
Abstract
Purpose:
Fixation of displaced midshaft clavicle is well known to decrease nonunion, malunion and shoulder disability as compared to nonoperative treatment. This study was done to compare the clinical and functional outcome of group 1 clavicle fractures treated with anatomic locking plates (ALP) versus Titanium elastic nail (TEN).
Methods:
We studied patients presenting with displaced midshaft clavicle fractures treated with ALP or TEN. The study period was from Jan 2013 to Dec 2016. Patients were reviewed and at each visit clinical and radiological progress of union was noted, complications if any were noted, functional assessment was done using the quick Dash score and Constant Murley score.
Results:
A total of 116 patients met our inclusion criteria. 62 patients were treated with TEN and 54 with ALP. Bony union was achieved at an average of 11.8 weeks in the TENS group and 12.8 weeks in the ALP group post operatively and this was found to be significant. The mean postoperative Constant Murley score in the ALP and the TEN groups were 92.8 (range 80–97), and 93.7 (82–97) respectively. The mean postoperative quick dash score in the ALP and TEN groups were 2.48(range from 0 to 6.8) and 2.1 (range 0–9.1) respectively.
Conclusion:
Both Anatomical locking plate and TEN are good options for the treatment of non-comminuted mid clavicular fractures as they have a similar functional outcome. TEN nail insertion has the advantage of being minimally invasive, having a faster union time and may be recommended in midshaft clavicle fractures without comminution.
Introduction
Clavicle fractures account for 4% of all bone fractures in adults. 1 Clavicle fractures may result due to an indirect trauma or direct trauma to the bone itself. Most common mechanism of injury is a fall on the outer side of the shoulder and is the cause in 90% of the cases. 2 Allman in 1967 described a classification where Group 1 fractures involve the middle third of clavicle, Group 2 fractures involve the lateral third and Group 3 fractures involve the medial third. 3 Group 1 fractures are the most common as described by Nordqvist and Petersson. 4 There has always been a controversy whether to treat group 1 fractures conservatively or operatively. Previously non operative treatment was considered to be the gold standard for these fractures. 5
The indications for operative treatment of these fractures include open fracture; severe displacement caused by comminution, an imminent lesion of the skin by a sharp edge of the clavicle, and neurovascular injuries. The relative indications for surgery are: multiple trauma, floating shoulder, and symptomatic malunion and nonunion. More recently, other relative indications have been added which include high-energy fractures, clavicle shortening greater than 20 mm, complete displacement, and severe comminution. 6
Recent studies have shown that the rate of nonunion in displaced fractures of the middle third clavicle, treated by a non-surgical treatment is more than 15%, compared to 2.2% in fractures that were surgically treated. 7
The common implants being used currently include, the dynamic compression plate, reconstruction plate, titanium elastic nail (TEN) and the precontoured anatomical locking plates (ALP) specially designed for treating clavicle fractures. 8,9 There are few studies in literature that compare the outcome of ALP versus TEN. We hypothesized that both ALP and TEN used in the treatment of group 1 clavicle fractures will have a similar functional outcome. We did a study to compare the functional outcome of group 1 clavicle fractures treated with anatomic locking plates (ALP) and Titanium elastic nail (TEN).
Materials and methods
We studied patients presenting with displaced midshaft clavicle fractures treated with ALP or TEN after approval from our Institutional Ethics Committee. The study period was from Jan 2013 to Dec 2016 with a minimum follow up of 12 months. It is a retrospective study. The case records of the patients were reviewed. Patients between the ages of 20 and 60 with displaced midshaft clavicle fractures with more than 2 cm of shortening, vertical displacement more than the shaft width as measured on the AP digital radiograph with the patient supine, threat of skin perforation, presenting to our hospital within 2 weeks of injury were included in the study. We excluded patients if the duration was more than 2 weeks, patients who presented with open fractures, patients with comminuted or segmental fractures (Robinson Type 2B2), patients with preexisting morbidity of the shoulder, arm or hand and patients with neurovascular injury.
All patients who met with our inclusion criteria were operated either with TEN or ALP.
In the ALP group the patient was put in a beach chair position with a folded sheet along the medial border of scapula, a transverse incision was made spanning the fracture, dissection was carried down to the fracture, followed by a careful subperiosteal dissection. The fracture was reduced and stabilized with an ALP, in oblique fractures an interfragmentary lag screw was used in addition to achieve compression and give a more stable fixation. The fascia and skin were closed in layers. (Figure 1).
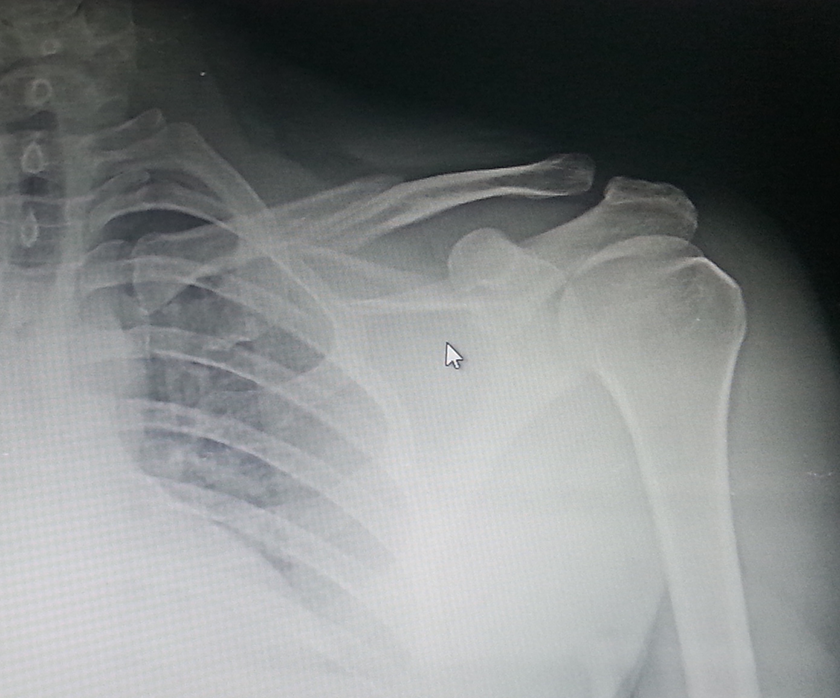
Preoperative radiograph ALP.
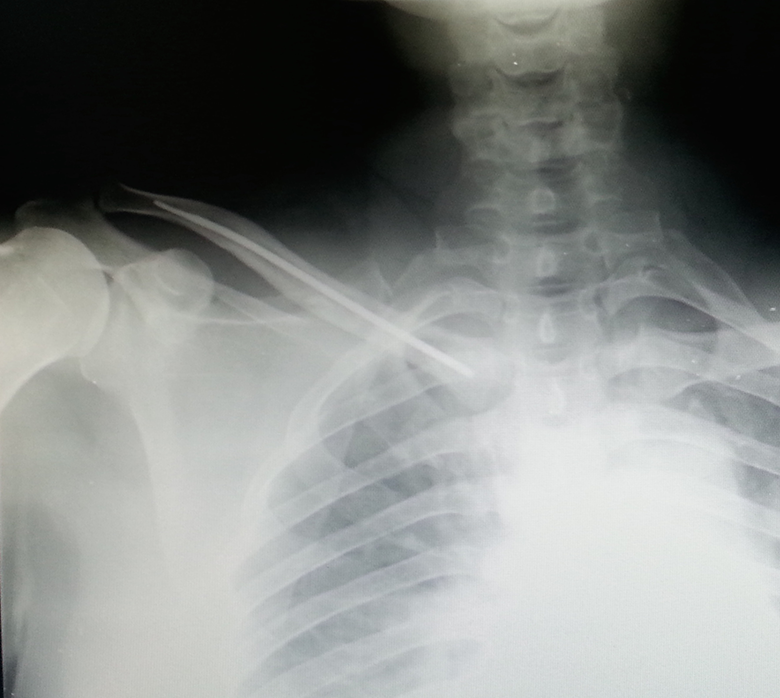
In the TEN group, patients were placed in the supine position. The sternoclavicular joint was palpated and marked. Using the image intensifier, the point of entry was identified. A small incision was made 1 cm lateral to the sternoclavicular joint, then an entry in the anterior cortex of the sternal end of the clavicle was made using a bone awl. A 2–3 mm (depending on the width of the clavicle) TEN was then inserted and passed under image guidance. Closed reduction was attempted using pointed reduction forceps, under control of the image intensifier, but if the reduction was difficult, we didn’t hesitate to make a small incision(mini open) over the fracture to manipulate the fragments and achieve reduction. The nail was then inserted across the fracture site until it was just medial to the acromioclavicular joint. The nail was cut close to the entry to avoid irritation to the soft tissue later. The fascia and skin were then closed (Figure 2). Both the implants were locally manufactured implants from Sharma Surgicals.
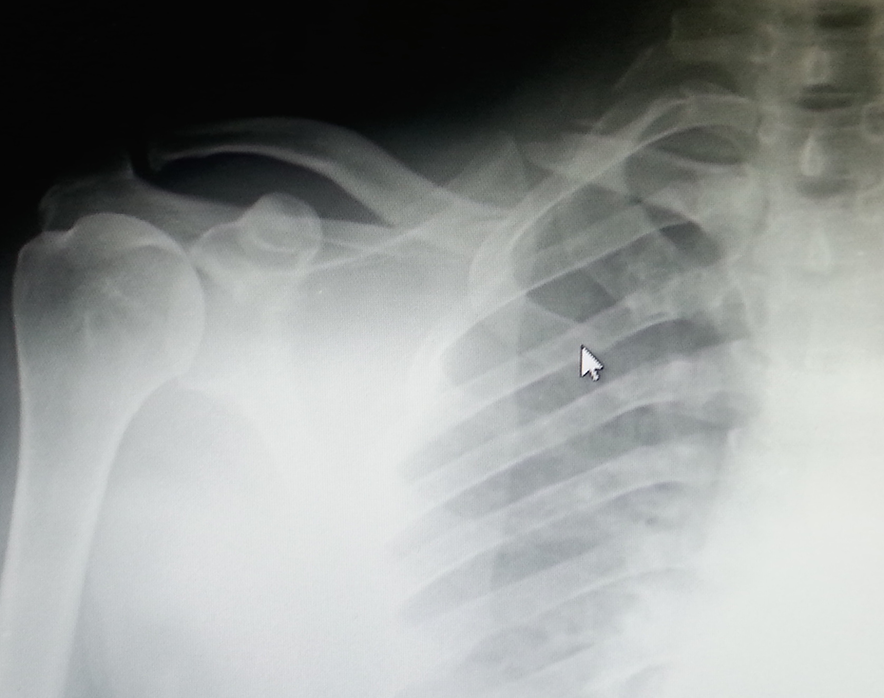
Preoperative radiograph TEN.
Post operatively the patients of both groups were given a sling for 3 weeks. They were allowed active mobilization of shoulder immediately after surgery. Patients were reviewed at 4 weeks, 8 weeks, 12 weeks, 16 weeks, 6 months and 1 year. At each visit patients were assessed for the primary and secondary outcome measures.
At each visit clinical assessment included, assessment of range of motion of the shoulder, time of clinical union; which was the absence of tenderness at the fracture site. Functional assessment was done using the quick Dash score and the Constant Murley score. Standard anteroposterior radiographs were obtained at each visit till fracture union, to assess the healing process and complications if any. Healed fracture was defined as bony callus formation/obliteration of fracture lines across 2/3rd the circumference. The time of radiological union was recorded. Secondary outcome measures included complications such as neurovascular injury, wound infection, nonunion, malunion, implant migration, medial soft tissue irritation, implant failure, refracture after implant removal and implant prominence under the skin. TEN nail removal was done after bony union in all the patients. Patient who were lost to follow up were excluded from the study. Statistical Analysis was done mean, standard deviation was calculated and two-tailed independent t test was performed for finding significance using the SPSS version 16 software. A p value < 0.05 was considered as significant.
Results
A total of 116 patients met our inclusion criteria. 62 patients were treated with TEN and 54 with ALP. There were 86 males and 30 females in the study. Most common mode of injury was fall from a two-wheeler due to a road traffic accident. The average age of the patients was 35(18 to 54) years in the TEN group and 38 years (21 to 59) in the ALP group.
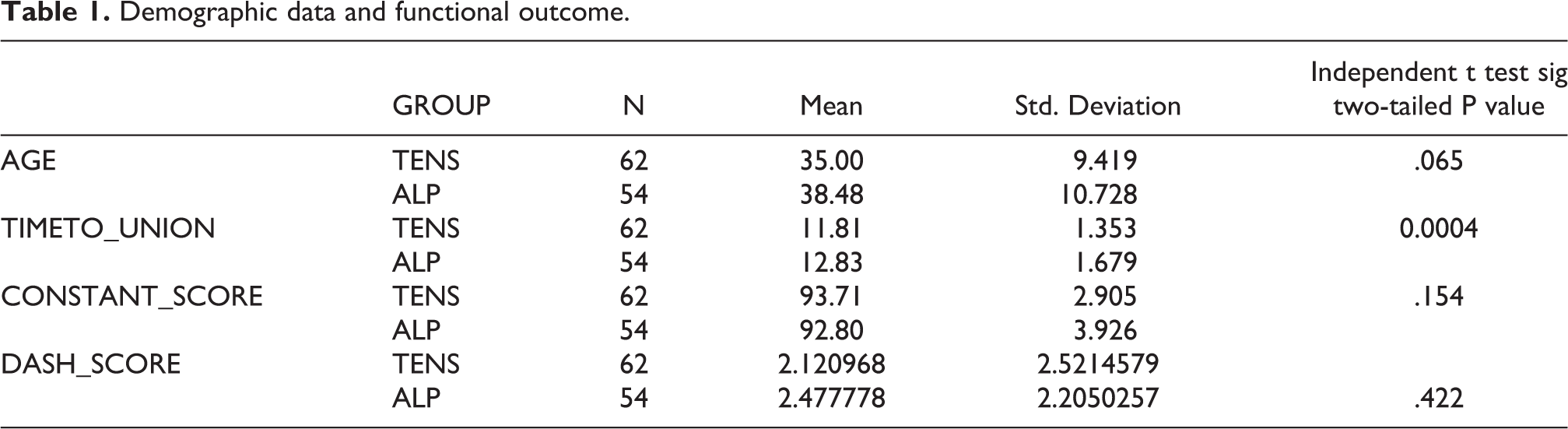
In 28 patients in the TEN group, nail was inserted after closed reduction, in 34 patients minimum open reduction was necessary to aid in the passage of the nail. Bony union was achieved at an average of 11.8 weeks in the TENS group and 12.8 weeks in the ALP group post operatively and this was found to be significant (Table 1).
Demographic data and functional outcome.
All fractures went on to unite in the ALP group (Figure 3); there was one case of superficial infection, which settled with antibiotics. There was one case of implant prominence, for which implant removal was done after fracture union. There was one case of implant being exposed for which implant removal was done in the third month but the fracture had united.
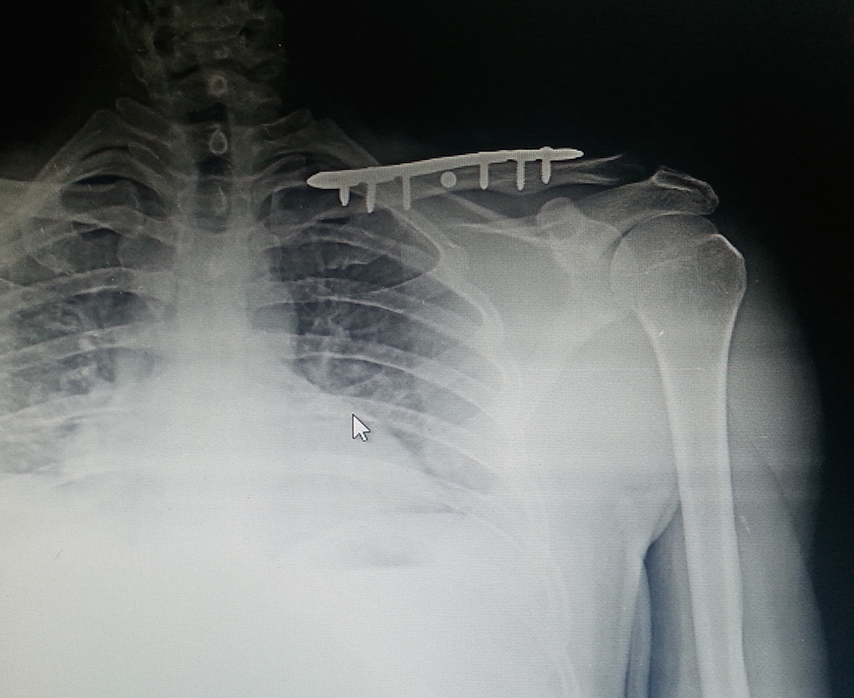
Postoperative after union radiograph ALP.
In the TENS group (Figure 4) there was one case of deep infection, who had nonunion and ultimately needed ALP fixation. Three patients had superficial wound infection and 10 cases had medial soft tissue irritation because of nail prominence at the insertion site which improved with analgesics and nail removal was done after fracture union.
Postoperative after union radiograph TEN.
In the ALP group at 1 year follow up, the mean postoperative constant score was 92.8 (range 80–97), whereas in the TENS group the mean postoperative constant score was 93.7 (82–97). This difference was not significant, p value of 0.154 (Table 1).
The mean postoperative quick dash score was 2.48 (range from 0 to 6.8) in the ALP group and 2.1 (range 0–9.1) in the TENS group. This difference was not significant, p value 0.422 (Table 1).
Both these outcome scores are suggestive of good to excellent results in most of the patients in both the groups.
Discussion
The best treatment for midshaft clavicle fractures is still debatable and limited evidence is available, regarding the effectiveness of the various methods of surgical treatment. 6,10 Anatomical clavicular plates have the advantage of being precontoured, so contouring on table is not required, thus saving time and also giving a good stable fixation. Biomechanically plate fixation is a good option as it has a better resistance to torsional and bending forces when the upper limb is elevated above the shoulder level. 11 Fixation with TEN is more physiological, has a shorter operative time and there is early pain relief, resulting in a faster functional recovery. 12 Disadvantages of the TEN include irritation at the entry site and it is preferably removed at 4–6 months post-surgery, so a second surgery is required. 12
In our comparative study, we had good to excellent result in all our patients. We did a review of literature to look at the functional outcome of both implants and found both implants have a similar outcome (Table 2).
Comparison of various studies and their outcome scores.
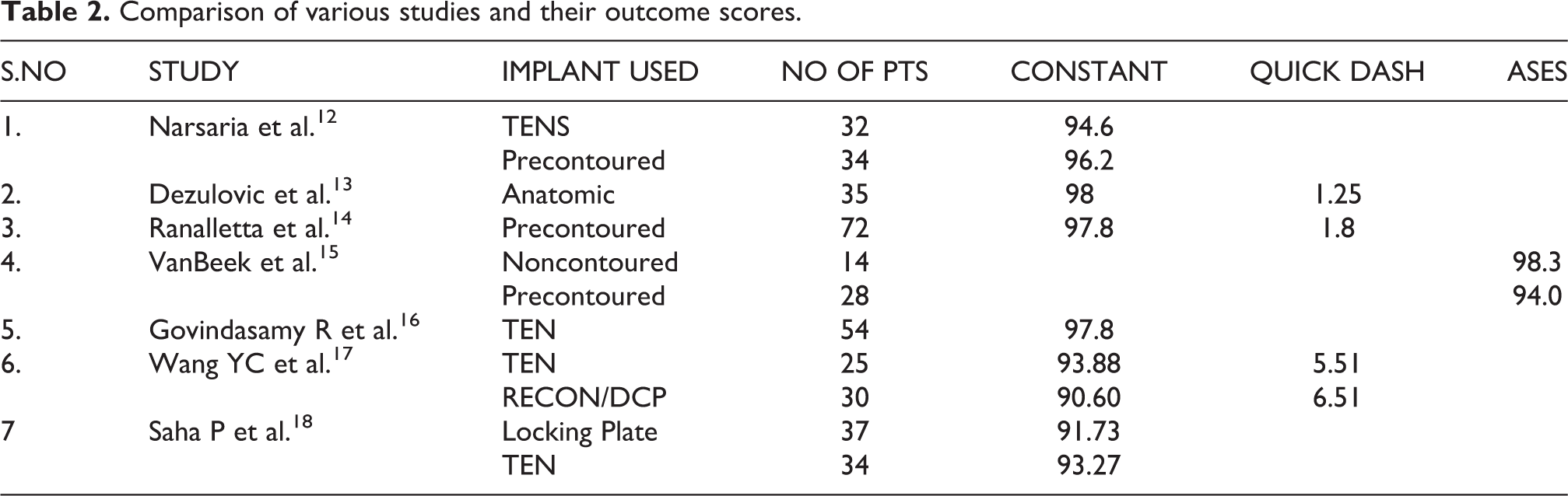
Narsaria N et al. 12 compared 32 patients treated with Titanium Elastic Nail (TEN) and 34 patients treated with precontoured clavicular plate. The Constant Murley score was 96.2 in the plating group and 94.6 in the TEN group. We had a Constant Murley score of 92.8 in the ALP group and 93.7 in the TEN group which was similar to their study. They concluded that TEN is an equally effective alternate to plate fixation. Also, Dezulovic M et al. 13 evaluated 35 patients treated with multidimensional, anatomical locking plate osteosynthesis for comminuted clavicle shaft fracture. They had a mean DASH score of 1.25 and a mean Constant Murley score of 98. They had one case of infection and no nonunion or implant failure. We also had similar results with ALP. Saha P et al. 18 prospectively compared locking plate versus TENS in treatment of displaced midshaft clavicular fracture and found similar Constant Murley scores in both groups (Table 2). The time to union was faster in the TEN group compared to the plate group. We also had a faster time to union in the TEN group.
Considering the complications, we had 1 case of superficial infection, 1 case of implant prominence and 1 case of implant being exposed in the ALP group. Ranalletta M et al. 14 evaluated 72 patients of mid clavicular fractures treated with precontoured locking plate. The average Constant Murley score was 97.8 and Quick Dash score was 1.8. They had 15 (22.1%) complications out of which 3 were major and included 1 case of subclavian vein extrinsic compression, 1 nonunion and 1 hardware loosening. The authors concluded that they had satisfactory results with low rate of complications and a low rate of hardware removal with precontoured locking plates. VanBeek C et al. 15 analysed 52 patients with mid clavicular fractures, 14 out of which were treated with noncontoured plates and 28 with precontoured plates. 9 of the 14 patients treated with noncontoured plate had hardware prominence, compared to 9 of the 28 treated with precontoured plates.
Complications were slightly higher in the TEN group in our study; with eight cases of medial irritation due to implant prominence, three cases of superficial infection and one case of deep infection. Govindasamy R et al. 16 evaluated 54 patients who underwent TEN nailing. In 24 patients the nail was inserted closed and in 30 patients minimum open reduction was done. The mean constant score was 97.8. The complications included skin irritation in 15 patients, temporary paraesthesia in 5 patients, superficial skin infection in 3 patients, implant migration and perforation of the lateral cortex in 1 patient and delayed union in 1 patient. All fractures went on to unite. Wang YC et al. 17 analysed 25 patients treated with TEN and 30 patients treated with either Recon (reconstruction plate) or DCP (dynamic compression plate). Both group of patients had similar constant and DASH score (Table 2) which was not significant statistically. The authors concluded that TEN fixation produced similar functional results as plate fixation, with some shortening when used in comminuted fractures but this did not affect the functional outcome. We had excluded comminuted fractures in our study.
Lenza M et al. 6 in 2015 published a review of surgical interventions for treating acute fractures or nonunion of the middle third of the clavicle. The authors concluded that only very low quality and limited evidence is available on reviewing randomized controlled trials regarding the effectiveness of different methods of surgical fixation of fractures and nonunion of the middle third of the clavicle. Hussain N et al. 19 did a systematic review and meta-analysis of Intramedullary nailing versus plate fixation for clavicle fractures. They concluded that intramedullary nailing had a similar functional outcome and rate of treatment failure when compared to plate fixation. However, complications not requiring surgery were higher in the plate group. Intramedullary nailing may be a viable alternative, as it is more cost effective due to the reduced operating time.
The limitation of our study are that it was a retrospective study, additional details like the duration of surgery, pain scales could have been added. Future randomised controlled trials with larger number of patients may help settle which implant is superior for these fractures.
Conclusion
Both ALP and TEN are good options for the treatment of mid clavicular fractures as they have similar functional outcome as seen in our study. Either device can be used for fixation of mid clavicular fractures. TEN nail insertion has the advantage of being minimally invasive, having a faster union time and may be recommended in midshaft clavicle fractures without comminution.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.