
Abstract
Colorectal cancer is the third most common cancer in the Western population and has a 5-year overall survival of 5–10% when metastatic. Approximately 30% of the patients with metastatic colorectal cancer have limited disease apparently isolated to the liver and, if this can be resected, the 5-year overall survival is improved to 30–60%. Therefore, it is important to identify patients who have both resectable disease and those with initially unresectable tumors who can potentially be downsized with chemotherapy to allow resection. First-line doublet chemotherapy regimens lead to response rates of 50–60%, triplet chemotherapy regimens may result in a response rate of up to 70%, and biological agents may add to responses or induce morphologic changes that facilitate disease resection. Surgical advances in recent years have also increased resectability rates and have challenged prior rules of resectability. Local therapies including ablation and radiation, often performed in conjunction with resection, may further aid in control of disease. The aim of this article is to focus on the role of neoadjuvant therapy in the treatment of colorectal liver metastases.
Keywords
Introduction
Colon cancer is the third most common cancer in the United States and is responsible for approximately 50,000 deaths annually [Siegel et al. 2011]. A total of 20% of patients with colorectal cancer present with metastatic disease and around 25–30% of them have isolated liver metastases at the time of diagnosis (see Figure 1). The prognosis for metastatic colorectal cancer has significantly improved in the past 10–15 years with more effective surgical approaches and more efficacious chemotherapy regimens rendering more patients surgical candidates [Kopetz et al. 2009].
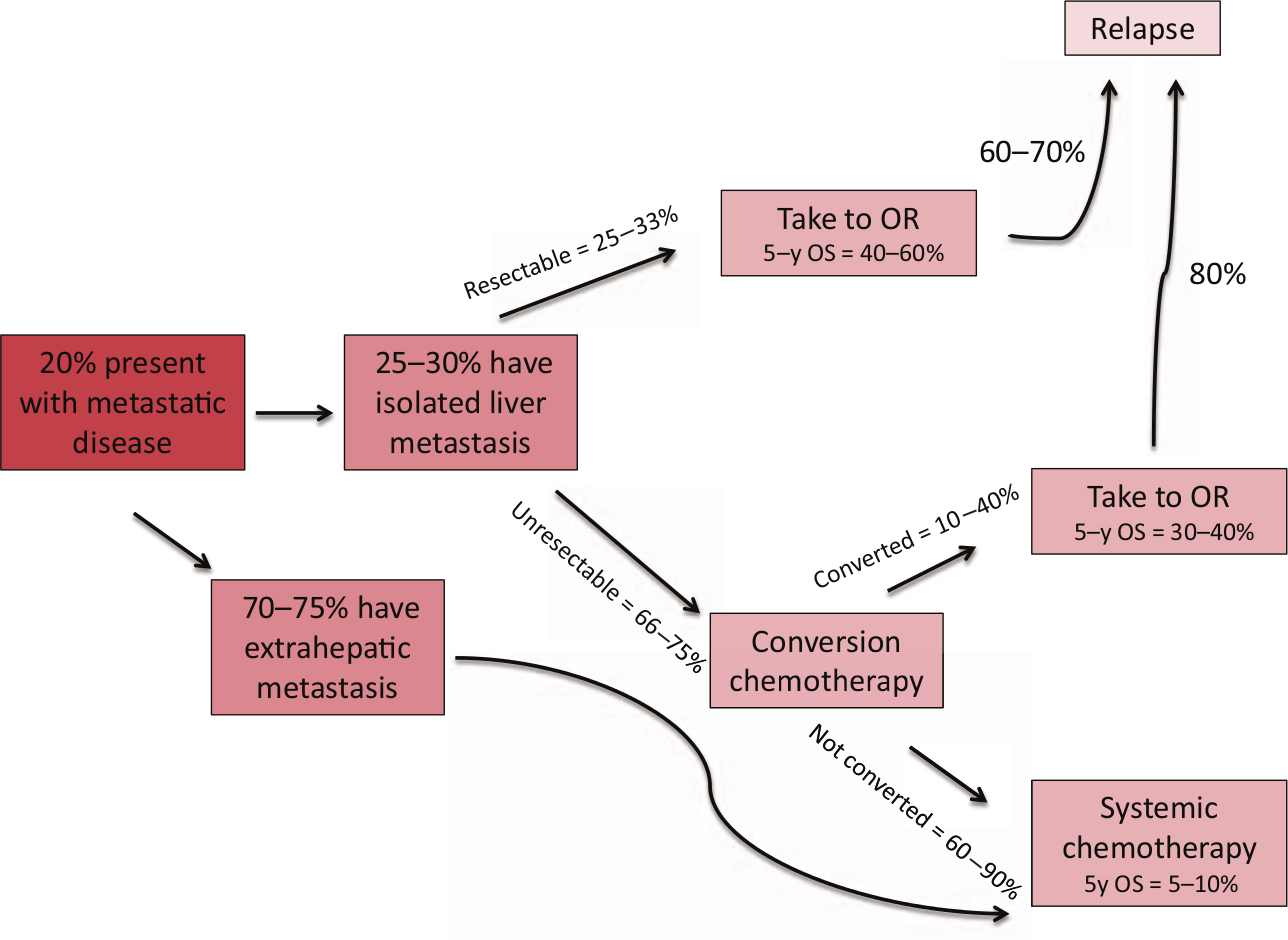
Expected outcomes for patients presenting with metastatic colorectal cancer.
Chemotherapy can now convert unresectable colorectal liver metastasis (CLM) into resectable disease (conversion chemotherapy) and prior ‘rules of resectability’ have been challenged. This has increased resectability rates from 10–15% up to 20–30% with 5- and 10-year overall survival (OS) of about 33% and 23%, respectively [Adam et al. 2004a]. Patients who undergo liver resection and survive beyond 10 years appear to be cured in almost all cases [Tomlinson et al. 2007]. Hepatic resection has therefore become the treatment of choice for patients with CLM whenever it is feasible. As a comparison, patients with metastatic disease who do not undergo surgery have a 5-year OS of about 10% [Sanoff et al. 2008]. Although prognosis has improved, up to 75% of patients do eventually have recurrence of disease [Nordlinger et al. 1996] and so new ways of both predicting and improving outcome are being explored. Local liver-directed therapies are also available including radiofrequency ablation (RFA), radioactive yttrium90 microspheres (SIR-spheres), hepatic intra-arterial chemotherapy (HAI) and transarterial chemoembolization but these modalities have not been shown to improve OS.
Who is resectable?
One of the more important determinants of OS following hepatic resection of isolated CLM is negative surgical margins (R0 resection) [Adam et al. 2010a; Pawlik et al. 2005] and so surgery is not considered when the surgeon believes that this cannot be achieved. In such cases, chemotherapy to convert the disease into resectable disease should be strongly considered (see the section on ‘Conversion chemotherapy in unresectable liver metastasis’). It should be noted that in an era of more effective chemotherapy regimens and local therapies directed at a positive margin, a resection with a positive margin(R1 resection) may not be detrimental to the patient’s care. In a study by de Haas and colleagues, patients with R1 resections had more intrahepatic recurrence than patients with R0 resections but 5-year OS was not vastly different (57% versus 61%) with 88% and 78% receiving postoperative chemotherapy in the two groups [de Haas et al. 2008].
A number of other factors need evaluation including how much of the liver will remain (future liver remnant [FLR]) and the functional status of the FLR. If patients have been heavily pretreated with chemotherapy or have underlying liver disease, a liver biopsy may be prudent to evaluate the histopathological features of the FLR. Resection should only be undertaken if at least 25–30% of functional hepatic parenchyma will remain after resection, but in case of underlying liver disease or prior chemotherapy, 30–40% of remaining functional parenchyma is needed [Abdalla et al. 2006]. Furthermore, at least two disease-free liver segments with viable vascular inflow, outflow and biliary drainage should be left behind. Major risk factors associated with postoperative liver failure include age >70 years old, cirrhosis, fibrosis, hepatitis, steatosis, preoperative chemotherapy, obstructive cholestasis and intraoperative blood loss or ischemia [Clavien et al. 2007]. Portal vein embolization (PVE) can induce an increase of up to 50% in size in the nonembolized lobe over 4–6 weeks and can help increase the resectability rate in initially unresectable tumors where the FLR is initially believed to be too small to maintain adequate liver function [Wicherts et al. 2010]. Not only does PVE function to increase the size of the FLR prior to resection, it can serve as a test of the liver’s ability to regenerate prior to major hepatectomy.
Surgical case series generally report 5-year OS rates between 25 and 60% with <5% surgical mortality. However, a population-based retrospective cohort of 3957 US Medicare enrollees who underwent hepatic resection had a 5-year OS of 25% [Robertson et al. 2009], emphasizing the fact that selection of patients is important but also revealing that older patients can benefit from surgery as the 5-year OS in that cohort is longer than when chemotherapy is given alone. One study looking at liver surgery for CLM in the elderly (>70 years old) reported a slightly higher mortality rate (3.8% versus 1.6%) and postoperative complication rate (15.9% versus 12.5%) compared with patients <70 years old. While patients need to be selected carefully in this group, they should not be excluded from potentially curative or life extending intervention solely on the basis of age [Adam et al. 2010b].
The following criteria are generally considered to be contraindications to hepatic resection: Extensive unresectable extrahepatic disease (EHD), involvement of contralateral portal structures (e.g. hepatic artery, major bile ducts or main portal vein), celiac/aortic lymph node involvement, >70% liver involvement (or more than six involved segments or involvement of all three hepatic veins) or inadequate postresection functional reserve [Adam et al. 2008]. Although investigators initially believed that a margin of >1 cm was associated with lower recurrence rates, this has been disproven in more recent years [Pawlik et al. 2005].
Clinical risk scores were developed in the past to try to determine which patients would benefit most from surgery. Factors with significant negative predictive value for OS included <12 months from primary resection to development of liver metastasis, >1 liver tumor, node-positive primary, hepatic tumor >5 cm and carcinoembrionic antigen (CEA) level >200 ng/ml. Five-year OS was 40% if none of these was present and fell to 16% if all of them were present [Fong et al. 1999]. Other prognostic risk score models have included negative margins and size of the largest metastasis (>5 cm) as predictors of survival [Nordlinger et al. 1996]. These are, however, of limited benefit today when choosing patients for surgery as they were created before the era of neo-adjuvant chemotherapy regimens.
Extrahepatic disease
A review of 171 patients with EHD who underwent resection of both liver metastases and EHD with curative intent revealed a significant 5-year OS difference (26% compared with 58% for those without EHD) and a recurrence rate of 85%. Patients with aortocaval lymph node involvement had the worst OS compared with other EHD sites [Pulitanò et al. 2011]. A recent retrospective review of 840 resected patients of whom 185 patients had resectable EHD attempted to identify prognostic factors to help with selection of patients with EHD for surgery. Five-year OS was 55% in isolated CLM patients compared with 28% in patients with resected EHD. Five poor prognostic factors were identified on a multivariate analysis: location other than lung metastases, EHD concomitant with CLM recurrence, CEA >10 ng/ml, at least 6 CLM lesions and right-sided colon cancer. Five-year survival ranged from 64% (with no factors) to 0% (with >3 factors). Patients in the EHD group with recurrence had a slightly better outcome at 5 years when resected compared with giving chemotherapy only (38% versus 21%, p = 0.05) [Adam et al. 2011]. So patients need to be selected carefully for surgery if they have evidence of EHD.
Primary lesion in place
If patients present with synchronous CLM, the traditional approach has been to give neoadjuvant chemotherapy to ‘select’ patients for surgery who have clinical responses and to avoid unnecessary liver resection in aggressive disease. This has recently come into question as studies have shown that, in the hands of an experienced surgeon, there is acceptable morbidity from these simultaneous resections and assessment of response via clinical imaging obtained while on chemotherapy does not necessarily predict pathological responses [Benoist et al. 2006; Reddy et al. 2009]. Studies have shown simultaneous resections to be as safe as staged resections with fewer days spent in the hospital [Martin et al. 2009; Reddy et al. 2007]. Major hepatectomy independently predicted severe morbidity after simultaneous resections [Reddy et al. 2007], so a two-staged approach should be considered in cases of large liver resection such as trisegmentectomy.
How to evaluate responses and resectability
Choosing the type of imaging and methods to evaluate responses to chemotherapy can have an impact on the decision of whether or not to take a patient to surgery and therefore warrants some discussion. A meta-analysis of 39 articles published from 1990 to 2010 with 3391 patients showed computed tomography (CT), magnetic resonance imaging (MRI) and 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) to have sensitivities of 83.6%, 88.2% and 94.1%, respectively, on a per patient basis with MRI being more sensitive in evaluating lesions <10 mm than CT. Specificity estimates were comparable [Niekel et al. 2010]. FDG-PET is useful in evaluating EHD and is only recommended in the workup of potentially surgically curable M1 disease in the National Comprehensive Cancer Network (NCCN) guidelines [NCCN, 2013]. CT and/or MRI are used to monitor disease responses. Ultrasound can be useful for intraoperativestaging to help in determining resectability. Contrast-enhanced ultrasound has been shown to reveal more lesions than conventional ultrasound as the echoic nature of lesions in the portal/delayed phase can both reveal lesions <1 cm and help determine whether they are malignant versus benign. It was found to improve the sonographic accuracy in 13.7% of cases in a study of 82 patients undergoing liver resection [Chami et al. 2008].
When determining whether unresectable patients have responded to chemotherapy, targeted therapies can induce different types of responses to the accepted predefined size-based criteria of Response Evaluation Criteria in Solid Tumors (RECIST) that would be expected with cytotoxic chemotherapy. The RECIST criteria, while reproducible as a means of assessing response are arbitrary, and it is unclear that a 30% reduction correctly represents a response in circumstances in which targeted agents are used. Biological agents such as vascular endothelial growth factor (VEGF) inhibitors can cause morphological changes to the tumor when given with cytotoxic chemotherapy. The commonly observed changes in tumor texture and margins include a heterogeneous ill-defined solid mass becoming a sharp, homogeneous hypoattenuating mass. Such morphological criteria did correlate better with response to chemotherapy and OS than more traditional size-based RECIST criteria in a single study [Chun et al. 2009], but these findings have yet to be validated. Changes in the radiographic characteristics of lesions induced by chemotherapy can therefore be misleading at times and even in the absence of targeted agents, as demonstrated in a case report of a patient who had a reduction in the size of the primary lesion and CEA levels after three courses of 5-fluorouracil (5-FU) and oxaliplatin (FOLFOX) while liver lesions grew in size and number. Therapy was continued and a month later the liver lesions had decreased in size and the patient continued to have a response for 12 months after therapy initiation [Shah and Goldberg, 2008]. Of note, patients who obtain a complete response on imaging after receiving preoperative chemotherapy are still likely to benefit from resections to achieve optimal outcomes as 83% are found to have residual microscopic disease [Benoist et al. 2006].
Neoadjuvant chemotherapy in resectable liver metastasis
It is still controversial whether there is any advantage to delivering chemotherapy before resection of liver metastases that are judged to be initially resectable. The EORTC 40983 study is the only reported phase III trial randomizing patients who were considered to have resectable disease to perioperative chemotherapy and surgery versus surgery alone. A total of 364 patients with a maximum of four liver metastases were randomized to surgery alone or to surgery with six cycles each of preoperative and postoperative 5-FU and oxaliplatin (FOLFOX4). Absolute progression-free survival (PFS), the primary endpoint, was increased significantly in the chemotherapy group by 9.2% in all resected patients (p = 0.025), but the PFS curves paralleled each other after a fallout of 9% of patients immediately following surgery suggesting that the 9% increase was due to patients who were not good operative candidates. A total of 84% of the patients completed the preoperative chemotherapy regimen while 76% of the resected patients completed the postoperative chemotherapy regimen. Preoperative chemotherapy caused a median decrease in size of liver metastases of 30% and 43% of the patients had an objective response (3% complete response, 40% partial response), while 7% of patients progressed on preoperative chemotherapy. Postoperative complications were higher in the chemotherapy group (25% versus 16%, p = 0.04) but did not affect postoperative mortality rates [Nordlinger et al. 2008]. A recent update on the trial reported that the OS after a median follow up of 8.5 years was not significantly different between the two groups with a 5-year OS of about 50% in both groups [Nordlinger et al. 2012]. An exploratory retrospective analysis of possible predictive factors only identified CEA >5 ng/ml as a predictive factor for better outcomes with perioperative chemotherapy leading to a 3-year PFS of 35% with perioperative chemotherapy compared with 20% with surgery alone [Sorbye et al. 2012]. This trial did not therefore show a significant difference in OS when patients with resectable liver metastasis were given perioperative chemotherapy and remains the only published randomized trial addressing this issue. No studies to date have looked specifically at VEGF or epidermal growth factor receptor (EGFR) targeted therapies in patients with initially resectable CLM.
Adam and colleagues looked retrospectively at 1471 patients with single metachronous liver metastasis, 169 of whom had received preoperative chemotherapy and 1302 who did not. The R0 resection rates were similar in the two groups and OS at 5 years was 60% for both patient groups. Receiving preoperative chemotherapy did not impact survival but factors significantly affecting survival in a negative manner on a multivariate analysis included age >70 years old, lymph node positivity in the primary tumor, a primary-to-metastases time delay of less than 12 months, raised CEA levels >5 ng/ml at diagnosis, tumor >5 cm, noncurative liver resection and absence of postoperative chemotherapy. Postoperative chemotherapy significantly improved OS in patients with liver metastasis >5 cm (OS at 5 years 58% versus 33%,p < 0.01). They concluded that preoperative chemotherapy should not be given to resectable patients and that postoperative chemotherapy should only be given to patients with unfavorable characteristics such as large tumors [Adam et al. 2010a].
Besides one randomized controlled trial and a large retrospective study looking at preoperative chemotherapy in resectable CLM, there have been a few single-arm studies with small numbers of patients with upfront resectable CLM who receive neoadjuvant chemotherapy. They all report high resection rates (>85%), and a correlation between imaging responses and OS is usually seen [Bathe et al. 2009; Chiappa et al. 2009; Gruenberger et al. 2008]. In a study by Bathe and colleagues, 5-fluorouracil/irinotecan (FOLFIRI) was given pre- and postoperatively with 7 out of 35 patients progressing on preoperative chemotherapy; 4 were therefore not taken to surgery [Bathe et al. 2009]. There is a concern about missing the window of opportunity by giving neoadjuvant chemotherapy to patients when it is not clearly needed to accomplish an R0 resection. Even though doing so might reveal tumors with aggressive features, patients who progress on chemotherapy and are resected still have longer OS than those who are not resected. We would therefore not favor pre-operative chemotherapy in resectable patients with ≤4 liver metastasis if the tumor locations were favorable to resection.
The LiverMetSurvey, an international, internet-based registry to assess outcomes of patients who undergo operations for CLM, was accessed and analysed in a recent review article showing a marked difference in survival depending on the type of response patients had to preoperative chemotherapy. Five-year survival was 62%, 48%, 44% and 29% in 4581 patients who had complete response, partial response, stable disease and progressive disease, respectively [Adam et al. 2012]. Although patients who had progressive disease derive less benefit from surgery, their 5-year OS is still better than that seen in patients getting chemotherapy alone for metastatic disease (10%) [Sanoff et al. 2008]. OS probability in patients who are initially considered resectable versus those who are not but later become resectable is not vastly different, emphasizing the fact that surgery should be pursued when possible. The LiverMetSurvey showed a 5-year OS of 46% in initially resectable patients versus 33% in initially unresectable patients with 10,940 patients followed [Adam et al. 2012].
It is less clear what to do for patients with >4 liver metastases as these patients were not included in the EORTC 40983 trial. Adam and colleagues studied 131 patients with ≥4 liver metastasis, some resectable upfront but others not (numbers of resectable versus unresectable patients were not reported in the article). Patients who had a response (>50% reduction in size of tumors) or stable disease (<25% increase to <49% decrease in size) had a significantly better median OS compared with patients with progression (>25% increase in size) with 5-year OS being 37%, 30% and 8% in the three groups, respectively. This was irrespective of the type of treatment as demonstrated in a multivariate analysis but tumor progression on preoperative chemotherapy, number of resected metastases, elevated preoperative CA 19-9 level and number of lines of chemotherapy had a significant impact on survival. Some patients achieved responses with second or third line chemotherapy indicating that surveillance and continuous evaluation of resectability of liver disease is important [Adam et al. 2004b]. Based on this study, one might consider giving preoperative chemotherapy to patients with ≥4 liver metastasis and abort plans for surgery if progression is noted as these patients had a 5-year OS of 8%, which is no better than when chemotherapy is given alone.
Preoperative chemotherapy can cause liver toxicities and therefore potentially limit the resectability of tumors and increase the chance of postoperative complications including liver failure. 5-FU chemotherapy has been associated with steatosis. Irinotecan-based therapy has been associated with an increased incidence of steatohepatitis and an increased 90-day mortality in one study [Vauthey et al. 2006]. Oxaliplatin exposure is associated with an increased risk of vascular damage such as sinusoidal dilatation [Rubbia-Brandt et al. 2004] and hepatic fibrosis [Adam et al. 2010a] but these did not lead to increased mortality [Aloia et al. 2006; Vauthey et al. 2006]. More than 12 courses of chemotherapy hasbeen associated with longer hospitalization, higher rates of reoperation [Aloia et al. 2006] and increased postsurgical complications [Karoui et al. 2006]. The number of preoperative chemotherapy cycles should therefore be limited to 12 weeks or less where possible. An interval of less than 4 weeks between chemotherapy and resection has also been associated with increased complication rates [Welsh et al. 2007], so we favor waiting 6–8 weeks after stopping chemotherapy before taking patients to surgery.
Postoperative chemotherapy is commonly used although it has not been clearly shown to improve survival, likely partly due to poor accrual to trials and published trials using outdated chemotherapy regimens. Two randomized trials (both closed prematurely due to poor accrual) showed better median PFS (28 months versus 19 months, p = 0.058) with postoperative chemotherapy compared with observation and a trend towards better survival (62 months versus 47 months, p = 0.095) in a combined analysis of both trials [Mitry et al. 2008]. In a trial comparing FOLFIRI with 5-FU/leucovorin (5-FU/LV), there was no significant change in median disease-free survival (22 months versus 25 months) in the 306 patients treated [Ychou et al. 2009]. Similarly, irinotecan has failed to demonstrate a benefit as adjuvant therapy in resected stageII/III colorectal cancer when compared with 5-FU alone. There are no good data on whether to include biological agents in the postoperative chemotherapy regimen. The current NCCN guidelines suggest conventional adjuvant therapy as used for stage II/III disease in patients with resected liver metastasis for a total of 6 months as an option [NCCN, 2013]. However, in patients with prior exposure to oxaliplatin based therapy in the adjuvant setting for stage II or III disease, the potential for the same regimen to make the difference between recurrence and cure of micrometastatic disease left behind after metastasectomy seems limited.
It is our practice that if a patient has synchronous resectable disease (≤4 liver metastasis) and is a good operative candidate, surgery should not be delayed to administer chemotherapy. The role of preoperative chemotherapy is less clear when >4 liver metastasis are detected with no prospective data available to guide decision-making. We tend to administer preoperative chemotherapy for 2–4 months to reveal the biology of the disease and, if no progression is noted, to go ahead with surgery. Chemotherapy should be given postoperatively in an attempt to eliminate any residual microscopic disease in FOLFOX naïve patients as benefits should be analogous to administration of chemotherapy after resection in stage III colorectal cancer.
Conversion chemotherapy in unresectable liver metastasis
Patients who present with metastatic disease isolated to the liver but who are not deemed resectable or are borderline resectable should be considered for conversion chemotherapy to obtain resectability with negative margins (see Figure 2). 5-FU alone rarely provided sufficient reduction in tumor size to allow conversion of unresectable disease to resectable with a response rate of ~20% [Advanced Colorectal Cancer Meta-Analysis Project, 1992]. With new cytotoxic agents approved since 1996, chemotherapy regimens including FOLFOX and FOLFIRI provide objective response rates of 50–60% in patients when given as first-line therapy [Tournigand et al. 2004], four-drug regimens with a combination of 5-FU, leucovorin, oxaliplatin and irinotecan (FOLFOXIRI) provide response rates of 60–70% [Falcone et al. 2007; Ychou et al. 2008] and when bevacizumab is added to that regimen it may be as high as 80% [Masi et al. 2010].

Evaluation and management of a patient with isolated colorectal liver metastasis (CLM).
When comparing trials that report resectability rates in initially unresectable patients, care should be taken to distinguish between trials that include unselected patients and trials that select patients with metastases isolated to the liver [Nordlinger et al. 2010] (see Table 1). Large randomized controlled trials reporting resectability rates in patients receiving first-line therapy for metastatic disease report rates of 3.3–36% [Falcone et al. 2007; Tournigand et al. 2004, 2006], but the cohort of patients who were initially considered eligible for conversion are usually not reported separately and it is therefore difficult to distinguish how effective the regimens are at affecting conversion. In the OPTIMOX-1 trial, about 60% of patients had only one site of disease (70% had liver involvement) on enrollment. FOLFOX was given continuously in arm A (FOLFOX4) and for 3 months in arm B (FOLFOX7) at which point oxaliplatin was stopped but 5-FU/LV maintenance continued. Around 60% had objective responses with 15% and 18% of patients being able to undergo surgery in arm A and arm B, with 9% and 11% having R0 resections, respectively. The patients who underwent R0 resections had improved median survival of 39 and 43 months, while the entire trial cohort had median survival of 19 and 21 months, respectively for arm A and B [Tournigand et al. 2006]. In the N9741 trial, 795 patients were randomized to 1 of 3 regimens, irinotecan/fluorouracil (IFL), FOLFOX4 or irinotecan/oxaliplatin (IROX). About 30% of all patients had isolated CLM disease. Twenty-four patients (3.3%) underwent curative metastatic resection and almost all resected patients had received an oxaliplatin-containing regimen, FOLFOX4 (11) or IROX (11). Median OS in resected patients was 42.4 months compared with 19.5 months and 17.4 months observed in all patients on the FOLFOX4 and IROX arms, respectively [Delaunoit et al. 2005].
Conversion chemotherapy trials for initially unresectable CLM.

In patients who underwent resection; **patients with resected metastases in liver and other sites; ***in FOLFOX7 group, oxaliplatin was stopped after 3 months and reintroduced at progression; ****bilobar disease deemed unresectable in all cases.
CLM, colorectal liver metastasis; FOLFIRI, 5-FU/irinotecan; FOLFIRINOX/FOLFOXIRI, 5-FU/irinotecan/oxaliplatin; FOLFOX4 (5-FU bolus 400 mg/m2 and leucovorin 200 mg/m2 followed by infusional 5-FU 600 mg/m2 over 22 h on days 1-2, oxaliplatin 85 mg/m2); FOLFOX6 (5-FU bolus 400 mg/m2, infusional 5-FU 2400 mg/m2 over 46 h, leucovorin 400 mg/m2, oxaliplatin 100 mg/m2); FOLFOX7 (infusional 5-FU 2400 mg/m2 over 46 h, leucovorin 400 mg/m2, oxaliplatin 130 mg/m2); 5-FU/oxaliplatin; IFL, irinotecan/bolus 5-FU; IROX, irinotecan/oxaliplatin; mo, months; NR, not reported.
Trials with selected patients with unresectable isolated CLM report resection rates of 10–40% following conversion chemotherapy [Alberts et al. 2005; Barone et al. 2007; Ho et al. 2005; Ychou et al. 2008]. They all had a small number of patients (less than 50) and were all single arm trials except for the CELIM trial which compared FOLFOX to FOLFIRI, both given with cetuximab; these two regimens were shown to be equivalent with conversion rates of 60% in both groups [Folprecht et al. 2010].
In both selected and unselected studies, a strong correlation exists between response rates and resection rates [Adam et al. 2004b; Folprecht et al. 2005]. As resection rates are directly related to objective response rates it can be estimated that regimens with higher response rates will lead to higher resection rates in eligible patients. At least 4 courses (treatments) of preoperative chemotherapy should be given with re-evaluation with imaging every 2 months. Trials including selected patients with isolated CLM are hard to design as this patient group can be heterogeneous and require different modulations of therapy including local therapies for positive margins; they are furthermore often limited by slow accrual so it is unlikely that we will see many of these trials designed. Retrospective reviews of patients with isolated CLM have been reported but can clearly be biased both based on patient selection and based on who is considered resectable as this decision is somewhat subjective.
The largest retrospective review of 1104 unresectable patients who were given 5-FU/LV combined with oxaliplatin (70%), irinotecan (7%) or both (4%) revealed that 12.5% of patients, who were considered ‘good responders’ (not further defined in the paper), underwent hepatic resection after an average of 10 courses of chemotherapy but 80% relapsed during the mean follow-up period of 48.7 months [Adam et al. 2004a].
FOLFOXIRI has been explored in two phase III trials in unselected patients and in one phase II trial in selected patients with isolated CLM, and has some of the highest response rates seen with any chemotherapy regimen. In the HORG trial, 283 patients with unresectable disease not confined to the liver received FOLFOXIRI versus FOLFIRI in the first-line setting with no difference in PFS and OS, and no significant change in the rate of surgical resection. Ten per cent of the patients treated with FOLFOXIRI and 4% of the patients treated with FOLFIRI (p = 0.08) underwent resection, with 64% and 33% having R0 resections, respectively. There was a significant increase in toxicities in the FOLFOXIRI arm, mainly in alopecia, diarrhea and neuropathy [Souglakos et al. 2006]. In the GONO trial, 244 patients with untreated initially unresectable disease were randomized to FOLFOXIRI versus FOLFIRI (Douillard regimen). Response rates and R0 resection rates were higher in the FOLFOXIRI arm compared to FOLFIRI (RR 60% versus 34%, p < 0.0001; R0 rates 15% versus 6%, p = 0.033) in patients with isolated CLM. Results showed improvement in PFS (9.8 months versus 6.9 months, p = 0.0006) and a median OS (23 months versus 17 months, p = 0.032) with increased, but not prohibitive, toxicities for the 4 drug regimen [Falcone et al. 2007]. Of note, the FOLFOXIRI arm on the GONO trial received 5-FU 3200 mg/m2 as a continuous infusion over 48 hours while the FOLFOXIRI arm on the HORG trial and the FOLFIRI arms on both the trials received the less dose intense 5-FU 400 mg/m2 bolus followed by 600 mg/m2 given over 22 hours on days 1 and 2 (known as the Douillard regimen), possibly explaining the better response rates with FOLFOXIRI in the GONO trial. In the single-arm phase II trial by Ychou and colleagues, 34 patients with isolated unresectable CLM were enrolled and had a response rate of 71%. This trial used an infusion of 5-FU at 2400 mg/m2 over 46 hours rather than the Douillard regimen. A very high number of patients or 82% were converted with this regimen, likely due to careful selection of patients [Ychou et al. 2008]. It is unclear if targeted therapies added to this three-agent regimen would be tolerated but such trials are currently ongoing (CHARTA, PERIMAX) [Stein et al. 2012].
The effect of adding targeted therapies to preoperative conversion chemotherapy is not well established (see Table 2). Bevacizumab addedto oxaliplatin- or irinotecan-based first-line chemotherapy regimens has been shown to increase response rates by ~0–10% and median OS anywhere from 2–6 months in all patients with metastatic disease [Giantonio et al. 2007; Hurwitz, 2004; Kozloff et al. 2009]. Similarly, adding EGFR inhibitors (cetuximab or panitumumab) to first-line chemotherapy in unselected patients with metastatic disease has been shown to increase response rates by 10–20% and improve OS by 2–3 months [Bokemeyer et al. 2009; Douillard et al. 2010; Maughan et al. 2011; Van Cutsem et al. 2011]. Of note, cetuximab has not been shown to improve OS when given with oxaliplatin-based regimens [Maughan et al. 2011; Tveit et al. 2012] and this combination has therefore been removed from the NCCN guidelines [NCCN, 2013] and should not be routinely considered as conversion chemotherapy.
Conversion chemotherapy trials with targeted agents for initially unresectable CLM.

In patients who underwent resection; **arm C with intermittent FLOX+Cmab is not presented here; ***all patients presented were KRAS wildtype only but it is not clear from the study whether the resected patients were KRAS wildtype or mutated.
bev, bevacizumab; CAPEOX, capecitabine/oxaliplatin; CLM, colorectal liver metastasis; Cmab, cetuximab; EGFR, epidermal growth factor receptor; FLOX, bolus 5-FU 500 mg/m2 and folinic acid 60 mg/m2 on days 1-2, oxaliplatin 85 mg/m2; FOLFIRI, 5-FU/irinotecan; FOLFIRINOX/FOLFOXIRI, 5-FU/irinotecan/oxaliplatin; FOLFOX4, (5-FU bolus 400 mg/m2 and leucovorin 200 mg/m2 followed by infusional 5-FU 600 mg/m2 over 22 h on days 1-2, oxaliplatin 85 mg/m2); FOLFOX6, (5-FU bolus 400 mg/m2, infusional 5-FU 2400 mg/m2 over 46 h, leucovorin 400 mg/m2, oxaliplatin 100 mg/m2); FOLFOX7 (infusional 5-FU 2400 mg/m2 over 46 h, leucovorin 400 mg/m2, oxaliplatin 130 mg/m2); IFL, irinotecan/bolus 5-FU; IROX, irinotecan/oxaliplatin; mo, months; mFOLFOX6, modified FOLFOX6 (5-FU bolus 400 mg/m2, infusional 5-FU 2400 mg/m2 over 46 h, leucovorin 400 mg/m2, oxaliplatin 85 mg/m2); NR, not reported; Pmab, panitumumab; VEGF, vascular endothelial growth factor; wt, wildtype.
Randomized trials comparing FOLFOX with and without bevacizumab in isolated CLM have not been reported. Bevacizumab only moderately improved resectability rates when given with FOLFOX/CAPEOX in the NO16966 trial (6.1% with chemotherapy alone versus 8.4% in the combination arm). Furthermore, only 47% patients in the chemotherapy arm and 29% patients in the chemotherapy and bevacizumab arm were treated until progression of disease and the addition of bevacizumab did not improve response rates [Saltz et al. 2008]. Bevacizumab was assessed in combination with the 3 drug regimen, FOLFOXIRI, in 57 patients with unresectable disease whereof 30 patients had isolated CLM. Response rates were dramatic or 80% in the CLM-only group with 40% undergoing surgery and a median OS of 30.9 months in all patients irrespective of resection. Neutropenia was the most commonly reported grade 3/4 adverse event, seen in 25% of patients [Masi et al. 2010]. A single-arm study with 43 patients treated with FOLFIRI and bevacizumab revealed a response rate of 65% with 9% of patients subsequently undergoing liver resections [Kopetz et al. 2010]. A retrospective study showed the addition of bevacizumab to FOLFOX to cause a reduced degree of tumor viability but did not affect the number of complete pathologic response (11.3% versus 11.6%). Interestingly, patients who received bevacizumab had a decreased incidence and severity of sinusoidal dilatation [Ribero et al. 2007]. Another study found bevacizumab to increase the degree of necrosis in the resected tumor (55% versus 32% in patients without bevacizumab, p = 0.001) but not complete pathologic response rates (3% versus 8%, p =0 .307) [Wicherts et al. 2011]. Bevacizumab has been known to cause problems with wound healing [Kozloff et al. 2009], and as it has a half-life of 20 days, it is commonly recommended to have 6–8 weeks elapse between last dose of bevacizumab and time of surgery.
The phase II CELIM trial investigated cetuximab in combination with either an oxaliplatin- or irinotecan-based regimen in initially unresectable patients with isolated CLM (defined as ≥5 tumors, technically unresectable on the basis of inadequate FLR, infiltration of both hepatic arteries/portal vein branches or infiltration of all hepatic veins). Objective responses were seen in 68% versus 57% of patients on oxaliplatin versus irinotecan-based regimens with cetuximab. R0 resection rates were high or 38% and 30% in the two groups, but as no comparison was made to a group without cetuximab, the benefit of adding it is not clear [Folprecht et al. 2010]. A total of 70% of KRAS wild-type tumors had a response while only 41% of KRAS mutated tumors had a response. Similarly the CRYSTAL trial showed a modest increase in rate of surgery and R0 resection in KRAS wild-type patients who received FOLFIRI with cetuximab versus FOLFIRI alone (surgery rate 7.9% versus 4.6% p = 0.0633; R0 resections 5.1% versus 2.0%, p = 0.0265), respectively [Van Cutsem et al. 2011]. A phase II trial reported at the annual European Society of Medical Oncology (ESMO) meeting in 2012 randomized 116 patients with KRAS wild-type tumors to mFOLFOX6 or FOLFIRI with or without cetuximab. Response rates were 66% versus 33% in the 2 arms with improved R0 resection rates (31% versus 9%) and a median OS of 46.6 months in the resected cetuximab arm [Xu et al. 2012]. Assenat and colleagues explored adding cetuximab to the 3-drug regimen, FOLFOXIRI, in a phase II single-arm trial with 42 patients (57% were KRAS wildtype) where 81% had a response to therapy but resection rates were not reported. Grade 3/4 adverse events included diarrhea (52%), neutropenia (38%) and asthenia (32%) [Assenat et al. 2011]. Other randomized clinical trials with EGFR inhibitors, not only including CLM patients, are reported in Table 2 and have shown minimal benefit of adding an EGFR inhibitor [Bokemeyer et al. 2011; Douillard et al. 2010; Tveit et al. 2012]. The only randomized study to report resectability rates with panitumumab did not show an increase in resectability rates [Douillard et al. 2010], but a study reported at ESMO 2012 in selected unresectable CLM patients receiving CAPEOX with panitumumab revealed response rates of 54% in KRAS wild-type patients with conversion rates of 31% [Leone et al. 2012].
When choosing an appropriate targeted agent with cytotoxic chemotherapy, it is not clear at this point which is most efficacious. Bevacizumab has been shown to both increase the degree of necrosis in the tumors and to reduce the toxicity of oxaliplatin, while there are currently no studies reporting the pathologic effects of adding an EGFR inhibitor. We would therefore commonly choose bevacizumab as the biological agent in addition to cytotoxic chemotherapy for conversion but further trials are needed. If patients are able to tolerate triplet chemotherapy regimens, this may also be a good choice as they have greater response rates, although there are increased toxicities and it is unclear if a targeted therapy should be given concomitantly.
Conclusion
Identifying patients who can be resected either upfront or potentially after downsizing of their tumor with conversion chemotherapy is important as resection of isolated CLM can significantly impact survival. Response rates correlate with both resectability rates and OS, and therefore chemotherapy regimens with the highest response rates should be chosen. Three-drug regimens (FOLFOXIRI) may be appropriate for patients with excellent performance status. Alternatively, targeted therapies (bevacizumab) have been shown to cause morphological changes in the tumors that can correlate with survival and may therefore be a good choice with cytotoxic chemotherapy while the efficacy of EGFR inhibitors is less lucid at this point. The only selected patient trials using EGFR inhibitors with cytotoxic therapy had high response and resectability rates and could therefore be considered in patients with KRAS wild-type tumors. Patients who are resectable upfront should not receive neoadjuvant chemotherapy, especially if they have few metastases confined to one lobe of the liver. It is a little less clear what to do for patients with more than four liver metastases but who seem to be resectable upfront as these patients were not included in the only randomized trial for resectable patients (EORTC 40983) and have worse prognosis than patients with less tumor burden. The management of patients with isolated CLM requires a multimodality approach with the cooperation of medical oncologists, surgical oncologists and interventional radiologists to achieve the best outcomes and further studies are needed to determine optimal therapies.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflict of interest in preparing this article.