartilage, the leakage of fluids from the perichondrium is terminated. 14 The adhesion between newly synthesized cartilage and auricular cartilage may cause auricular thickening and deformation. 14 Although the surgical treatment of auricular pseudocyst has a reduced rate of recurrence rate simple aspiration therapy, this therapy may incur traumatic injury and increase the risk of infection and aural deformity.16–18
There are several causes for the recurrence of auricular pseudocyst, including incomplete disruption of the cyst wall, residual fluid and partial adhesion between the cyst walls. 19 This current retrospective study compared the therapeutic efficacy of surgery and simple aspiration in treating auricular pseudocyst. In the control group, a U-shaped suture was used to keep an appropriate level of pressure to avoid the formation of an interspace that might lead to infection and delayed healing. Due to a poor blood supply, the duration of fibrosis and exudate absorption are much longer in cartilage than that in soft tissue, which results in a longer duration of wood healing and pain, and a larger incidence of postoperative complications. 17 In the current study, the use of anterior wall resection plus radiofrequency ablation compression showed significantly better therapeutic responses compared with simple aspiration and compression suturing. The surgical group had a significantly lower duration of postoperative medication use, duration of postoperative pain and postoperative duration of recovery of appearance compared with the control group. Moreover, the rate of recurrence was significantly decreased in the surgical group (4.59%) compared with the control group (17.86%). The rate of the other postoperative complications, infection, auricular thickening and incision swelling, were significantly decreased in the surgical group compared with the control group. The better therapeutic outcomes observed in the surgical group might have been due to the use of radiofrequency ablation, which can coagulate targeted tissues, occlude blood vessels, stimulate fibrosis and destroy the source of serous exudation. Also, radiofrequency ablation has the advantages of minimal trauma and rapid healing. 20
This study had several limitations. First, the limited number of patients might have affected the statistical significance and more participants should be enrolled to verify the effectiveness. Secondly, the follow-up duration was short and a longer follow-up is required in future studies.
In conclusion, simple compression treatment after aspiration was able to establish a complete adhesion between the cyst walls in patients with auricular pseudocyst. However, this therapy was associated with prolonged healing duration and pain and an increased risk of postoperative complications compared with surgical treatment combined with radiofrequency ablation. In contrast, surgical treatment combined with radiofrequency ablation significantly shortened the recovery time and reduced the rate of recurrence and postoperative complications. Therefore, these findings suggest that the surgical strategy combined with radiofrequency ablation might be safer and more effective than the simple aspiration technique for treating auricular pseudocysts. Further research with larger study populations is needed to confirm these findings.