
Abstract
Background:
Neer type 2 distal clavicular fractures are associated with poor outcomes after nonoperative management. Surgical management is preferred, and various fixation methods have been studied.
Purpose:
To assess the clinical and radiological outcomes in patients with unstable distal-end clavicular fractures that were treated with hook plate (HP) or arthroscopically assisted coracoclavicular (AAC) fixation.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively compared the clinical and radiological results of HP versus AAC fixation in patients who had unstable lateral-end clavicular fractures and at least 2 years of follow-up. The recorded postoperative Constant score, American Shoulder and Elbow Surgeons score, and shoulder forward flexion were compared between treatment groups using the independent t test. Fracture union was evaluated on routine shoulder radiographs.
Results:
This study included 34 patients (17 with HP fixation, 17 with AAC fixation) with a mean ± SD age of 36.4 ± 8.3 years for the HP group and 37.2 ± 6.9 years for the AAC group. The mean follow-up period was 30.8 ± 2.8 months for the HP group and 28.8 ± 3.01 months for the AAC group. No statistically significant difference between groups was observed regarding postoperative Constant score (89.7 vs 92.5; P = .07), American Shoulder and Elbow Surgeons score (88.2 vs 91.1; P = .12), or mean time to union (10.1 vs 9.3 weeks; P = .16). Postoperative shoulder forward flexion was better in the AAC group (168.2° ± 4.3°) versus the HP group (161.9° ± 6.6°; P = .002), and the complication rate was lower in the AAC group (5.8% vs 41.1%; P = .03).
Conclusion:
Both the AAC and HP fixation methods were effective in the surgical fixation of unstable Neer type 2 lateral-third clavicle fractures, with successful functional and radiological outcomes. However, AAC fixation provided an earlier return to work with fewer complications.
Adult clavicular fractures account for 2.5% to 4% of all fractures and 35% of shoulder fractures. 21 Fractures of the distal-third clavicle are responsible for 15% to 25% of all clavicular fractures, with approximately 25% of these fractures being unstable. 16 –18,23 Distal-end clavicle fractures usually result from high-energy trauma, with motor vehicle accidents and sports-related injuries being the most common mechanisms in young adults. 25
Neer classified distal-third clavicle fractures into 5 types: 1, fractures located lateral to the coracoclavicular (CC) ligaments; 2, fractures that are medial to (2A) or between the insertion of CC ligaments (2B); 3, fractures that are lateral to ligaments that extend to the acromioclavicular (AC) joint; 4, epiphyseal separation in skeletally immature patients; and 5, comminuted. 30 Neer type 2 fractures are considered unstable because of the disruption of CC ligaments and the presence of strong deforming forces. 23
Nonoperative treatment is usually reserved for stable fractures. Difficulty in maintaining fracture reduction and the associated high rate of nonunion are the main contributors to unsuccessful nonsurgical management of Neer type 2 fractures. 14,27,31 Surgical treatment is advocated for unstable lateral-end clavicle fractures (Neer type 2) to maintain the adequate fracture reduction necessary for union and minimize the complications associated with nonoperative management, such as malunion, nonunion, chronic shoulder pain, and shoulder asymmetry. 24
The small size of the distal fragment, comminution, and disruption of CC ligaments are the major challenges for surgical fixation of such fractures. A variety of surgical options have been utilized for fixation, such as Kirschner wires, hook plate (HP), locked plate, and arthroscopically assisted CC (AAC) fixation, with no consensus on which is the best. 1,2,8,10 HP fixation provides a simple and easily applicable method of fixation for most orthopaedic surgeons. 11 However, it is associated with many adverse effects related to the presence of the hook in the subacromial space, which needs plate removal after complete fracture union. 26 The minimally invasive AAC fixation technique has been recently introduced as a method of indirect fracture reduction utilizing 2 cortical buttons. 4 The main advantages of this technique are less soft tissue stripping, no violation of the subacromial space, and no need for implant removal. 22
The purpose of this study was to compare the functional and radiological results of HP versus AAC fixation methods for patients with Neer type 2 lateral-third fracture of the clavicle. We hypothesized that patients with AAC fixation would have a lower complication rate with an earlier return to work.
Methods
This retrospective study received ethics committee approval, and all included patients provided informed consent. We reviewed the data from 37 patients with unstable lateral-end clavicle fractures who underwent surgery between August 2016 and October 2019 at 2 university hospitals. The data were obtained from the hospital registration unit as well as the patients’ medical records in December 2021. The study inclusion criteria were as follows: unstable lateral-end clavicle fracture (Neer type 2), fracture sustained for <3 weeks, and patient age ≥18 years. Patients with incomplete medical records, stable fractures (Neer types 1 and 3), open fractures, associated injuries, fractures >3 weeks, skeletal immaturity, and incomplete follow-up were the main criteria of exclusion. We divided the patients into those treated with HP fixation (Synthes) and those who underwent AAC fixation using 2 cortical buttons (TightRope; Arthrex).
Surgical Technique
All surgical procedures were performed under general anesthesia by 2 senior shoulder surgeons (F.S.F. and M.E.H.; 1 surgeon for each treatment group) with an intravenous antibiotic (cefotaxime, 1 g) administered 30 minutes before surgery. The patients were seated in a beach-chair position.
HP Fixation
The fracture was approached through a straight 6- to 8-cm horizontal incision centered over the clavicle across the AC joint laterally. After incision of the skin, subcutaneous tissue, and periosteum, the fracture was directly reduced and held with an HP. The plate was fixed to the bone through the passage of the hook behind the AC joint underneath the acromion process and the insertion of 3.5-mm cortical screws medial to the fracture. The wound was stitched in layers.
Arthroscopically Assisted CC Fixation
First, a viewing posterior portal was located 2 cm distal and 1 cm medial to the posterolateral tip of the acromion. Then, a spinal needle was used for proper placement of the anterior working portal. The rotator interval was released using a radiofrequency device, and the base of the coracoid process was cleared of soft tissue (Figure 1). Through the anterior portal, a mobile C-arm device (Zenition; Philips) was centered beneath the coracoid process, and a guide pin was drilled from the upper surface of the clavicle, medial to the fracture, exiting through the inferior surface of the coracoid (Figure 2). A 4.5-mm cannulated drill bit was passed over the inserted guide pin to make holes within the clavicle and coracoid. One cortical button of the Tight Rope fixation system was retrieved and positioned below the coracoid process, while the other button was tightened over the clavicle to reduce the fracture (Figure 3). Intraoperative fluoroscopy was used to verify the final fracture reduction.

The base of the coracoid process, C, was cleared of soft tissue using a radiofrequency probe.
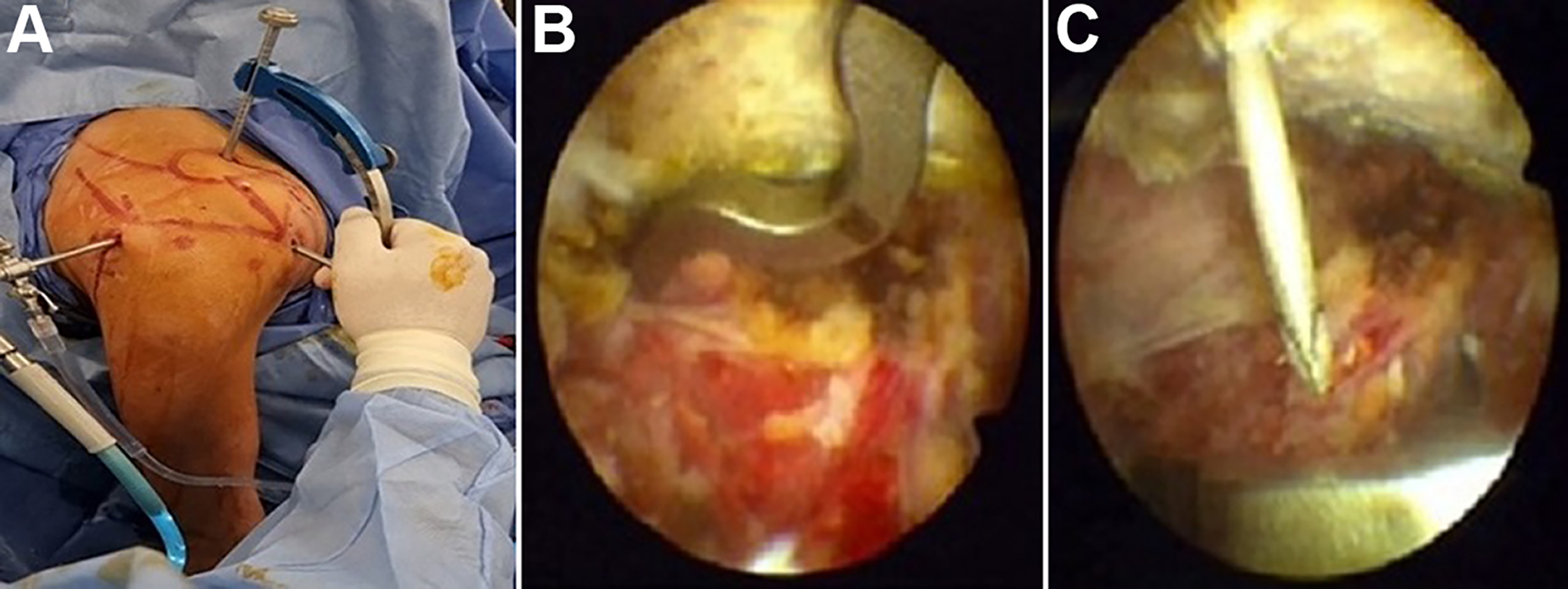
(A) Introduction of C-arm device through the anterior portal. (B) The guide system was centered below the base of the coracoid process, and (C) the guide wire exited the undersurface of the coracoid process.

The cortical button was retrieved to settle underneath the coracoid.
Postoperative Rehabilitation and Follow-up Evaluation
The rehabilitation program was the same for both techniques. The stitches were removed after 2 weeks, and the arm was immobilized in an arm sling for 6 to 8 weeks. The patients started pendular exercises on day 1 postoperatively. Active assisted motions were commenced after radiographic union (6-8 weeks), while active resistive exercises were performed after 12 weeks.
At the final follow-up, functional assessment was evaluated using the Constant score, 5 American Shoulder and Elbow Surgeons (ASES) score, 13 and shoulder forward flexion. In addition, complications were recorded, and patients were asked about their level of satisfaction and how much they recommended their surgery to other patients. Serial postoperative plain radiographs were obtained at 0, 6, 8, 12, and 16 weeks postoperatively for the evaluation of fracture union (Figures 4 and 5).

(A) Preoperative anteroposterior view radiograph of a 28-year-old man who had an unstable distal-third clavicle fracture that was fixed using a hook plate. (B) The patient achieved full radiographic union at 4 months postoperatively.

(A) Preoperative anteroposterior view radiograph shows a Neer type 2 lateral-third clavicle fracture. (B) The fracture was indirectly reduced and fixed using arthroscopically assisted double-button cortical fixation with (C) complete radiographic union achieved at 3 months postoperatively.
Statistical Analysis
The SPSS data editor (SPSS for Windows Version 25; IBM) was used for statistical analysis. The numerical values were presented as means and standard deviation, with the calculation of a 95% confidence interval for means. First, the normality of data distribution was checked using the Kolmogorov-Smirnov test. A 2-sided independent t test was used to estimate the difference in the quantitative variables between the treatment groups. The difference in qualitative or categorical data was estimated using the Fisher exact test. P value < .05 was set as the threshold for statistical significance.
Results
Of the initial 37 patients, we excluded 2 who had incomplete medical records and 1 who was lost to follow-up, leaving 34 patients. Of these patients, 17 were treated with HP fixation and 17 underwent AAC fixation. The mean age was 36.4 years (range, 23-52 years) for the HP group and 37.2 years (range, 24-48 years) for the AAC group, and the mean ± SD follow-up time was 30.8 ± 2.8 months (range, 26-36 months) in the HP group and 28.8 ± 3.01 months (range, 24-33 months) in the AAC group (P = .06). Table 1 shows the characteristics of the patients in each treatment group.
Demographic Characteristics of the Treatment Groups a
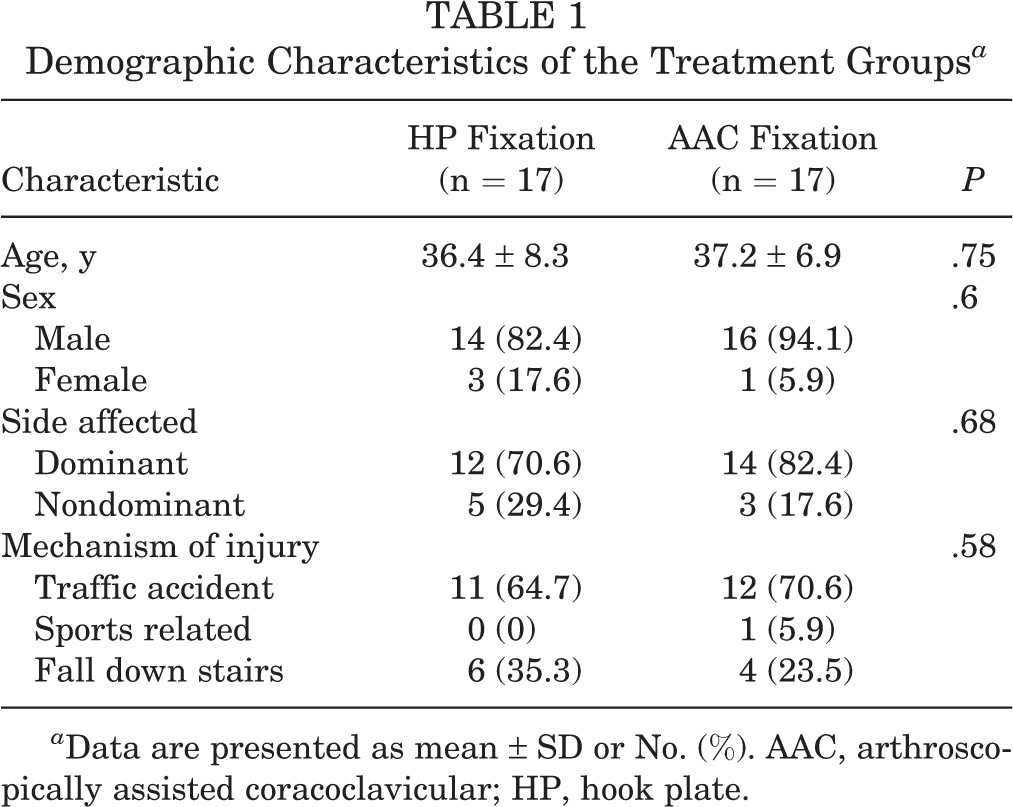
a Data are presented as mean ± SD or No. (%). AAC, arthroscopically assisted coracoclavicular; HP, hook plate.
There were no significant differences between the HP and AAC groups in terms of time before surgery (3.1 ± 1.57 days [range, 1-5 days] vs 3.8 ± 1.4 days [range, 2-7 days], respectively; P = .18) or surgery duration (49.3 ± 7.3 vs 52.9 ± 6.3 minutes; P = .13). The reported mean time of postoperative hospital stay in the AAC group was 2 ± 0.8 days, which was significantly shorter than the HP group (3.4 ± 1.1 days; P = .0001).
The postoperative Constant scores were considered excellent (HP, n = 12; AAC, n = 16) and good (HP, n = 5; AAC, n = 1), with no statistical difference between groups (Table 2). Similarly, there was no significant difference in ASES score between the groups. Significantly better postoperative forward flexion was seen in the AAC group versus the HP group (168.2° ± 4.3° vs 161.9° ± 6.6°, respectively; P = .002) (Table 2).
Final Functional and Radiological Results for the Treatment Groups a

a Data are presented as mean ± SD (95% CI) or No. (%). AAC, arthroscopically assisted coracoclavicular; ASES, American Shoulder and Elbow Surgeons; HP, hook plate; NA, not applicable.
b Bold P values indicate statistically significant difference between groups (P < .05). P values are based on an independent t test unless noted otherwise.
c Fisher exact test.
All patients achieved full radiographic union, with no statistically significant difference between groups in the time to achieve union (Table 2). After fracture healing consolidation, all patients in the HP group underwent routine plate-removal surgery. All patients returned to their preoperative levels of activity and occupations without any functional deficits, but the mean time for resuming work was significantly shorter in the AAC group than the HP group (11.2 ± 1.9 vs 17.05 ± 5.1 weeks; P = .0001).
The AAC group had only 1 patient (5.8%) with superficial wound infection, while the HP group had 7 (41.1%) with major complications that required a second operation to remove the plate: 1 case of deep infection, 3 cases of prominent hardware, and 3 cases of subacromial impingement. The degree of satisfaction was 100% in the AAC group and 58.8% in the HP group (P = .007).
Discussion
In this retrospective study, we found comparable clinical and radiological outcomes between the HP and AAC fixation groups at a minimum 2-year follow-up and better shoulder elevation (P = .002), faster return to work time (P = .0001), better satisfaction (P = .007), and a lower complication rate (P = .03) in the AAC group. The findings corroborated the study hypothesis.
Lateral-end clavicular fractures with concomitant CC ligament disruption are inherently unstable injuries that require surgical fixation to achieve fracture union, avoiding the unsatisfactory functional outcome that is associated with nonoperative treatment. 12 The surgical fixation of unstable distal-end clavicular fractures remains a difficult problem for orthopaedic surgeons. Locked plate or HP, Kirschner wires, CC screws, suture anchors, and tension band wiring are all examples of traditional fixation methods. 3 Although these techniques provide successful union, they have been associated with various morbidities, such as prominent hardware, implant failure, infection, and arthritis of the AC joint, that require another operation for hardware removal. 20 In 2007, Nourissat et al 19 introduced AAC fixation using double cortical buttons (originally described for AC joint dislocation) for the surgical fixation of Neer type 2 distal clavicular fractures. Minimal soft tissue dissection, low profile hardware, and detection of other intra-articular injuries are the main benefits of the arthroscopic technique.
Our study aimed to contribute to the few previously published studies that compared the outcomes of HP versus AAC fixation for unstable lateral-third fracture clavicle. Only 2 comparative studies were found, both in a recent systematic review by Yagnik et al. 29 The most common mechanism of injury in our study was high-velocity trauma, including road traffic and falling injuries (33 patients, 97.1%), which is consistent with the findings of Flinkkila et al, 7 who reported that 90% of injuries in their study were related to road traffic accidents and falling injuries (36 of 40 patients).
We recorded a mean time before surgery of 3.1 days for HP and 3.8 days for AAC fixation. Additionally, the mean surgical time was 49.3 minutes for HP and 52.9 minutes for AAC fixation. Xiong et al 28 estimated a total mean time before surgery of 3.5 days with a longer operative time than that in our study (84 minutes for HP and 108 minutes for AAC). Flinkkila et al 7 reported a longer delay before surgery, 6 days in the HP group and 4 days in the AAC group, with a comparable mean operative time (45 minutes for HP and 49 minutes for AAC). No studies have compared the mean postoperative hospital stay between the treatment groups. The AAC fixation group had a significantly shorter postoperative hospital stay (P = .0001).
Regarding the postoperative Constant score, no statistically significant difference was found between treatment groups at the final follow-up (89.7 ± 4.7 for HP and 92.5 ± 4.07 for AAC). Similarly, Flinkkila et al 7 found no statistically significant difference in the last postoperative Constant score (89 ± 9 for HP and 93 ± 7 for AAC; P = .21). Xiong et al 28 estimated a total postoperative Constant score of 90.2 ± 12.2 in 58 patients treated with HP, anatomic plate, and arthroscopic EndoButton fixations, with no statistically significant difference between the treatment groups.
There was also no statistically significant difference in postoperative ASES score between the HP and AAC groups (88.2 ± 5.2 vs 91.1 ± 5.4, respectively). Erden et al 6 treated 47 Neer type 2 clavicular fractures with anatomic locked plate and AAC fixation and calculated a postoperative ASES score of 92.5 ± 3.9 for the locked plate group and 95 ± 3.3 for the AAC group, with no statistically significant difference (P = .32). Kapicioglu et al 9 reported a postoperative ASES score of 92.6 ± 3.2 in 17 patients treated with AAC fixation, which is close to the findings of our study.
There were no patients with nonunion or implant failure in our study, and all patients achieved complete fracture healing. No difference between treatment groups was found regarding time to union (10.1 ± 1.3 weeks [HP] vs 9.3 ± 1.8 weeks [AAC]; P = .16). Flinkkila et al 7 did not record the mean time to union in the HP or AAC fixation group and reported 2 cases of nonunion, 1 in each treatment group. Erden et al 6 estimated a comparable mean time of union in each treatment group (10.9 ± 1.1 weeks for the locked plate group and 9.7 ± 1.7 weeks for the AAC fixation group), with no documented cases of nonunion. Xiong et al 28 recorded 1 case of nonunion among 28 patients treated with arthroscopically assisted EndoButton fixation, with no estimated mean time of union for each treatment group.
The main deficiency of HP is the necessity of another operative procedure to remove the implant. 26 Given the requirement of plate extraction, patients in the HP group had a longer time to return to work, with a reported mean 17.05 ± 5.1 weeks as compared with 11.2 ± 1.9 weeks in the AAC group at the last follow-up. This aspect has not been previously investigated in the published comparative studies. According to Erden et al, 6 patients in the locked plate and AAC fixation groups resumed their daily activities between 6 and 12 weeks after surgery.
We recorded a significantly higher rate of complications in the HP group than the AAC fixation group (41.1% vs 5.8%). The complications in the HP group included 1 patient who developed a deep infection, 3 with plate prominence, and 3 with subacromial impingement that required plate removal after fracture healing. Only 1 patient in the AAC fixation group had a mild superficial skin infection that was resolved with repeated wound dressing and antibiotics. Flinkkila et al 7 found no statistical difference in the complication rate between the HP and AAC fixation groups (15.7% vs 9.5%, respectively), but all patients in the HP group required another operation for plate removal. A meta-analysis by Oh et al 20 reported a complication rate of 40.7% in 162 patients treated with HPs. Motta et al 15 revealed no complications in 14 patients treated with AAC fixation.
Limitations
Numerous limitations were identified in our research. First, the number of included patients was small because of the rarity of this injury. A post hoc analysis demonstrated that our statistical power was 57%, and each group needed at least 26 patients to achieve 80% power and a significant size difference in the primary outcome measurements. Second, this study was retrospective, and prospective studies are recommended to select a proper sample size that gives the required statistical power and minimizes the selection bias. Additionally, a longer follow-up period is needed to detect the development of remote complications such as AC joint arthritis. The accuracy of fracture reduction in the anteroposterior plane after AAC fixation was not investigated using a postoperative computed tomography scan. Finally, AAC fixation is a technically demanding procedure that is challenging for most orthopaedic surgeons and cannot be securely performed in fractures extending to the buttonhole.
Conclusion
Although both the AAC and HP fixation methods provided comparable fracture union and improvements in postoperative shoulder functional scores, with no statistical difference at a minimum 2-year follow-up, AAC fixation was superior in terms of postoperative hospital stay, forward flexion of the shoulder, complication rate, and time to resume work.
Footnotes
Final revision submitted August 4, 2022; accepted August 30, 2022.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Zagazig University Hospitals (No. 974/13-12-2021).