
Abstract
Background
Management of complex lateral end clavicle fractures with coraco-clavicular ligament disruption can be challenging.
Methods
We prospectively analysed 19 (17 M:2F) patients from January 2014 to June 2016. Six patients had intra-articular fractures (Edinburgh-3B2) and the remaining were extra-articular (3B1). All patients had open reduction internal fixation with lateral end locking plate augmented with a coracoid anchor. All patients were evaluated at the final follow-up by American Shoulder and Elbow Surgeon score (ASES), Disabilities of the Arm, Shoulder and Hand (DASH), Oxford Shoulder Score (OSS), return to work, sports and radiographs.
Results
At a mean follow-up of 54 months (range 37–64), 19 patients were available for analysis. Mean age of patients was 34 years (range 24–65). At final follow-up DASH score was 1.66 (range 0–5); ASES score was 98.14 (93.3–100) and OSS was 46.6 (42–48). There was no difference in the functional outcome between 3B1 and 3B2 fractures (DASH – p(0.51); ASES – p(0.44); OSS – p(0.69)). All patients returned to preinjury level of function, sports and work. Five patients needed implant removal and three developed capsulitis that resolved with conservative treatment.
Conclusion
Locking plate fixation, augmented with coracoid anchor is an effective option in the management of these complex injuries. The need for implant removal is reduced (26%) and there is no difference in the functional outcome between 3B1 and 3B2 fractures.
Keywords
Introduction
Clavicle fractures account for approximately 4% of all fractures and 10% of shoulder injuries. 1 Lateral end clavicle fractures comprise 15% of all clavicle fractures and are associated with increased risks of non-union and poor functional outcome.1–5 The two major factors that predispose these fractures to non-union are displacement and coraco-clavicular ligament disruption.1–9 Various surgical methods have been described in the literature to manage lateral end clavicle fractures associated with coracoclavicular ligament disruption.6–11
A commonly used technique in these injuries is hook plate fixation; however, this is associated with a complication rate of upto 40% and a need for secondary surgery to remove the plate.6,11,12 Locking plate fixation in unstable Edinburgh 3B1 and 3B2 fractures is challenging and if not augmented with coraco-clavicular fixation, could lead to failure of the fixation.12,13 The aim of this study was to evaluate the radiological and functional outcome in unstable lateral end clavicle fractures (Edinburgh 3B or Neer type V) 3 with no attachment of coracoclavicular ligament to both medial and lateral end clavicle fracture fragments, treated with locking plate and coracoid anchor augmentation.
Patients and methods
From January 2014 to June 2016, the medical records, outcome score database and radiographs of patients with unstable lateral end clavicle fractures, who presented to our hospital were retrospectively reviewed. Nineteen consecutive patients with Edinburgh Type 3B displaced unstable lateral end clavicle fractures were included in the study. Patients with non-union, children, open fractures, associated shoulder girdle injuries, pre-existing shoulder conditions and those living out of catchment area were excluded from the study. Twelve patients had extra-articular (Edinburgh 3B1) and six patients had intra-articular fractures (Edinburgh 3B2). Using Neer’s classification, 1 all were type V fractures. In all patients, the coraco-clavicular ligament was injured, and the fracture was unstable in both antero-posterior and superior-inferior planes. Mean age at presentation is 34 years (range 24–65) and there were 17 males and 2 females. Of the 19 patients, 3 had road traffic accidents, 6 sports related, 7 due to fall from bike and 3 due to a simple fall. One patient had small subdural haematoma and two had rib fractures and small pneumothorax.
Patients’ notes were accessed through the local Caldicott Guardian and Musculoskeletal Audit department. Formal ethical approval was not required.
Surgical technique
The procedure was performed under general anaesthesia with patient in a beach chair position. The fracture was exposed through a bra strap incision, and through the fracture site where the deltoid was torn, the coracoid was identified. An anchor (Acusinch) with size 5 non-absorbable ultra-high molecular weight polyethylene suture was inserted near the base of the coracoid. The fracture ends were then reduced in both axial and coronal planes and temporarily fixed with a K-wire. The fracture was then fixed with a superior distal clavicle plate (Acumed clavicle fixation system, Hillsboro, Oregon) under fluoroscopic guidance. The sutures from the anchor were retrieved through an eyelet that sits in the plate hole and tensioned (Figure 1) to restore the support provided by the coracoclavicular ligament. If there were remnants of coracoclavicular ligament attached to bone, they were sutured to the clavicle using size-1 vicryl (Figure 2(d)). Then the delto-trapezial fascia was closed over the implant and wound closed in layers and the repair was protected by immobilising the shoulder in a with sling for six weeks. Patients were referred to physiotherapy and pendulum exercises and rotational movements were allowed as tolerated immediately after surgery. From two to six weeks they were allowed to do active assisted forward flexion and abduction to 90°. Patients were allowed full range of movements after six weeks and return to sports around 10--12 weeks.
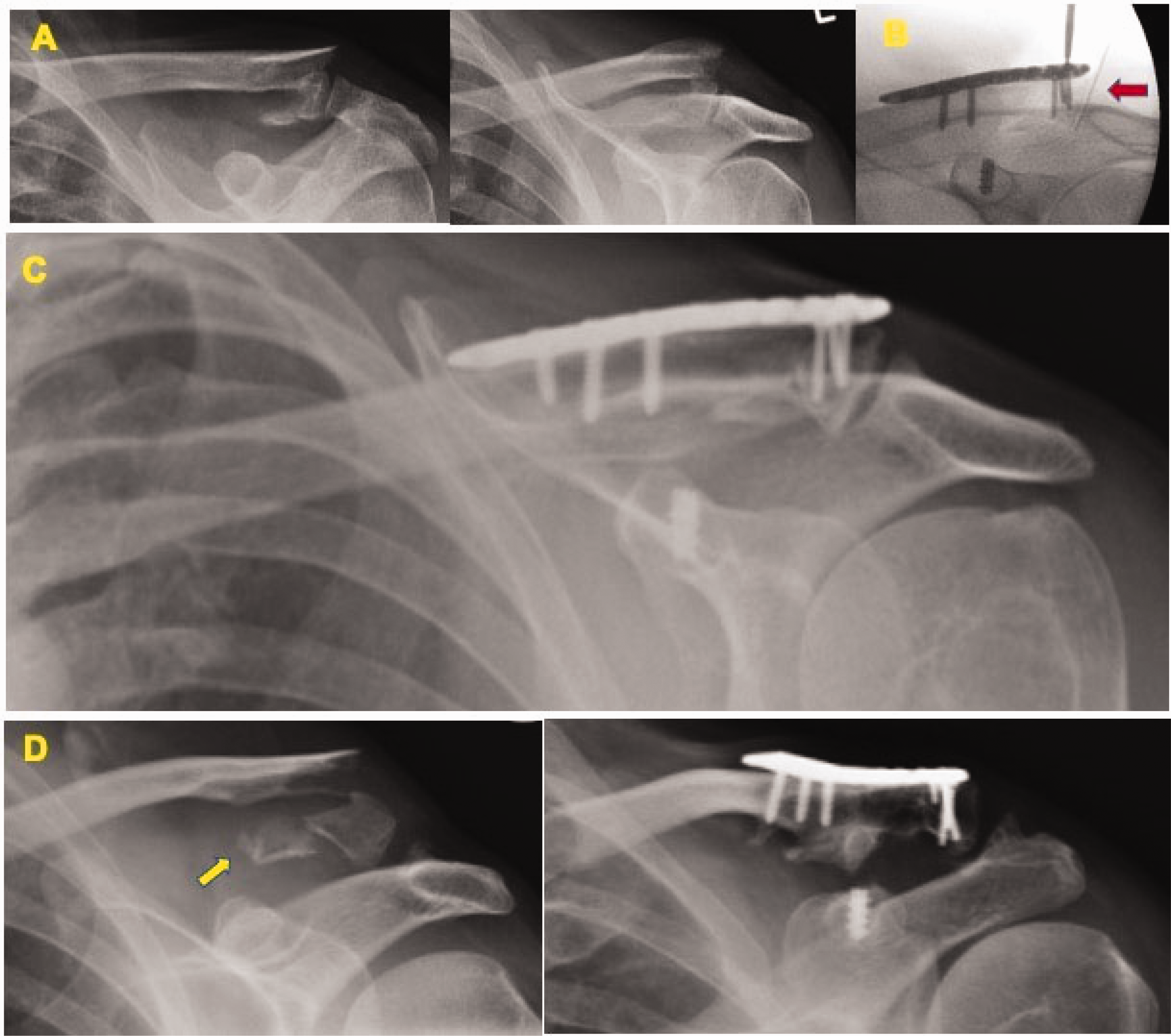
Intra-operative picture after fixation of the fracture showing the coracoid with anchor (yellow arrow) and the eyelet (star). In the later part of the study the knots were tied between the clavicle and coracoid to reduce soft tissue irritation and hence reduce the need for implant removal. (a) Fifty-three-year-old male with fell off from a bicycle and sustained type Edinburgh 3B1 fracture; (b) intra-operatively the ACJ was identified with a needle (red arrow) and lateral row screws were avoided to prevent joint penetration; (c) post-op radiograph at six months and patient returned to preinjury level of activities; (d) 65-year-old male had a skiing injury and sustained Edinburgh 3B1 fracture, fracture fragment with CC ligament attached (yellow arrow) tied with a size 1 Vicryl to the clavicle during surgery; the image on the right is the radiograph at one year.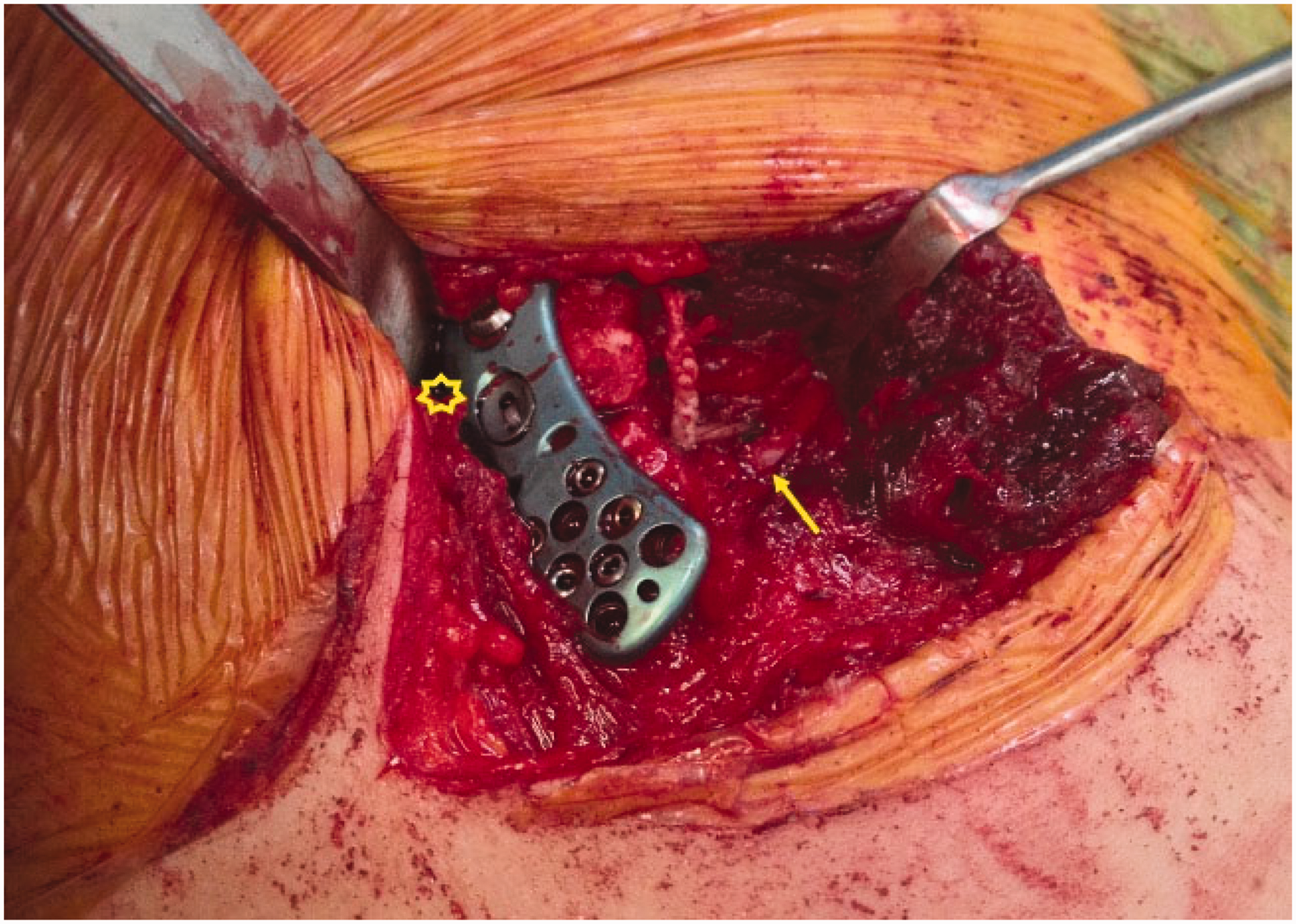
Outcome assessment
Patients were evaluated using Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire, 14 Oxford Shoulder Score (OSS), 15 American Shoulder and Elbow Surgeon score (ASES), 16 radiographs and patient’s return to work and preinjury activities.
Statistics
Statistical analysis was performed using Stata/MP 13.0 for Windows. Data for DASH, OSS and ASES are presented as median with interquartile range. Any difference in these scores by Edinburgh classification was tested using the Kruskal–Wallis rank test. A p value of 0.05 or less was considered significant.
Results
All patients were assessed at a mean follow-up of 54 months (range 37–64). Mean time to surgery was 10 days (range 2–35). All patients achieved radiological healing at a mean of nine weeks (range 6–12; Figures 2 and 3). At the final follow-up, the DASH score was 1.66 (range 0–5); ASES score was 98.14 (93.3–100) and OSS was 46.6 (42–48).
(a) Thirty-four-year-old male had a high energy injury to his dominant shoulder and sustained Edinburgh type 3B2 fracture; (b) radiographs at one year showed that the fracture has healed and the patient returned back to preinjury level of activities.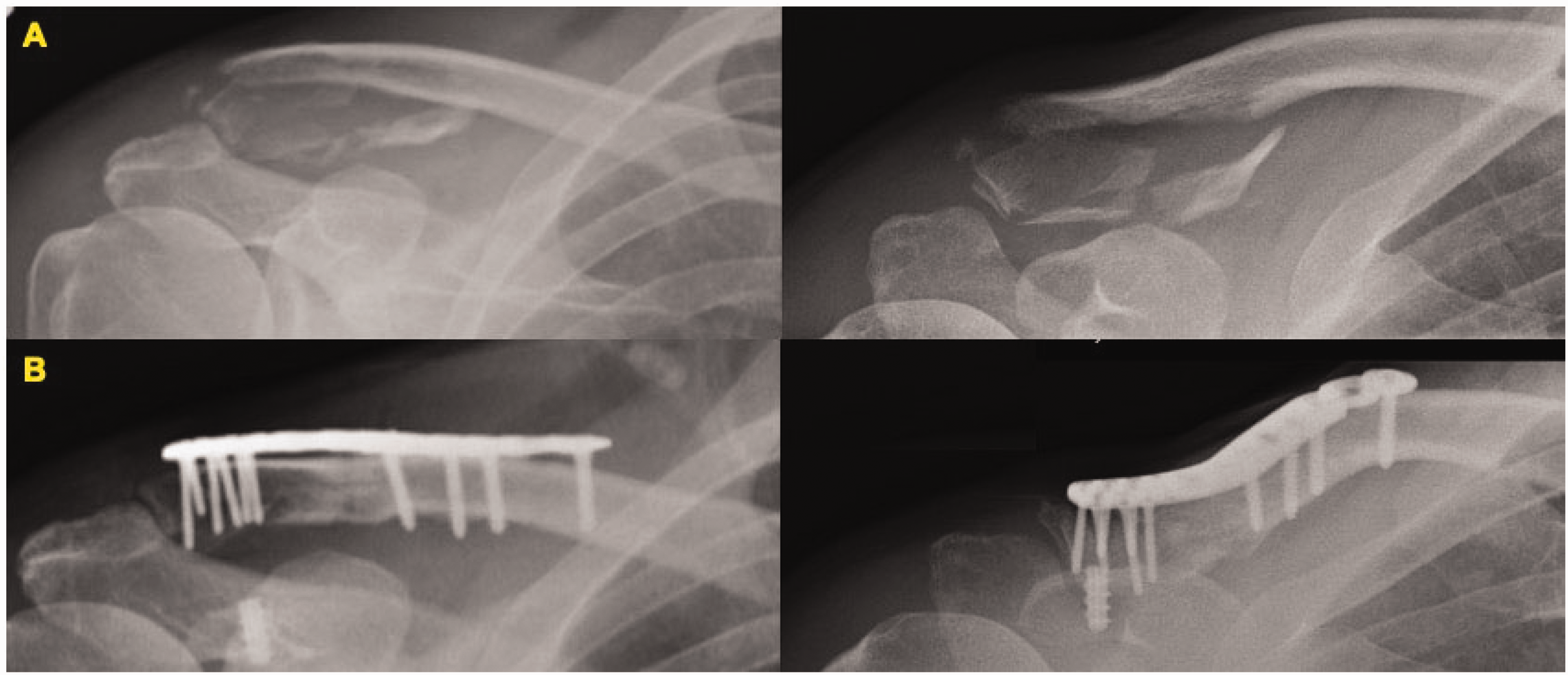
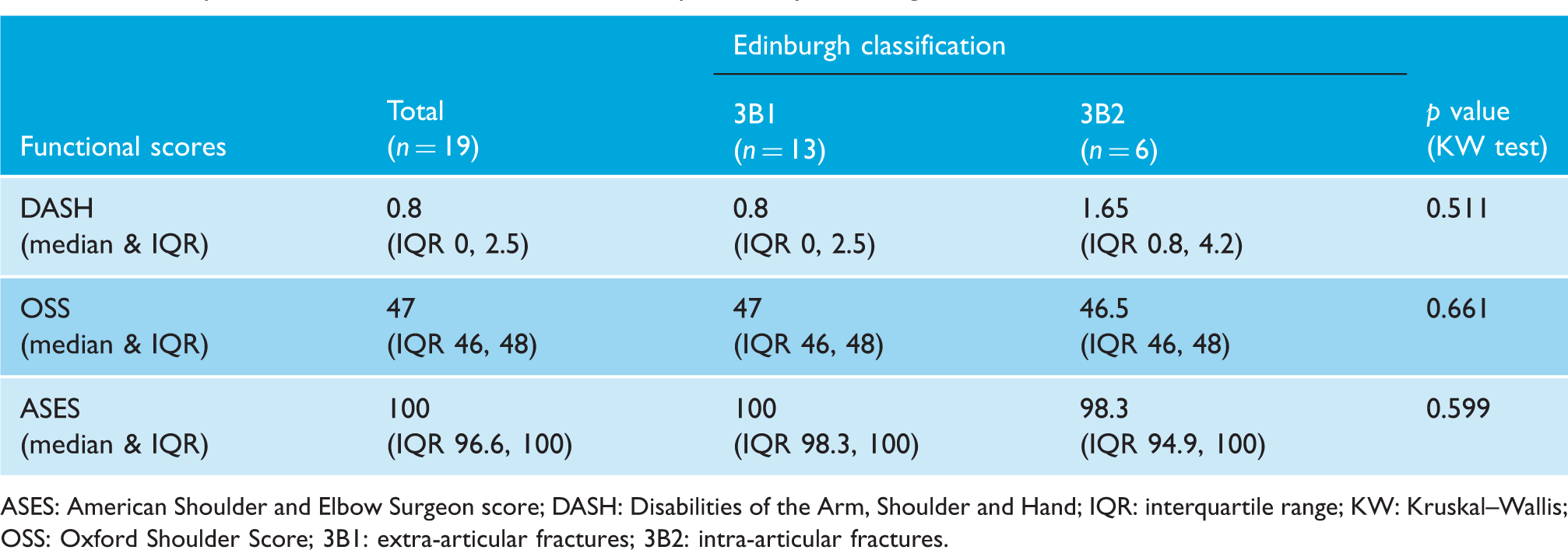
All patients achieved excellent functional outcome at final follow-up and the post-operative median functional scores for patients are depicted in Table 1 and as box plots in Figure 4. The median DASH scores and IQR (interquartile range) for 3B1 and 3B2 groups were 0.8; IQR 0, 2.5 and 1.65; IQR 0.8, 4.2, respectively. However, this difference was found to be statistically non-significant (p = 0.51). The mean Oxford scores for 3B1 and 3B2 class were 46.69 ± 1.75 and 46.33 ± 1.86, respectively. However, this difference in mean Oxford scores was not found to be statistically significant (p = 0.69). The mean ASES scores for 3B1 and 3B2 class were 98.44 ± 2.23 and 97.47 ± 2.96, respectively, and this difference in mean ASES scores was found to be statistically insignificant (p = 0.44). The median DASH, OSS, and ASES scores of extra-articular fractures (3B1) are marginally better than the intra-articular group, however statistically non-significant (p > 0.05).
Box plots depicting post-operative median of functional scores of patients by Edinburgh classification. Post-operative median of functional scores of patients by Edinburgh classification. ASES: American Shoulder and Elbow Surgeon score; DASH: Disabilities of the Arm, Shoulder and Hand; IQR: interquartile range; KW: Kruskal–Wallis; OSS: Oxford Shoulder Score; 3B1: extra-articular fractures; 3B2: intra-articular fractures.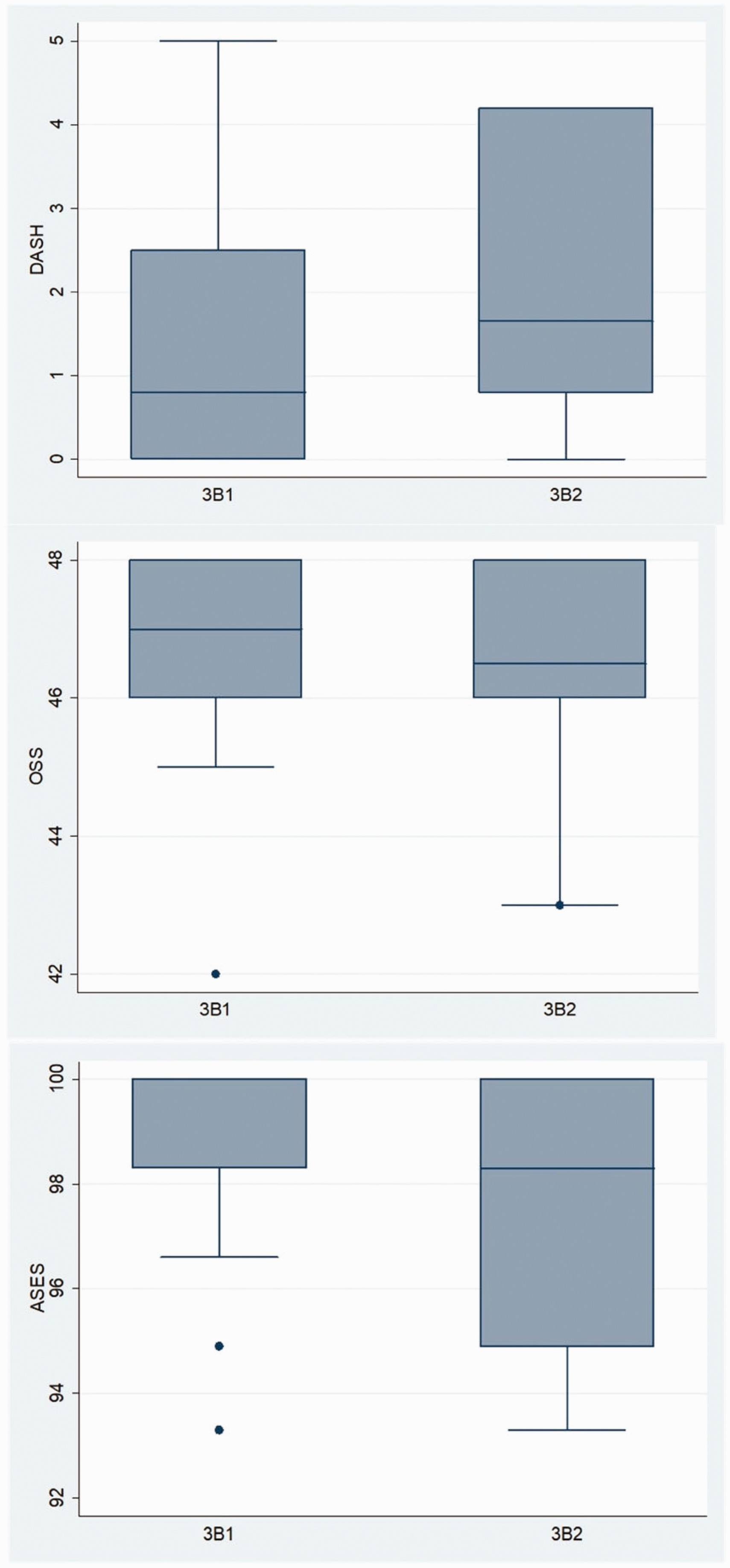
Three patients (15%) developed capsulitis of which two responded well to hydrodistension and steroid injection. One needed implant removal and hydrodistension screw penetration in to the acromioclavicular joint (ACJ; Figure 5). The shape of the ACJ is variable
17
and in very distal lateral end fractures, a needle is inserted into the ACJ to indicate the joint line. The most lateral row of screw holes in the plate may be left empty to avoid joint penetration (Figures 1 and 2(b)). Five patients (26%) needed implant removal, of which three were due to prominent suture knots, one plate irritation and one with screw penetration into the ACJ. In the earlier part of study, knots were tied above the eyelet in the plate. However this was later modified where the knots were tied between the clavicle and coracoid (Figure 1) to avoid skin irritation. Four patients (3B1 – 1; 3B2 – 3) had radiological evidence of ACJ space narrowing, which was clinically asymptomatic. There were no complications related to implant failure, bone healing or osteolysis. Sixteen patients returned to preinjury level of activities and work at a mean of eight months (range 5–13). All the patients returned to preinjury level of function, sports and work at the final follow-up (mean 10.2 months; range 5–26).
(a) Fifty-year-old female had a fall and sustained this injury Edinburgh 3B1 fracture; (b) one screw in the lateral row was prominent and started eroding the acromion (red arrow) and the implant was removed after the fracture healed; (c) 30° cephalic radiograph at one year where the ACJ space is maintained.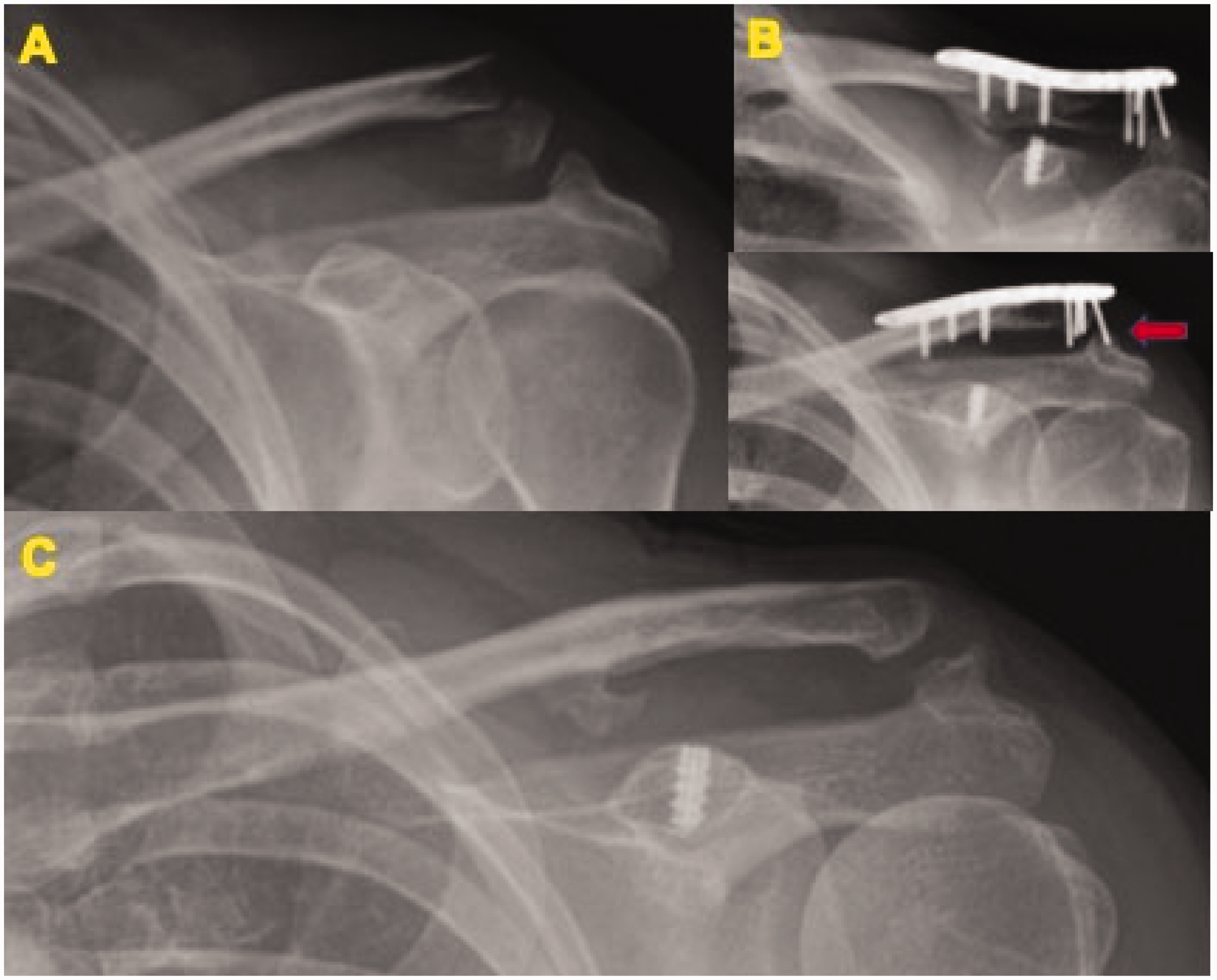
Discussion
Unstable lateral end clavicle fractures form a small percentage of clavicle fractures, but constitute around 50% of clavicular non-union.18,19 The reasons for non-union is multifactorial and are attributable to the opposing forces of muscles attached to the fragments, gravity, detached coracoclavicular ligament and small distal fragment with comminution.1–3,18,19 A number of surgical techniques have been described in the literature and include hook plates, locking plate, coracoclavicular screws, Kirschner wires/tension band wiring, intramedullary fixation and flexible coracoclavicular fixation.6,11 Operative management is preferred for most displaced fractures; however, there is no consensus in the optimum method of fixation.6,11
The Hook plate is the most commonly used implant for treating these injuries, especially those involving coracoclavicular ligament injury and very distal lateral end clavicle fractures (Edinburgh 3B and Neer V).6,11,20–24 One of the major disadvantages of hook plate is that all patients need a second surgery for removal of plate. This causes significant morbidity, delay in recovery of function and is also not cost-effective. In our group, only 26% of our patients needed secondary surgery for implant removal and this was reduced in the later part of our study, after we slightly modified our technique. The reduced need for implant removal in our study is similar to other studies in literature.25,26 The hook plate is associated with a significant number of complications (40.7%) such as dislocation of hook, fracture medial to the plate, non-union, AC joint arthrosis, rotator cuff tear, acromion fracture, acromion osteolysis, etc.6,11,19–26 A study by Klein et al. 7 was one of the earlier articles to highlight the increased complication rate of hook plate (83%) versus locked plate augmented with coracoclavicular fixation (17%). However, the study by Klein et al. has a heterogenous dataset with short-term follow-up. Literature reviews have shown that the hook plate is associated with the highest number of major complications and open reduction internal fixation (ORIF) with coracoclavicular stabilisation has the lowest complication rate.6,11
The other commonly used implant is the locking plate (precontoured or distal radius plate) without coracoclavicular stabilisation.27–31 Locking plates alone could work well in selected Neer Type II extra-articular fractures where there is enough bone stock in the lateral fragment. However, if the lateral fragment is comminuted and/or small, the chances of failure are high. The patients we selected in our study had very distal lateral end fractures (Neer V or Edinburgh 3B) and it is reported in the literature that there is a high failure rate in these patients with isolated locking plate fixation. 13
There are few articles reporting good outcome with isolated coracoclavicular fixation in these fractures.8–10 This type of fixation provides good stability in the superior-inferior direction, however very little in the antero-posterior direction. In ACJ injuries stabilised with a tightrope, Singh et al. noticed joint subluxation and tunnel widening due to ‘windscreen wiper’ micromotion at follow-up. 32 Besides, the dissection needed to achieve reduction could increase the risks of adhesive capsulitis. 12 In suture fixation, complications related to clavicle fracture, corocoid fracture and endobutton migration have also been reported.32–35
Various studies have suggested good results with locking plate fixation supplemented with coracoclavicular ligament stablisation.6,7,11,36,37 Most authors used a loop around the coracoid or endobutton and needed safe soft tissue dissection around coracoid. The coracoid is surrounded by vital structures, especially medially and inferiorly, dissection into this area while applying a loop around coracoid (PDS, tendon) or inserting the endobutton through the inferior cortex of coracoid increases the risk of injury to surrounding vital structures. 38 In our technique, the superior surface of coracoid is exposed and drillhole is made with a 3.5-mm drill (with a unicortical stop at 12 mm) and the anchor inserted. This theoretically reduces the risks of injury to surrounding structures.
Our study has its share of limitations, including the small sample size, which is a reflection of the strict inclusion and exclusion criteria. There was no control group and it is difficult to ascertain the effectiveness of CC fixation, though we have excellent results. A prospective multicentre randomised control trial comparing various techniques is essential to make definitive conclusions.
Conclusion
Our study shows that angular stable locking plate augmented with a coracoid anchor is a safe, effective and reliable option in the management of unstable lateral end clavicle fractures. All the fractures healed and there were no issues with fracture healing and implant failure. Twenty-six per cent of the patients needed implant removal and tying the knot below the clavicle reduced issues with knot irritation. The potential complication of adhesive capsulitis could be minimised with careful soft tissue dissection, screw placement in the lateral fragment under image guidance and early physiotherapy.
Footnotes
Acknowledgements
The authors thank Dr Arvind Kumar Singh for helping with the statistics of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Patients notes were accessed through the local Caldicott Guardian and Musculoskeletal Audit department.
Informed Consent
Informed consent was acquired from the patient for possible publication in journal/presentations.
Guarantor
KK.
Contributorship
KK: data collection, analysis, critical review, writing up of the article; AB: data collection, analysis, writing up of the article; TCS: critical review, writing up of the article; JS: critical review, writing up of the article; RT: critical review, writing up of the article; AT: critical review, writing up of the article.