
Abstract
The health informational practices of Indigenous community members living in urban areas remain understudied in Quebec (Canada), despite their importance given rapid population growth and unmet needs. These practices became even more crucial during the COVID-19 pandemic, when many health services were disrupted. In collaboration with the Native Friendship Centre of Lanaudière, this study explores how Indigenous people living in urban settings in Quebec accessed, interpreted, and used health information during the pandemic. We conducted 24 in-person qualitative interviews between September 2021 and February 2022 and analyzed the data through a thematic content analysis, guided by the concept of trust as a relational and subjective construct. This project was not conducted under the OCAP® (Ownership, Control, Access, and Possession) principles, as it focused on individual lived experiences of urban Indigenous participants in collaboration with a community partner, without involving collective data governance mechanisms.
Findings show that informational practices were diverse and multifaceted, combining multiple media sources with a preference for locally shared information through social networks and community organizations. It is important to underscore that participants’ mistrust of government sources cannot be attributed solely to the COVID-19 infodemic. While media saturation and the dissemination of contradictory messages contributed to uncertainty, this mistrust is also deeply rooted in the ongoing impacts of settler colonialism, including systemic racism, intergenerational trauma, and experiences of exclusion and harm within the health system. This structural context continues to shape how information is received, interpreted, and acted upon. The study underscores the need to approach informational practices through a lens that centers Indigenous lived realities, historical memory, and self-determination.
Keywords
Introduction
In Quebec (Canada), more than half of the Indigenous population (55.6%) lives in cities (1). The urban population is highly diverse and includes members of First Nations (there are 10 First Nations in Quebec), Métis, and Inuit. Members of Indigenous communities living in urban areas experience unique situations as they are confronted with discrimination and various health challenges arising from social inequalities and structural issues (e.g. systemic racism, discrimination, lack of access to culturally safe care, etc.) (2). During public health crises, such as the COVID-19 pandemic, individuals within marginalized groups frequently find themselves disproportionately affected by illness (3). During the pandemic, many Indigenous community members also needed to conform to both the measures implemented by the Quebec government and those put in place in their communities (4).
Indigenous community organizations raised concerns regarding information overload and misinformation encountered by Indigenous communities living in urban areas, which could sometimes result in preventive practices being disregarded. The COVID-19 pandemic was marked by a continuous flow of information, leading the World Health Organization to describe it as an ‘infodemic’ (5). This surge, across both traditional and social media, fueled the viral spread of misinformation and disinformation about the pandemic (3 –6). Misinformation refers to erroneous information disseminated with no intention to deceive or harm, while disinformation implies a malicious intent (7). During the pandemic, both, combined with information overload, have contributed to confusion, anxiety, risky behaviors, and distrust toward health authorities (5 –8). Therefore, the main objective of this project is to explore informational practices of Indigenous community members living in urban areas.
Informational practices refer to how people engage with information, through devices, sources, tools, and cognitive strategies, across contexts of searching, processing, and evaluating information (9). These practices are embedded in social and cultural realities and focus on how users concretely access and use media to obtain health information (10,11). Closely tied to the notion of informational reflexivity, they also involve how individuals and communities assess the credibility, legitimacy, and relevance of information, highlighting the collective and conversational dimensions of information evaluation (12,13).
A few studies have examined the health informational practices of Indigenous people in Canada. One study identified five common themes guiding the health informational practices among three different Indigenous Nations in Ontario: the value of experiential knowledge; the influence of community structure on the dissemination of health information; the preference for messages generated within the community (including culturally appropriate languages and symbols); the importance of family and community networks in the dissemination of health information; and the local effects of colonization on Indigenous knowledge systems, which vary from Nation to Nation (14). The availability of visual information, the accessibility of the experiences of people in similar situations, the possibility to remain anonymous, and the absence of stigma associated with more sensitive health topics are features appreciated by Indigenous community members (15 –17). Different social media platforms, such as Facebook, are also frequently used (15 –17). In addition, the importance of local news sources, specifically community radio, in Inuit informational practices in Nunavik is also highlighted (16). This preference for local and community-based information happens in a context where the lack of consideration of Indigenous communities and their issues by traditional media are documented (18). Despite their importance in terms of population and their particularities, the health informational practices of members of Indigenous communities living in urban areas have never been studied in Quebec. Health informational practices play an even more important role in the context of a pandemic, when many services are no longer accessible.
Methods
Research team positionality and community engagement
During the COVID-19 pandemic, Indigenous community organizations faced significant challenges in reaching their members, particularly those in vulnerable situations. Many organizations noted that public health messages were not adequately reaching their communities. These challenges required numerous adjustments on the part of organizations to better respond to the needs of their members. This project emerged from those concerns and was developed in close collaboration with the Native Friendship Centre of Lanaudière (NFCL). The NFCL is an Indigenous community-based organization. Its objective was to support the development of more culturally appropriate and community-relevant public health messaging. The project included two components: an exploratory phase, presented in this article, and a series of co-design workshops aimed at developing a practical tool for public health and community use (19). Community partners played a central role throughout the research process. They were involved at every key stage, including project design, the development of data collection tools, the interpretation of findings, and participation in co-design workshops. However, due to the constraints of the COVID-19 pandemic and the heavy workload faced by community organizations during this time, the level of direct involvement varied across partners.
The research team was led by a White, non-Indigenous researcher from Université Laval, Quebec City, Canada and included White team members and one Afro-Caribbean member. While the project was not Indigenous led, it was informed by ongoing and sustained engagement with Indigenous partners. We recognize the limitations of our positionality and acknowledge as a structural failure the absence of Indigenous governance and the lack of a formal ‘Ownership, Control, Access, and Possession’ agreement (OCAP®). Nonetheless, we endeavored to align with its principles by prioritizing transparency, ongoing consultation, access to research findings, and tangible community benefits notably through the co-development of a tool. Insights from the exploratory phase directly informed the co-design workshops, resulting in a practical tool that is freely available and has been widely disseminated through partner networks (19).
Study design
This research is grounded in the field of sociology of uses (20). We employed exploratory qualitative methods through individual interviews. Participants were recruited with the assistance of employees from the NFCL, as well as the Native Friendship Centre of Montréal (NFCM), and the Southern Quebec Inuit Association (SQIA), who shared the project with their members during interventions and through the centers’ Facebook pages. To participate in the study, participants needed to be 18 years of age or older, belong to a Canadian Indigenous community, and live in an urban area. Interested participants could contact the research team via phone or email or visit the community organization during the hours specified in the messages, which led to a convenience sample. Verbal or written informed consent was obtained prior to participation, using clear and accessible language. Participation was entirely voluntary, and participants were informed they could withdraw at any time without consequence. As members were not comfortable with remote interviews, they were conducted in person, and preventive measures were applied. Financial compensation of $30 was given to all participants for their time and expertise. In total, 24 in-person interviews were conducted between September 2021 and February 2022 at the NFCL (Joliette), the NFCM (Montreal), and the SQIA (Montreal).
Each interview lasted approximately 1 h. The participants could choose the language of the interview and conduct it in their native language with the assistance of an interpreter. However, all interviews were conducted in English or French according to the participants’ preference.
Each interview was documented with a report detailing the interview conditions, the flow of discussion, the main themes discussed by participants, and the interview’s personal reflections. These reports also served as reflective notes, aiding the interviewer in becoming aware of potential biases.
The interviews explored participants’ information sources, credibility assessments, changes in practices due to the pandemic, impacts on health behaviors, and informational needs. All interviews were audio recorded and transcribed in their original language (French or English).
We conducted a thematic content analysis using NVivo Pro software (version 1.7.1). This method refers to the transposition of a given corpus into a number of themes representative of the content being analyzed, with respect to the research focus (21). The main analytical categories were guided by the theoretical framework, while the sub-themes were inductively derived from the interview data and iteratively refined through team discussions. Verbatims were classified into these six main themes: informational practices; information appropriation; reflexivity; health behaviors; information and communication behaviors; and context. Each main theme encompasses sub-themes (see supplemental file for detailed codification). An initial codification was performed by A.B. and revised by M.V. Ambiguous extracts were discussed between A.B. and M.V. to reach consensus on their meaning and coding. Although participants were given the opportunity to review their full transcripts, few responded favorably to this option. This limited engagement was likely due to the constraints of the pandemic, which made follow-up communication particularly challenging. Given the urgency of the situation, key themes were instead validated in community meetings and during co-construction workshops, allowing for collaborative interpretation of findings and correction of any misrepresentations. To maintain a record of methodological and analytical decisions, a logbook was kept, and the research team met once a week to discuss methodological challenges and potential biases.
For the writing of this article, French quotes were translated into English by the research team and revised by an external professional translator. The research project has been approved by the CIUSSS du Centre-Sud-de-l'Île-de-Montréal ethical board (Project 2022-829).
Results
Participant profiles
In total, 15 men and 9 women participated in our study. Most of them lived in Montreal (14) and Joliette (6) and were between 30 and 59 years of age (15). Seven were under 30-years old, and two were 60-years old and over. They were from a variety of cultural origins: Atikamekw (6), Cri (6), Inuit (5), Métis (5), Ojibwe (1), and Innu (1). Among them, 3 were unilingual, 15 were bilingual, and 6 were trilingual or more (Table 1).
Participants’ sociodemographics.
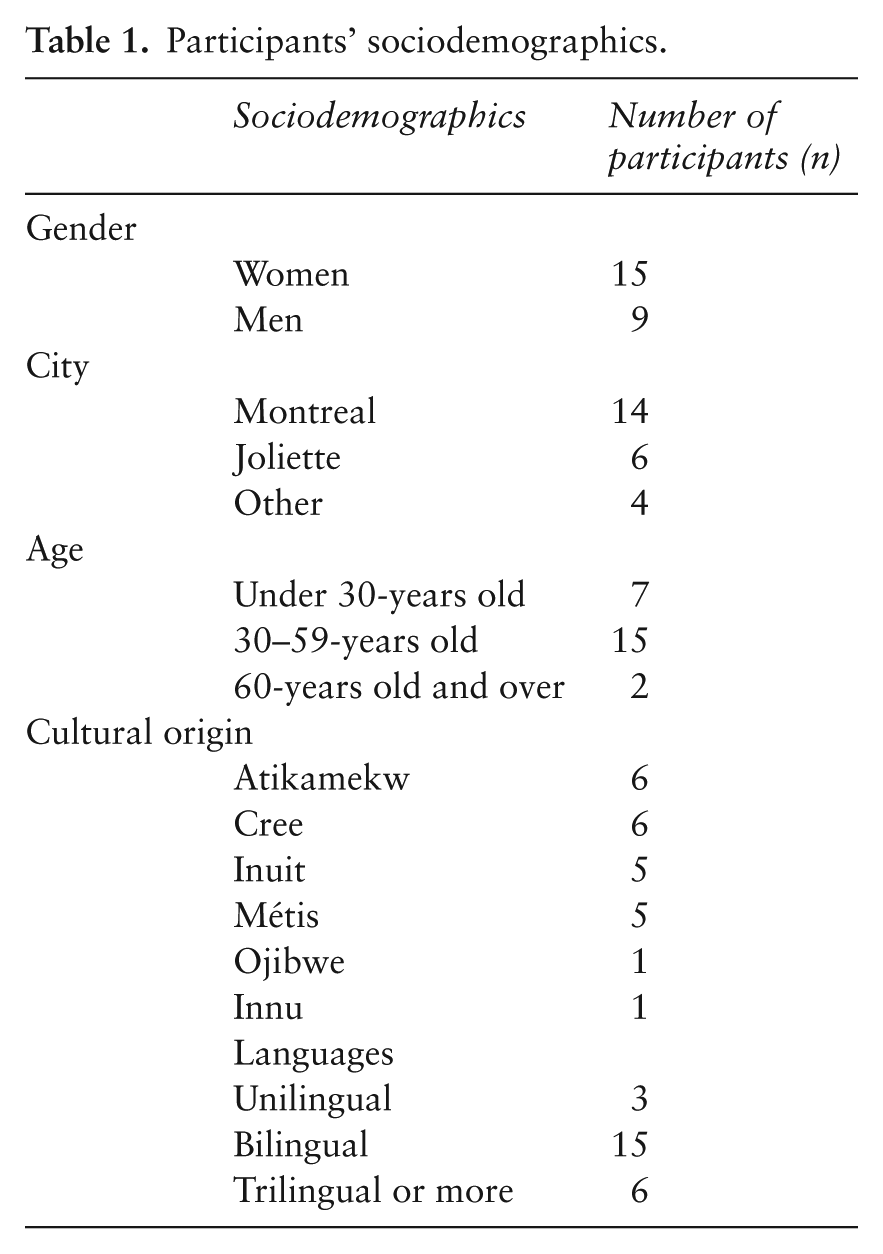
Most participants were navigating complex and often precarious economic and social conditions: 15 were unemployed, and some were experiencing homelessness or living in transitional housing through community organizations. Several also shared health challenges such as diabetes, being on a kidney transplant list, or undergoing detox treatment. However, these significant social and economic challenges were not the only defining aspects of their experiences. As presented in the following results, participants demonstrated important forms of resilience, adaptability, and agency in their informational practices.
Informational practices
Information supports diversity and accessibility
First, the devices used by participants to access news were, in decreasing order, television, cell phone, computer, and radio. For some participants, television and computers were available when they visited their community organization or friends’ homes (n = 4), and they would ask to use them to access news. One participant stated, ‘I don’t have TV at home but when I’m at the Friendship Centre. . . [. . .] We always ask to put on the news and that’s how I get it too, on TV (participant 64)’. On the contrary, one participant mentioned that at home, the television is on all day. In addition, some participants did not own a cell phone (n = 2), and many did not have access to the internet. The frequency of information consumption therefore varied significantly from one participant to another. However, most participants consulted information sources every day, and in some cases, multiple times a day. A few participants mentioned that they had decreased the frequency of their information consumption to reduce their anxiety.
Second, there were multiple sources of information related to COVID-19. Participants consulted traditional media, whether they were international (n = 5), national (CBC) (n = 12), provincial (TVA, LCN, Radio-Canada, Toronto News) (n = 9), or Indigenous (CBC Iqaluit, Nunatsiaq News) (n = 5), on television or online. Many participants also mentioned social media, primarily Facebook. The following quote from a participant reflects in a way the vast range of sources:
[. . .] it’s more the news, TV, Facebook, because there is still news on Facebook that come up regularly, so. . . [. . .] a bit everywhere, I would say. [. . .] journalists from TVA, Radio-Canada. But there are friends who post news that they have seen, but it’s a lot of news from journalists (participant 38).
Participants sought information from community organizations, such as Friendship Centers, recognizing them as trusted and accessible sources about the pandemic (on site or via Facebook). Other sources of information included family (n = 11), friends (n = 6), and people in general (n = 7). A number of participants also consulted community members, family, and Elders as important sources of information about COVID-19. One participant mentioned being kept informed by his ‘grandfather’, adding, ‘He’s not really my grandfather, but I call him my grandfather all the same. Because he’s an Elder. And what’s more, he’s an Elder who’s respected in the community’ (participant 37). As for government websites, they were generally not consulted very often, although some participants did access them for practical questions related to travel and current restrictions. A few participants mentioned having listened to some of the press conferences given by the Quebec government.
Generally, even though participants consulted multiple sources to stay informed, they claimed that they did not actively engage in seeking information about COVID-19; they opted for the information presented to them instead. Looking up concrete and practical information related to daily life (such as store opening hours) through Google or a friend seemed to be the exception. Seeking information on the internet was sometimes considered difficult: ‘Well, when I try to do searches on the internet, I can’t seem to find anything (laughs). [. . .] That’s why I wasn’t interested in going on the internet to see where we’re at with COVID-19’ (participant 30). However, several participants intentionally shared information with their networks, especially via Facebook, aiming to raise awareness about vaccination benefits, risks, or preventive measures.
Information appropriation
Information was consulted in English, Cree, Inuktitut, and, to some extent, French. While only a few participants spoke French, non-French speakers did not encounter difficulties finding information in English in Quebec. Several participants preferred to receive information in English and also consulted news in their mother tongue to stay informed about the situation in their community. Some expressed a preference for information in their mother tongue, especially to ensure accessibility to Elders. One participant mentioned that she understood English information and asked her partner when she didn’t understand messages in French.
Most participants considered that the information was clear, especially the instructions on how to protect themselves from the virus. For some, information was challenging to understand at times. Referring to the statements shared by doctors in the media, one participant mentioned: ‘There are things I don’t understand in their words because sometimes they use words that are so complex that we don’t understand’ (participant 37).
Information evaluation methods
Several methods were employed to evaluate the information consulted such as seeking a diversity of sources for obtaining a variety of points of view. For many, information gained credibility if it was shared by multiple sources; for example, one participant asserted: ‘When everyone says the same [thing], okay, but when the reports are contradictory on one side or the other, well then it comes with more questioning’ (participant 38). Others were confident that, having consulted this variety of information, they were better able to rely on their own judgment to sort through it: ‘Anyway, I’ve heard a lot of things and all, so I’ve sort of, I’ll form my own point of view’, said another participant (participant 47).
Information shared by family, friends and Elders was considered reliable, as it came from trustworthy individuals who spoke from their experiences. Similarly, community organizations, providing support to their members in various aspects, appeared to be a credible source. Several participants emphasized the role of the Friendship Center in their acceptance of the vaccine. One of them said in this regard:
It also helped me to trust the vaccine, because everyone was vaccinated here at some point. [. . .] So because of the Friendship Centre, well, it allowed me to trust. [. . .] Because it’s an organization that will, that helped me a lot [. . .] (participant 37).
Distrust, skepticism, annoyance, constant uncertainty
The distrust in government expressed by several participants functioned on different levels. Part of this distrust was based on an initial lack of trust in the involved stakeholders. For instance, a participant stated that his level of trust in the information provided by government representatives (on television and through public health organizations) was approximately 50%. This distrust predated the pandemic, due to historical circumstances. ‘How can you trust a government when they haven’t been trustworthy? They’ve always been like sneaky’ (participant 58), questioned a participant. Some of them had the impression that information was deliberately concealed. As a result, they questioned the independence of both the media and government representatives in the face of financial interests and decisions made at a higher level.
This distrust also explains why some individuals preferred browsing on social media platforms (Facebook, TikTok), where information was considered uncensored: ‘It’s not like the mainstream media . . . It’s raw information on TikTok,’ said one participant (participant 50). Another mentioned, ‘So TikTok is usually good, people usually post a couple of videos, and then it gets deleted, you know, then they have to post more cause it’s a never-ending battle to tell the truth’ (participant 54). While most participants appeared to be motivated by a prevailing mistrust of information published by the government or specific traditional media outlets, a few indicated completely trusting the information they shared. One mentioned, ‘I see the outbreaks and the deaths every day. It’s not made up, it’s official information. I believe in the official authorities, the government that provides us with news about these things’ (participant 43).
Another portion of this general distrust translated into various factors of skepticism related to the pandemic and its evolution. For the information shared by the media, several elements came into play, like the presence of contradictory information and the constant evolution (or even revision) of information. One participant shared the uncertainty caused by this situation: ‘To be honest, I don’t trust anything anymore. Because everything is different from one day to the next. [. . .] We just don’t know anymore’ (participant 38). She pointed out: ‘If at least, from one news channel to another [. . .] if everything were the same, then we’d be more confident. But it’s just that. . .everything’s different from one country to another’.
Furthermore, the expressed distrust distinguished itself based on what is specifically called into question (in descending order of the intensity of such distrust): the pandemic itself; its magnitude; the proposed measures; or the interests that certain stakeholders derive from the situation. For example, this participant is situated at the first end of this spectrum:
I try to stay away from those [government websites]. Cause I feel like they’re all like pushing a narrative that doesn’t really fit with like what’s happening right now. Like the entire COVID pandemic, I feel like it’s all kind of like propaganda (participant 53).
Another participant is positioned further toward the other end, questioning the financial interests behind the development of the vaccine: ‘When it comes to the vaccine, there’s a lot of money involved, I think’ (participant 49).
In addition to the distrust that was felt, feelings of irritation and uncertainty frequently recurred in the participants’ discourse. For example, information overload and repetition seemed to have created annoyance for some on a day-to-day basis.
It became disturbing to always hear about COVID-19, the statistics every morning. I heard that. . . it was everywhere, Facebook, it was even on TV everywhere, it was just about that, and how many deaths, what percentage, who’s more affected, and. . . Well, the statistics every morning. That really affected me (participant 37).
Skepticism, uncertainty, and irritation felt due to information overload sometimes led to disinterest in consulting or seeking information.
Discussion
Informational practices
Consistent with other studies, one of the main findings regarding participants’ informational practices related to COVID-19 is the multitude of sources consulted, including both traditional and digital media, people close to them, and community organizations (16 –22). Participants’ informational practices during the COVID-19 pandemic relied on their critical mindset, often privileging their own judgment, embodied experience, and people close to them, while sidelining government sources. This stance is not merely individual skepticism but reflects a collective memory shaped by colonial health policies. The history of colonial policies in Canada has deeply affected Indigenous peoples’ relationships with health institutions (23). Among government decisions rooted in colonialism that have affected the health of indigenous populations, we can mention, for instance, non-consensual medical experiments, the proscription of the Indigenous healthcare system, or the program to evacuate Inuit tuberculosis victims to sanatoriums far from the communities. The Indian Residential School system, established by the government of Canada (1880–1990) to assimilate Indigenous populations, is also responsible for intergenerational trauma among them (24). The living conditions of Indigenous peoples are still affected today by treatment rooted in racism. The death of Joyce Echaquan in September 2020 at the Joliette hospital illustrates how the Quebec healthcare system is not always safe for Indigenous community members. The coroner’s report concluded that systemic racism contributed to Joyce Echaquan’s death (25), despite the Quebec government’s continued refusal to acknowledge systemic racism (26). Beyond this tragedy, health policy failures also shape Indigenous people’s healthcare experiences. For example, the Régie de l’assurance maladie du Québec, the provincial public health insurance plan, has historically excluded certain Indigenous people living in Quebec from coverage, creating barriers to access and perpetuating inequities (27,28). Also, legislation such as Bill 96 perpetuates linguistic colonialism, further erasing Indigenous languages and restricting access to healthcare and legal services (27). These past and present experiences contribute to a particularly negative perception of the public healthcare system and the governments of Quebec and Canada (29).
In other words, the culture of skepticism toward dominant hegemonic structures can be associated with colonialism (29). Therefore, if the pandemic is recognized as a global phenomenon (by some), the interpretation of its consequences and the actions to be taken seem ‘imposed’ by the government. This does not imply that participants were unaware of this global phenomenon, but rather that, at their local level, the pandemic is intrinsically linked to the history between the government and Indigenous peoples. In this sense, participants’ preference for family, Elders, and community networks can be read as a form of resilience and agency rooted in historical experience with institutional mistrust.
In this context, social media, especially Facebook, played a key role by centralizing diverse information sources and allowing multiple types of information to coexist on a single platform. As shown in another study, this combination could explain that Facebook is the participants’ preferred social media as far as information is concerned (17). However, since August 2023, Meta has removed news from its platforms, raising questions about the diversity of information currently coexisting on social media.
This preference for using Facebook to obtain information is noteworthy in a context where social media is often associated with misinformation, and where misinformation related to public health issues is particularly prevalent on these platforms (30). However, the impact of exposure to misinformation on behaviors and attitudes remains uncertain, as encountering misinformation does not necessarily lead to its adoption.
When seeking information, participants aimed to solve specific problems and questions that directly affected their daily lives. In this context, the evaluation of the information consulted is based on its situational relevance (11). The impact of the COVID-19 pandemic on the sources consulted by the participants appears to be relatively minimal, except for a reduction in consultation frequency for some, which can be attributed to anxiety generated by information overload. Participants’ reliance on social media to access information from peers and community members reflects both pragmatic problem-solving and a broader skepticism rooted in historical experiences of institutional neglect and exclusion. This brings us to an essential dimension of their informational practices: how information was evaluated, and how trust was built and negotiated throughout the pandemic.
Information evaluation and trust
Participants prioritized information based on the sender’s proximity and trustworthiness, valuing direct conversations, personal testimonies, and the ability to witness events firsthand. Social media such as Facebook and TikTok contribute to the sharing of this kind of information. Information circulating on social media is considered less censored than that conveyed by television, a medium associated with government and official information. This observation seems to echo the importance, among many Canadian Indigenous Nations, of experiential knowledge and community networks in disseminating health-related information (11). The inclination of several participants to consult experiences on social media also seems to reflect the ‘building of horizontal relationships of trust’, facilitated by the internet (31). In other words, the proximity of the sender partly explains the preference for social media as an information source. The threat of misinformation on social media thus appears diminished, as participants primarily use it to connect and learn from people or organizations they trust, both online and offline.
Community organizations played a key role in disseminating credible and reliable information, as participants felt they could trust them. Far from being mere intermediaries of government messages, these organizations, Friendship Centers, Elders, and peer networks, were recognized as knowledge authorities in their own right. Participants emphasized not only their competence and trustworthiness but also the cultural relevance they brought, which reinforced resilience, adaptability, and agency. Friendship Center employees, for instance, were central to participants’ acceptance of vaccination. While much of the information came from government sources, employees and Elders adapted it to local realities, ensuring it resonated with community needs (32).
Government information wasn’t automatically trustworthy. Many participants relied on their own judgment, family, Elders, and community organizations rather than government sources. This stance was part of a broader history shaping Indigenous peoples’ relationships with public institutions. Mistrust thus reflects both lived experience and the enduring impacts of colonialism, not only to the specific dynamics of the pandemic. At the same time, participants’ skepticism also resonates with broader patterns of declining trust in institutional authorities in contemporary ‘information societies’ (11,33). In summary, trust was negotiated through the lens of history, context, and relationships, rather than taken for granted. Furthermore, the coherence of connections across these various levels will also play a crucial role.
Conclusion
In the context of the COVID-19 pandemic and infodemic, mistrust of the government has become entangled with feelings of uncertainty exacerbated by media saturation and the circulation of contradictory information. Our study is not without limitations. First, this is exploratory work conducted in specific urban regions of Quebec with a small number of participants. It should therefore be read as shedding light on particular experiences rather than representing the entire urban Indigenous population. Many of the interviewees find themselves in a highly precarious situation, due to health or economic factors, which further shapes the lens through which results should be interpreted. While the study included participants from several Nations (Atikamekw, Cree, Inuit, Métis, Ojibwe, and Innu), it did not include participants from other Nations living in Quebec, such as Abenaki, Algonquin, or Mi’kmaq. We acknowledge this absence as a limitation of the study design, which was not intended to cover all Nations, but rather to conduct exploratory work with a limited group of participants. Second, the study was grounded in Western sociological frameworks, such as the sociology of uses, and concepts like informational reflexivity. These constructs, while analytically useful, present limitations in fully capturing Indigenous knowledge systems. The absence of explicit engagement with Indigenous epistemologies constitutes a significant limitation. Third, while our analysis sheds light on how participants within particular urban Indigenous populations access and use health information through digital platforms such as Facebook, it does not address the broader structural issue of Indigenous-controlled digital infrastructures. Reliance on corporate platforms inevitably shapes health information practices, but this dimension extends beyond the scope of our exploratory study and warrants further research. Finally, the social desirability bias among participants, inherent to qualitative approaches, should also be taken into consideration. Also, while compensating research participants is generally accepted in qualitative research to recognize the time and energy participants dedicate to answering questions, this practice could potentially reinforce social desirability biases or cause information biases. That being said, this issue was minimized by conducting interviews with professionals in qualitative research who possess extensive experience with Indigenous communities. Additionally, before the interview, participants were informed that there were no right or wrong answers and that their statements would remain confidential, which helped minimize bias.
To effectively disseminate health-related messages, it is essential that public health authorities collaborate with Indigenous communities.
Findings from the exploratory phase informed co-construction workshops that led to the development of an open-access tool to support health message dissemination in Indigenous communities and other partner organizations (19). This process illustrates the value of culturally aware, collaborative approaches that strengthen ties between community organizations and public health authorities (34). The importance of considering the perceptions of Indigenous community members regarding health and well-being, rather than viewing these concepts strictly from a Western perspective, is crucial, as Indigenous and Western knowledge systems are rooted in distinct theoretical and epistemological frameworks (4,14,33). Maintaining reflexivity on the knowledge systems we rely on, and considering Indigenous values and culture, can also contribute to a decolonization movement in research (35). Looking ahead, we explicitly commit to ensuring Indigenous governance and leadership in all future phases of this research. This commitment is in direct alignment with Canadian ethical frameworks, including the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (36), especially Chapter 9: Research Involving the First Nations, Inuit, and Métis Peoples of Canada, which will guide the next stages of our work.
Footnotes
Acknowledgements
We are immensely grateful for the collaborative efforts of the Native Friendship Centre of Lanaudière, the Native Friendship Centre of Montreal, and the Southern Quebec Inuit Association throughout this entire project, as well as all the participants who generously dedicated their time to our project. Additionally, we would like to thank Alexandre Tremblay and Origene Djun Danie for their valuable contributions in data collection and analysis.
Ethic
The research project has been approved by the CIUSSS du Centre-Sud-de-l’Île-de-Montréal ethical board (Project 2022-829).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Canadian Institutes of Health Research (Award number: MM1: 174884). The development of the research project was supported by the Reseau de recherche en santé des populations du Québec (Quebec Population Health Research Network).