
Abstract
Breast cancer is the most frequent malignant tumor in women worldwide and as breast cancer incidence increases with increasing age, over 40% of new cases are diagnosed in women older than 65 years of age. However, older patients are not treated to the same extent as younger patients and increasing age at diagnosis predicts deviation from guidelines for all treatment modalities. Evidence-based medicine in older patients is lacking as they are usually excluded from clinical trials often because of existing comorbidities and limited life expectancy. Accordingly, there is a higher competing risk of death from other causes than breast cancer compared with younger patients and this may have led to the false interpretation that prognosis of breast cancer in older patients is relatively good. However, every treatment modality should be evaluated during treatment decision making. Multimodal therapy should not be routinely withheld as data show that disease-specific mortality increases with age, probably due to undertreatment. Prognostic markers, fitness and comorbidities rather than chronological age should determine optimal, individualized therapy. It is recommended that treatment decisions should be discussed in a multidisciplinary setting, ideally in combination with any form of geriatric assessment, to improve breast cancer outcome in the older population.
Evidence-based medicine
Breast cancer is the most frequent malignant tumor in women worldwide, with almost 1,400,000 new cases in 2008 [Jemal et al. 2011]. In the USA, 41% of these women were 65 years or older at diagnosis [data.gov, Surveillance Epidemiology and End Results, 2011]. As breast cancer incidence increases with age, worldwide changing demographics and increasing life expectancy are expected to further enlarge the absolute number of older women with breast cancer.
Several studies have shown that older patients are not treated to the same extent as younger patients; older patients with breast cancer have lower odds of receiving standard care [Yancik et al. 2001; Allemani et al. 2010]. Studies on adherence to breast cancer guidelines have shown that increasing age at diagnosis predicts deviation from guidelines for surgical therapy [Yancik et al. 2001; Allemani et al. 2010; Giordano et al. 2005; White et al. 2003], adjuvant radiotherapy [Yancik et al. 2001; Allemani et al. 2010; Giordano et al. 2005; White et al. 2003], chemotherapy [Giordano et al. 2005; White et al. 2003], and endocrine therapy [Giordano et al. 2005; White et al. 2003]. However, guideline deviation does not necessarily equal inappropriate treatment. Adherence to guidelines may not improve breast cancer cure and care in older patients as is expected in the young population because evidence-based medicine in older patients is lacking.
Despite comprising a large proportion of patients with breast cancer, older patients are underrepresented in trials [Wildiers et al. 2007]. In the 1990s, the characteristics of over 16,000 patients, who were consecutively enrolled in trials between 1993 and 1996 were compared with the corresponding characteristics in the general population. Only 9% of patients in breast cancer trials were 65 years or older [Hutchins et al. 1999]. A recent literature review showed that of all clinical trials published in 2008 in five major medical journals, 20% excluded patients based on age. In the remaining trials, almost half of the studies excluded patients with age-related diseases [Zulman et al. 2011]. In addition, treating physicians have been shown to be less likely to recruit patients for clinical trials. Older patients, in contrast, do not consider their age as an important reason for not participating in trials [Townsley et al. 2005].
The generalizability of trials may be limited. Next to an underrepresentation of older patients, studies which include older patients are likely to have selection bias; only older patients considered ‘healthy enough’ will enter these studies. Additionally, older patients differ from younger patients in many aspects. The presence of comorbidities and concomitant medications may interact with treatment or survival of breast cancer [Louwman et al. 2005; Bastiaannet et al. 2010; Pallis et al. 2010; Houterman et al. 2004]. Moreover, older patients have a higher competing risk of death and life expectancy is generally limited compared with younger patients. Therefore, relevant study endpoints may vary with age. In conclusion, there seems to be reasonable grounds to doubt external validity of trials including only younger patients.
Prognosis of older patients with breast cancer
Given the lack of evidence-based medicine, is there evidence that we are treating older patients with breast cancer properly? Bastiaannet and colleagues showed that, in contrast to younger patients, survival of older patients with breast cancer has not improved significantly in recent years [Bastiaannet et al. 2011]. A retrospective analysis of 9766 postmenopausal women with hormone-receptor- positive breast cancer included in the TEAM (Tamoxifen Exemestane Adjuvant Multinational) trial revealed that breast cancer mortality increases with age, regardless of a higher risk of other-cause mortality and independent of tumor and treatment characteristics [van de Water et al. 2012b]. It is tempting to speculate on the underlying mechanisms which could explain these results. The most plausible explanation is that older patients included in this trial may have experienced undertreatment. All patients received surgery and endocrine therapy, while radiotherapy after a wide local excision was administered less frequently with increasing age. Moreover, while 48% of patients aged 75 years or older had nodal involvement, only 5.2% received adjuvant chemotherapy.
The design of the study renders the findings hypothesis generating. Until studies specifically address efficacy of treatment in older patients with breast cancer, it is challenging to point out appropriate treatment. Recently it was shown that the effect of comorbidities on overall survival was quantitatively similar to that of breast cancer stage [Patnaik et al. 2011]. Effective management of comorbidities, next to breast cancer management, may therefore result in longer overall survival for older patients with breast cancer.
Treatment of older patients with breast cancer
Locoregional therapy
Breast surgery remains the standard primary therapy of early breast cancer in older patients. The majority of older patients tolerate surgery and anesthesia with very low morbidity and almost nonexistent mortality [Wyld and Reed, 2007]. Older patients do not appear to be at increased risk of complications following axillary surgery, and quality of life after both sentinel node biopsy and axillary clearance was shown to be higher in older women than in younger women [Fleissig et al. 2006].
According to an overview of the Early Breast Cancer Trialists’ Collaborators Group, age did not affect the proportional reduction in local recurrence for irradiation after breast-conserving surgery. However, the absolute benefit of treatment was lower in older patients as absolute recurrence risk was lower [Clarke et al. 2005]. Administration of radiotherapy requires frequent hospital visits, which may be impeded by decreased mobility in old age. Hypofractionated radiotherapy showing good local control, comparable to historical results of conventional whole-breast fractionation, could be a valuable alternative as it permits a briefer period of treatment and fewer hospital visits [FAST Trialists Group, 2011; Rizzo and Wood, 2011; Freedman et al. 2012].
Breast brachytherapy could be another option for older women with breast cancer. However, caution has been raised recently by a large retrospective study showing more complications and more subsequent mastectomies than with postoperative whole-breast radiation [Smith et al. 2012], though there was no difference in survival.
Lately, several studies have addressed the question of whether radiotherapy after breast-conserving surgery could be safely omitted in selected populations [Hughes et al. 2004; Tinterri et al. 2009]. Recent data demonstrate that in women aged at least 70 years with clinical stage I, estrogen-receptor-positive breast cancer who have had lumpectomy and are receiving tamoxifen, the addition of radiotherapy results in an absolute reduction of 6% in ipsilateral breast tumor recurrence but has no impact on survival, distant disease-free survival or breast-cancer-specific survival [Hughes et al. 2010]. Given the low rate of breast cancer deaths in this age group, radiotherapy might be safely omitted in older patients with small tumors who are node negative and have hormone-receptor-positive disease. However, evidence from prospective trials is limited.
Endocrine therapy
Primary endocrine therapy should only be offered to women with hormone-receptor-positive tumors who are unfit for or refuse surgery [Hind et al. 2007; Chakrabarti et al. 2011]. Adjuvant endocrine therapy for older patients with hormone-receptor-positive tumors remains a standard treatment option in reducing breast cancer recurrence risk. Treatment choice should be based on individual patient characteristics, such as risk of recurrence and known side effects in relation to existing comorbidities including arthritis or a history of thrombosis. One should be aware of the age-associated nonpersistence rate. Studies have shown that older patients are more likely to discontinue tamoxifen before completion of 5 years of therapy [Barron et al. 2007; Partridge et al. 2003; van de Water et al. 2012a]. Recently we showed that in postmenopausal women with hormone-receptor-positive breast cancer, nonpersistence of adjuvant endocrine therapy within 1 year of follow up was associated with disease-specific survival and overall survival in patients younger than 65 years, but not in patients aged 65–74 years or in patients aged 75 years or older [van de Water et al. 2012a]. Although the study design was unfit to report on the efficacy of adjuvant endocrine therapy in older patients with breast cancer, the findings urge further age-specific studies.
Chemotherapy
The added value of adjuvant chemotherapy in older patients with breast cancer is currently being discussed. Recently the Early Breast Cancer Trialists’ Collaborators Group compared different polychemotherapy regimens. Although few older patients were included in the analyses, age did not significantly affect proportional risk reductions with taxane- or anthracycline-based chemotherapy. However, the absolute risk reduction would be greater in younger than in older patients as more years are lost by death at a younger age [Peto et al. 2012].
Recently the Adjuvant ChemoTherapy In Older womeN (ACTION) trial was initiated, in which older patients were randomized to four cycles of anthracycline chemotherapy or observation [Leonard et al. 2011]. Despite widespread support, the trial was closed early because of a lack of recruitment. The majority of patients who were eligible and were approached declined trial entry. In most cases this was due to the patient not wishing to undergo chemotherapy, although a smaller proportion made an active choice for chemotherapy. Next, inclusion was restricted to high-risk patients, which may have limited the number of eligible patients. Similarly the Chemotherapy Adjuvant Studies for women at advanced Age (CASA) trial closed early due to poor recruitment [Ring et al. 2011]. However, Muss and colleagues demonstrated that it is possible to recruit older patients with breast cancer for a chemotherapy trial [Muss et al. 2009]. Overall, 633 patients were included, of which 411 (65%) were aged 70 years or older. The trial was designed to test noninferiority of oral capecitabine compared with standard chemotherapy. Standard chemotherapy showed a superior relapse-free survival. As suggested in the TEAM trial, relatively fit older patients may benefit from adjuvant chemotherapy treatment [van de Water et al. 2012b]. However, older patients may have an increased toxicity risk when treated with chemotherapy [Pallis et al. 2010], which may impede quality of life. In the abovementioned trial by Muss and colleagues, quality of life after 1-year follow up was similar for both treatments [Kornblith et al. 2011]. A predictive score for chemotherapy toxicity may help to assess the individual risk of severe toxicity from chemotherapy [Extermann et al. 2011].
Decision making
Treatment bias and undertreatment
Undertreatment is a well documented phenomenon in older patients with breast cancer, having an impact on patient outcome as it leads to unnecessary disease-specific deaths [Bouchardy et al 2007; Schonberg et al 2011; van de Water et al 2012b]. There is strong evidence from multiple studies that older patients with breast cancer have lower odds of receiving standard care and increased age at diagnosis is a risk factor for deviation from international breast cancer treatment guidelines [Yancik et al. 2001; Allemani et al. 2010]. Older women are less likely to have surgery for operable breast cancer than younger women [Lavelle et al 2007] and radiotherapy is administered less frequently, even following breast-conserving surgery [van de Water et al. 2012b]. Compared with younger women with breast cancer of the same stage, older patients receive adjuvant chemotherapy to a significantly lower extent or with lowered doses [Bouchardy et al. 2007; Giordano et al. 2005; van de Water et al. 2012b]. The main reasons for this practice are limited life expectancy of older women, often existing comorbidities and increased frequency of treatment adverse events. Given the fact that several studies have shown that breast cancer mortality as a proportion of all-cause mortality decreases with age [Bastiaannet et al. 2010; van de Water et al. 2012b] there is a general belief among physicians that older women present with less aggressive breast cancer with relatively good prognosis, leading to undertreatment of these women [Markopoulos et al. 2011].
Risks and benefits of multimodal treatment
There is evidence that outcome is compromised in older patients with breast cancer in whom less than complete combined modality treatment is undertaken and multimodal therapy should not be routinely withheld [van Leeuwen et al. 2011]. However, the large heterogeneity in this population presenting with a high incidence of comorbidities and other age-related problems does not allow uniform treatment recommendations to be made. Prognostic markers, fitness and comorbidities rather than chronological age should determine therapy. Every treatment modality should be evaluated in terms of its efficacy to decrease disease-specific mortality, safety for not adding morbidity or impeding quality of life, and necessity in relation to remaining life expectancy. Evaluation of certain elements of a comprehensive geriatric assessment (Table 1) could help in treatment decision making during the multidisciplinary team meeting (Figure 1). Final treatment choice should respect the patient’s personal preference.
Basic elements of comprehensive geriatric assessment.
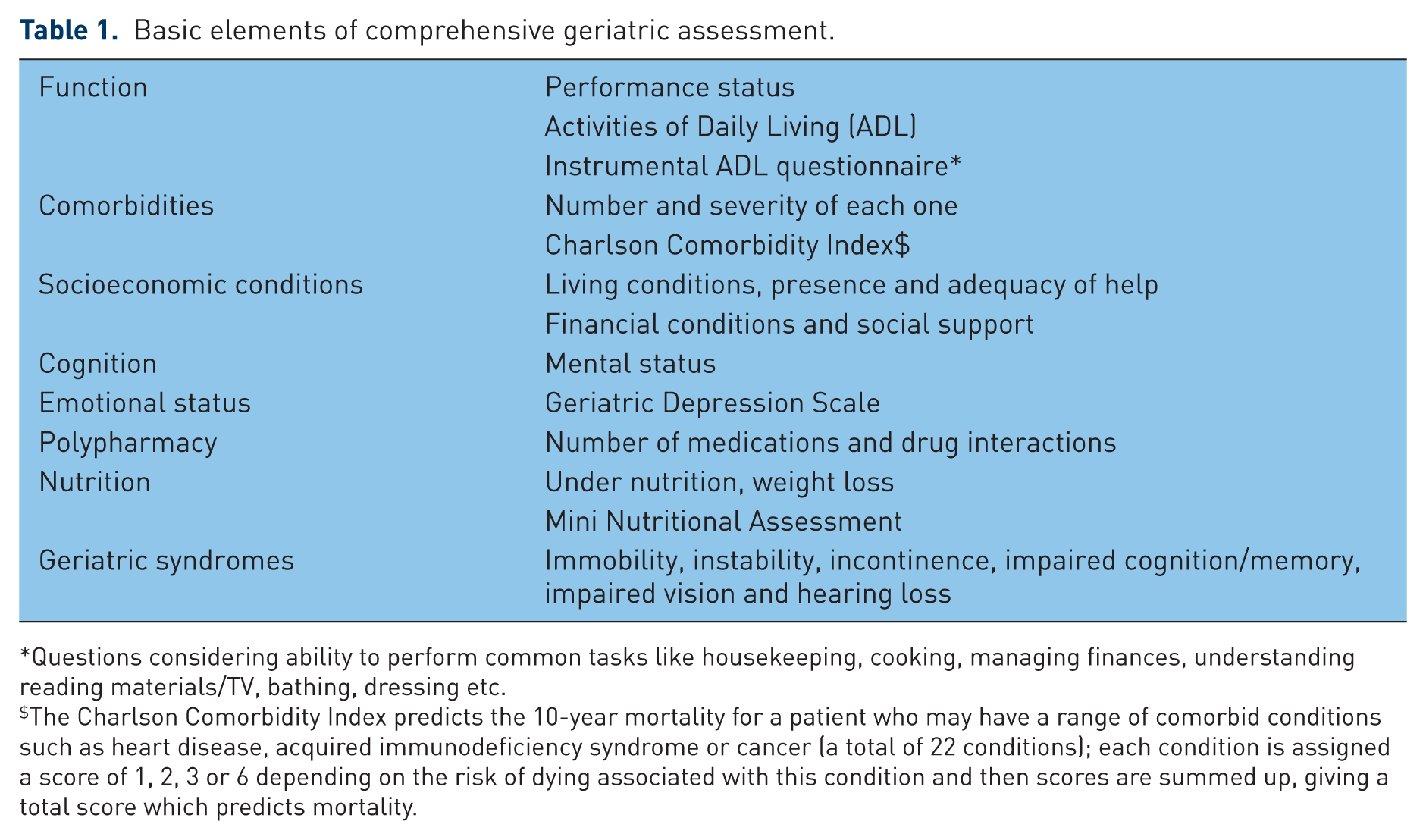
Questions considering ability to perform common tasks like housekeeping, cooking, managing finances, understanding reading materials/TV, bathing, dressing etc.
The Charlson Comorbidity Index predicts the 10-year mortality for a patient who may have a range of comorbid conditions such as heart disease, acquired immunodeficiency syndrome or cancer (a total of 22 conditions); each condition is assigned a score of 1, 2, 3 or 6 depending on the risk of dying associated with this condition and then scores are summed up, giving a total score which predicts mortality.

Treatment decision algorithm in older patients with early breast cancer.
Future perspectives
Patient characteristics, such as comorbidities and remaining life expectancy, and tumor characteristics both affect treatment recommendations. To improve breast cancer outcome in patients of all ages, age-specific breast cancer studies have to provide definite answers to the question, what is appropriate treatment for older patients with breast cancer? There are several possibilities to fill the ‘evidence gap’. In addition to large clinical trials with only minor exclusion criteria, which enable older patients to be included, alternative study designs may be helpful. Restriction in research topics, design and analysis may give observational research the chance to be as credible as randomized evidence [Vandenbroucke, 2004]. Large, quality-assured prospective cohort studies generate a large amount of reliable data. Moreover, these data are a representative selection of the general population, including the substantial heterogeneity within older patients.
Conclusion
Three things are important in improving breast cancer outcome in the large population of older patients with breast cancer. First, the decreased proportion of all-cause mortality attributed to breast cancer may have led to the conclusion that disease-specific mortality decreases with increasing age. The medical society should be aware of the lack of survival gain in older patients in recent years [Bastiaannet et al. 2011], and the impaired breast cancer survival in relatively fit older patients [van de Water et al. 2012b]. Second, wherever possible, older patients and treating physicians should be encouraged to take part in clinical trials. Third, alternative study designs should be explored in these patients or topics in which a clinical trial is not feasible. Our joint efforts will hopefully result in evidence-based medicine for older patients with breast cancer.
Footnotes
Funding
No specific grant from any funding agency in the public, commercial, or not-for-profit sectors was received for this article.
Conflict of interest statement
Christos Markopoulos received educational grants and lecture honoraria from AstraZeneca, Novartis (Basel, Switzerland), and Pfizer Inc. (New York, NY, USA). Willemien van de Water has no conflict of interest to report. No writing assistance was utilized in the production of this manuscript.