
Abstract
While the COVID-19 pandemic amplified the need for accurate and actionable health information, uncertainty and the proliferation of misinformation have contributed to significant mistrust in public health messages, especially among marginalized communities. Community health organizations can play an important role in creating trust and providing targeted health information to vulnerable groups. This qualitative study, which is focused on community health organizations supporting vulnerable populations in South Africa and Zambia, finds that during the pandemic, community health organizations expanded their roles and leveraged their established access and trust to support the communities they serve with health education and services. However, the reliance on external support limits the organizations’ ability to respond in an effective and efficient manner during health crises.
Introduction
The COVID-19 pandemic strained already struggling public health systems worldwide (1–5). Ensuring that vulnerable communities have access to accurate and actionable health education and information is critical for equitable public health responses and for reducing the spread of disease globally (6–8). Although governments often serve as a primary source of public health information, marginalized populations are less likely to receive information from government channels (9). Furthermore, mistrust in government and public health systems, particularly among marginalized groups, can erode the effectiveness of public health campaigns (10–13). During the pandemic, mistrust has grown due to the spread of misinformation, rumors, and global health conspiracy theories (14–18). In South Africa and Zambia, evidence suggests substantial mistrust in government sources. This has been observed in relation to information circulating about the COVID-19 crisis (10,11), making it important to understand the challenges faced.
Community health organizations can play an essential role in providing reliable information that reaches vulnerable populations and marginalized communities better, including the following: those with limited access to healthcare and safe housing and transportation; those experiencing racism, discrimination, and violence; those suffering from economic instability, food insecurity, environmental pollution, and health complications due to comorbidities and other noncommunicable diseases (NCDs); those with limited literacy; and linguistic minorities (19–21). For this study, community health organizations are defined as organizations that operate in local communities and are staffed primarily by local people, with the majority of the governing body and staff consisting of residents. Their primary operating offices are in the same country and region, and their areas of concern and program solutions focus on local issues. They are also actively engaged in providing health services and advocacy, and/or the delivery of health education and information services at the community level.
Historical evidence has shown that given their deep contextual understanding, community health organizations operating in local communities have been particularly successful in developing well-received targeted health messages. By providing targeted health messages and support, these community health organizations can support people to increase control over their health and improve it. For example, during the recent Ebola outbreak, international nongovernmental organizations, intergovernmental organizations, regional and national governments, and higher education institutions partnered directly with community health organizations and leveraged community health worker (CHW) programs, resulting in valuable support for mitigation efforts (22–25). Other illustrative examples include the immense importance of community organizations’ role in health promotion by supporting patients during the HIV/AIDS epidemic (12,26–28) and their enduring efforts to eradicate polio among the hardest-to-reach communities (29,30).
Emerging evidence during the COVID-19 pandemic reveals the importance of worldwide community-level responses (31). Community health organizations have played a vital role in filling the gap in burdened public health systems to meet the health education and information needs of the most vulnerable groups in the community. To address the swift and widespread impact of the COVID-19 pandemic, these organizations were driven to expand their role quickly to provide novel and evolving health information to constituents while operating at a limited capacity.
Here, we examine the experiences of community health organizations with regard to health promotion in their responses to the COVID-19 pandemic in South Africa and Zambia. The response to the pandemic by community health organizations has been critical in sub-Saharan Africa, given an already struggling public health infrastructure, a shortage of healthcare workers, barriers to accessing health facilities, and significant mistrust of government-provided health information, leaving marginalized communities in South Africa and Zambia at exceptionally high risk for inadequate healthcare during the pandemic (32,33). While both the governments and international health organizations operating in South Africa and Zambia have relied on community health organizations and workers to provide primary and emergency health services in the past, they have provided little support. These resource limitations may restrain community health organizations’ ability to support communities’ health needs (19,21,34). Given the reliance on community health organizations, the history of limited resources, and the nature of the crisis, it is critical to understand the role of these organizations in promoting public health in South Africa and Zambia.
Our study uses qualitative interviews and thematic analysis to investigate the strategies, challenges, and needs of community health organizations involved in public COVID-19 education to understand their role in public health crises in relation to communicating health information and providing services to support their communities’ improved well-being. This study seeks to understand how community health organizations in South Africa and Zambia responded to the pandemic and how limited resource support may have hindered their ability to address the health needs of marginalized communities. This study can illuminate the potential of community health organizations to fill gaps in mainstream public health education and bring about meaningful local-level responses during future public health emergencies.
Health promotion efforts by community health organizations
Community health organizations are uniquely positioned to understand how public health crises, such as the pandemic, have an impact on their community (35). Community health organizations understand local perspectives on public health issues, such as COVID-19, as well as susceptibility, threats, and barriers in relation to vulnerable groups, for example, constituents who may be immunosuppressed from HIV/AIDS or have comorbidities from NCDs. By integrating their knowledge of local perspectives with their understanding of the needs of their local patients, these organizations can modify communication strategies accordingly by ensuring that the most relevant information reaches the populations that need it, and also address localized myths and misinformation (35). All the specialized knowledge that community health organizations have amassed about local needs, challenges, and lived experiences can help them adapt and craft simplified messages about communicable diseases and pandemics in ways most likely to be trusted and adopted by local communities. These tailored messages help reinforce the partnership between community members and health organizations by empowering people and communities to make healthy decisions that affect their lives.
Limitations to effectiveness in health education
There are limitations to the effectiveness of the community health organization model. Previous research has found that small community health organizations face significant structural and resource challenges when collecting and sharing information, knowledge, and resources with local communities (36). The reliance of community health organizations on largely voluntary workforces is one obstacle to consistency (36) due to the loss of paid staff during times when financial resources are reduced (19). Another is having to adapt their programs because of shifting donor interests, government priorities, or funding opportunities (37). With changing members of an organization, shifting identities, or inconsistent programs, the reliability, knowledge, and trust that communities invest in community health organizations can be broken. Additionally, low compensation levels among CHWs due to a heavy reliance on limited public or donor funding can cause resentment that may translate into distrust in the organization among beneficiaries in the community (37,38). This situation may occur when workers cannot provide care or information, which has an effect on their credibility, or through their attitudes, discussions, or experiences (21).
The embedded nature of community health organizations that builds trust in the first place can also cause trust issues. For example, living in the same community can test the workforce’s ability to maintain confidentiality, which can strain trust (21). Social stigmas and local beliefs may also interfere with trust or access to health services (21). The potential limitations of the model illustrate the need for a greater understanding of the role that community health organizations play in health promotion during public health crises.
Methods
Sample population
A total of 18 community health organizations in South Africa and Zambia were included in the study. Criteria for inclusion in the study were the following: (a) active engagement in health services, advocacy, and/or delivery of health education and information services at the community level before the pandemic; and (b) involvement in health education efforts in response to COVID-19. While none of the community health organizations operated or were headquartered outside of sub-Saharan Africa, there was some variation in their areas of focus, operating size, target beneficiaries, and geographic focus. Of the 18 organizations, 12 operated nationally, and 6 operated strictly as local-level organizations. Of the 18 organizations, 12 were located in South Africa and 6 in Zambia, covering both rural and urban areas. Many of the organizations had long histories in the communities they served. The median time the community health organizations had been in existence was 13 years. The median size of the paid professional staff was 15 workers. Before the pandemic, many of these organizations also relied on large numbers of volunteers, up to as many as 500, and one organization relied solely on voluntary staff. However, the pandemic and related lockdowns caused most community health organizations to restrict or temporarily end their volunteer programs. Table 1 shows the number of organizations by characteristics.
Community health organization characteristics.
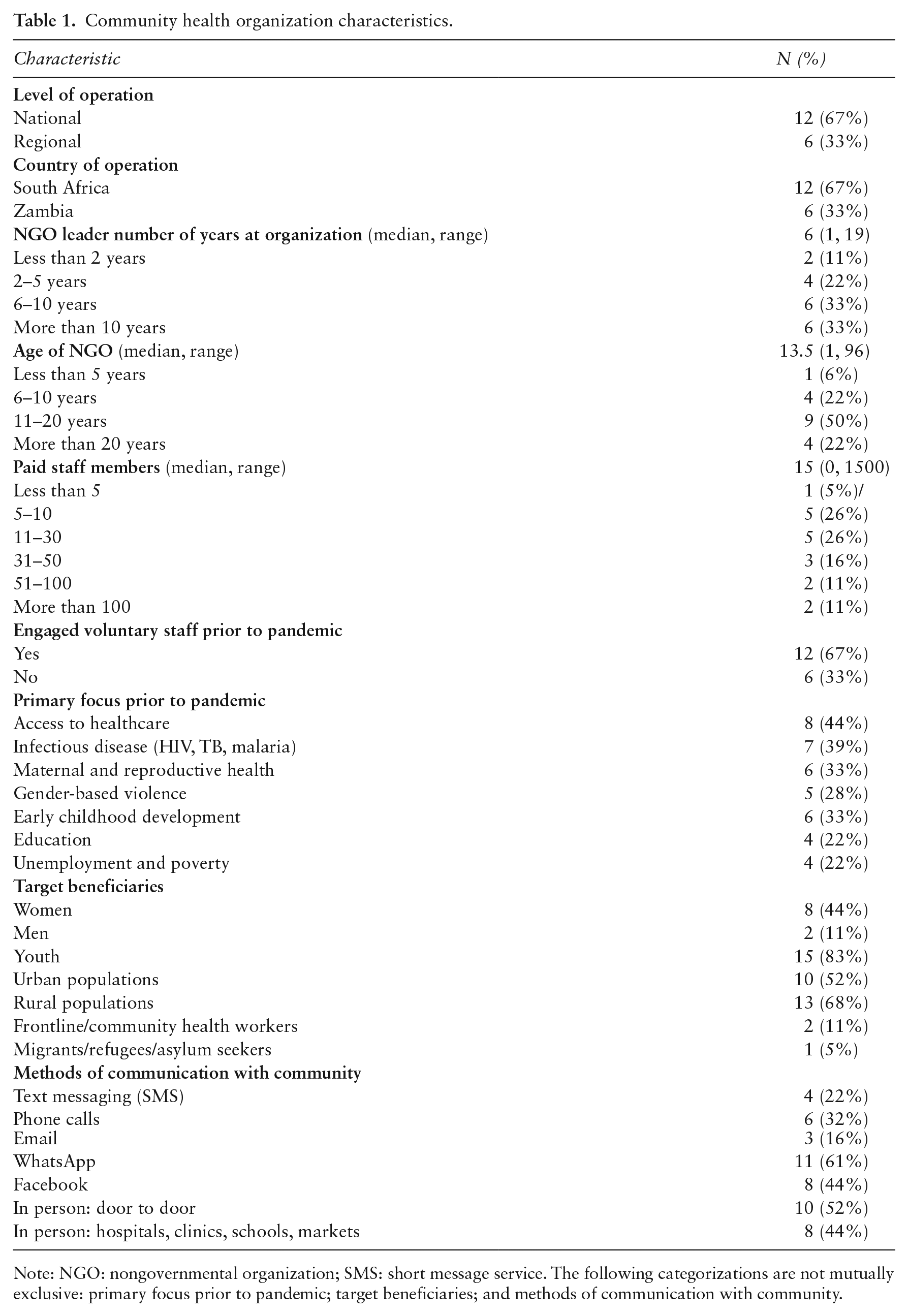
Note: NGO: nongovernmental organization; SMS: short message service. The following categorizations are not mutually exclusive: primary focus prior to pandemic; target beneficiaries; and methods of communication with community.
The community health organizations were identified through their previous collaboration in shared global health networks and expanded via a snowball technique and internet search. In total, 25 community health organizations were identified, of which 18 consented to participate in the study. All participating organizations except two are entirely nongovernmental. The remaining two were hybrid organizations. To recruit organizations, we contacted the director (highest-ranking staff member) to request permission to include the organization in the study. We then recruited the director or a senior-level staff member nominated by the director to participate in the semi-structured interviews. Because of pandemic distancing restrictions, we recruited and communicated with participants virtually via email, phone, or WhatsApp. Participants held leadership roles in their respective organizations at the time of the interview and had been with their organizations for a median of six years.
Data collection
The data for this study were collected through semi-structured one-on-one in-depth interviews (IDIs) with participants over the Zoom video conferencing platform. Interviews were conducted by a South African member of the research team in Cape Town, South Africa. To promote open and honest reflection, both interviewer and participants were in private spaces where personal responses would not be heard. The interviewer was trained in community-based research methods and health promotion.
The interviewer used a semi-structured four-part interview protocol, which was co-designed by researchers from South Africa and the United States. The 25-question protocol focused on background information, local community knowledge, information dissemination, pandemic responses and impacts, and information and education experiences. In the first two sections, the interviewer asked questions about the participant and the organization’s background as a health provider in the community. The sections were designed to understand the community health organizations’ knowledge about their local communities and how that knowledge has an impact on the information and education they provide during health crises. The third section asked about the organization’s response to the pandemic. The interview protocol concluded with a section focusing on the impact of the pandemic on communities and how communities received the information and education the organizations shared.
Data analysis
Interviews were transcribed verbatim via Zoom’s transcription program and reviewed by the research team for transcription errors. Once transcribed, inductive analysis and constant comparative methods were used to code data systematically and identify key themes emerging from them through the thematic analysis process. First, all of the authors gained familiarity with the data by reviewing the transcripts. This process generated initial codes related to the research questions. Next, two separate authors independently coded every interview to maximize internal validity and coding consistency using Dedoose qualitative software by applying a priori codes related to the primary research questions. Two authors organized codes into potential themes that emerged through the coding process and presented them to the research team. The research team met multiple times to confer, and calibrate coding interpretation. During these sessions, the research team sought consensus on refining and recalibrating coding schemes and themes. Finally, agreement was reached, the themes were revised, and the final codes were selected. Each transcript was then analyzed for a second time by two independent authors to ensure validity and consistency in applying the codes. The researchers then met, and based on this analysis reached consensus on the final themes.
Results
Three primary themes emerged from the analysis. First, as the pandemic spread, the community health organizations adjusted their services to respond to the pandemic’s new challenges, which they did by taking on new community roles. Second, the community health organizations provided responsive COVID-19 health education and information programs. Third, they supported healthy communities by addressing challenges exacerbated by the pandemic.
In response to the pandemic, community health organizations frequently adjusted their services and filled new roles. They filled new partner roles, often liaising between government ministries of health or large international organizations and their local populations. In these roles, they supported local hospitals and government pandemic efforts. Here, they often advocated for their client communities. For example, one organization provided personal protective equipment to health workers on behalf of the government, while another sent staff to help with government screening and testing programs. The community health organizations also partnered with each other, providing their unique expertise to serve the same communities better. When discussing how their organization partners with other local organizations, one leader said: Our two organizations decided to figure out how we can bridge the gap in terms of information . . . We are very focused on rural [areas], and there’s a gap in information for rural communities . . . We ended up identifying community radio stations because we thought that would be a viable platform during COVID . . . We developed a whole list of topics or talking points. Then we identified experts or informed persons, and we connected those people with community radio stations . . . As an organization, we work well with other organizations and are good at linking and connecting (IDI 8).
The community health organizations also adjusted their services by identifying community-specific concerns, which guided their responses to the pandemic and their work. One community health organization leader described the process of identifying community needs as follows: We had an obligation to better understand the communities within our learning site, and to also not make rash statements based on assumption, but to actually understand what is going on, on the ground. And then we tailored . . . what we did after we did the survey (IDI 8).
They then used the information they had gathered to tailor their programs to provide pertinent COVID-19-related health services, information, and education quickly.
The second theme that emerged was that the community health organizations provided responsive COVID-19 health education and information programs. Community health organizations use both social media and traditional forms of media to reach their communities with these programs. Given the constraints of the lockdowns and social distancing, most organizations used some form of social media to communicate with the public about COVID-19. WhatsApp and Facebook were the most commonly cited platforms and were deemed particularly effective at reaching younger populations. However, the organization leaders emphasized that many groups cannot be reached through the internet or social media, and radio was a popular platform for targeting rural populations. The community health organization leaders expressed that when they shifted to remote communications, they had an increased need for technical support, both in terms of greater technology access (e.g., a need for smartphones and tablet devices to communicate better with constituents) and support for using technology for both their own staff and the communities that they serve. One leader said: I think the shift to digital brings a lot of troubleshooting in terms of making sure you’re using the right tools, making sure you do it in a way that’s responsible . . . [so] that you’re not excluding a whole range of the population because they’re not online, as well as making sure that your use of digital space is a responsible one (IDI 1).
While there were substantial efforts to provide health information and education using remote methods, many community health organizations still utilized their physical presence in the community, especially to communicate with groups that were more difficult to reach. Posters and pamphlets were crucial materials used to deliver health information. Several community health organizations trained employees and CHWs to conduct home visits offering COVID-19 screening and education. An organization that visited homes found that many families had not heard of COVID-19. When [we] were doing home outreach, most people were actually surprised. They didn’t even know [about COVID-19]. They hadn’t even heard because they don’t have cell phones, they don’t have WhatsApp . . . most people needed to hear by word of mouth [which is] why we needed pamphlets . . . in both languages, English and Xhosa, so that people can easily understand (IDI 3).
However, there were limitations to and challenges for the community health organizations’ ability to provide responsive COVID-19 programs. The community health organization leaders stated that staff members felt overwhelmed and wanted relevant, solution-driven information. They expressed a need for guidance to decipher and distill what one leader described as ‘information overload’ (IDI 14) and an ‘overwhelming influx of COVID information’, subsequently noting a desire for ‘just [the] relevant information appropriate to you and to your constituency’ (IDI 8). One leader said: [The organization program manager] is basically drowning in information . . . [They] are really struggling because there’s just too much . . . finding relevant facts and information that’s also . . . solution driven. . . . with our expertise, we can bring [this material] to a plan and work and beyond. That would be useful (IDI 1).
The leaders stressed that many recommendations and protocols they received regarding COVID-19 from government ministries of health and international institutions did not reflect their communities’ challenges. For example, small living quarters and large families have an impact on the ability to comply with social distancing measures at home. The reliance on public transportation for essential tasks, like purchasing food or going to and from work, also has an impact on the ability to meet social distancing recommendations. Lack of access to clean water or masks hinders compliance with those recommendations. These challenges with regard to the recommendations frustrated the community members and health organizations. While the leaders were concerned about how this frustration would have an impact on compliance and trust in health information, they also desired support in making health information actionable.
Finally, community health organizations promoted healthy communities by addressing challenges exacerbated by the pandemic. Many of these organizations served vulnerable populations who faced a variety of other challenges, including food and housing insecurity, gang violence, HIV/AIDS, and NCDs, and struggled to overcome their distrust in the government’s public health messages and the more extensive health system, and found it challenging to accept pandemic protocols and messaging. One leader stated: ‘When it comes to the much bigger structures, people don’t have much trust in the health systems at all’ (IDI 16). Mistrust in information among disenfranchised youth, rural communities, and displaced persons created particular barriers for the community health organizations that they had to attempt to overcome.
Some communities viewed the pandemic as not a threat, or no more of a significant threat than their other concerns, as ‘people have faced so much adversity that this is just one more thing’ (IDI 5). This experience fed into a belief for some that COVID-19 was, as one leader stated, just another challenge: ‘A lot of the people’s mindsets currently is that, “you know what, we’ve survived AIDS, we’ve survived TB so that we will survive COVID as well”’ (IDI 16). Leaders expressed the importance of delivering health information and education that addresses the adverse impacts of the traumas and experiences that these communities have already experienced. The community health leaders also focused on supporting health issues ‘amplified by the crisis’ (IDI 1) and developing programs to address the pandemic’s economic impact on their communities, which resulted in increased unemployment, food insecurity, and poverty. In discussing a food service program her organization started, one leader said: It’s easy to tell everyone to go and stay in their own homes, but for the kids on the streets . . . they rely on donations or begging to get food . . . there are some families as well that have had nothing . . . those are some of the families that we are considering for this feeding program (IDI 6).
Another community health organization integrated its COVID-19 messages with additional resources in that it designated CHWs to visit families to discuss COVID-19 and identify those who could use more resources, such as food baskets.
Discussion and conclusion
Our study examines community health organizations’ responses to the COVID-19 pandemic. While this pandemic is unique in the breadth and severity of its impact globally, the responses exhibited by the organizations in this study reflect the role that community health organizations play in local communities to help protect and meet the needs of the most vulnerable members of society during a public health crisis. Community health organizations are a critical component of health promotion. They are essential in delivering targeted health information to high-risk groups otherwise unreached by mainstream health education channels and empowering them to make healthy choices.
We found that community health organizations are uniquely positioned to deliver effective health education given the following: their familiarity with local customs and norms; their awareness of local resource constraints; their ability to identify locally prevalent myths and misinformation; their knowledge of the needs facing specific risk groups (e.g., women, children, migrants, people living with HIV/NCDs, etc.); and their access to local translators who can assist with the translation of health information. This understanding of multiple aspects of local communities is built on their pre-existing relationships of trust within the communities, which supports these organizations to adapt health messages as needed. Adapting the health messages and providing relevant and necessary services bolsters those trusted relationships.
Community health organizations can leverage established communication channels, including traditional platforms, social media, and other technology, as well as in-person methods of communication. They can also utilize their networks to identify and leverage locally trusted sources of information, such as local religious and traditional leaders, to assist with information dissemination. These methods of communication further build and validate the trust between community members and the organizations. This trust then serves as an endorsement for the legitimacy of the health information provided by community health organizations.
While the potential for these organizations to reach the most vulnerable members of society exists, our findings reflect the challenges community health organizations face in times of crisis. The loss of funding and lack of technology and health expertise to navigate an effective response render these organizations less effective, which could jeopardize the community’s trust. Given the potential of community health organizations to serve the most vulnerable, this study underscores the formidable obstacles these organizations encountered. By spotlighting the challenges due to funding shortages, technological limitations, and a lack of health expertise, we can illuminate the complexities inherent in responding to public health crises. Furthermore, these insights can allow stakeholders to engage in collaborative problem-solving, innovative thinking, and the formulation of strategies that will potentially address these challenges.
The study illustrates the importance of contextual and actionable educational materials to bridge knowledge–behavior gaps. It suggests that support from governments, international organizations, and partners could enhance community health organizations’ educational efforts and extend their reach through easily adaptable content and assistance with technological and safety challenges. Given their role in providing targeted messages to their communities, community health organizations could benefit from educational resources that can be easily modified for various contexts. Since creating health messages to match local language and culture is highly labor intensive, easily modifiable content would allow organizations to make more efficient use of their staff, extending the reach of their health messaging. Community health organizations would also benefit from increased support for navigating technological and safety challenges in pandemic settings. Developing health education, resources, and information that engages and responds to communities requires time, empathy, and resources, which state responses may lack during health crises (31). While locally embedded organizations can support communities by their response to the pandemic, which involves engaging community members and successfully building confidence and trust in health messages and adherence to public health protocols, ultimately, they need sustainable funding sources to continue operating and set long-term goals for their programs, given these additional resource needs.
Our study contributes to a deeper understanding of the role of community health organizations in providing needed support and customized health education for vulnerable communities during the COVID-19 public health crisis. As we face future health crises, it will be critical for community health organizations to receive support to deliver health education and services to empower hard-to-reach groups effectively. Further research is needed to obtain a better understanding of the components of successful health interventions by community health organizations and their emerging needs, as well as those of communities.
Supplemental Material
sj-docx-1-ped-10.1177_17579759231205854 – Supplemental material for Exploring the role of community health organizations in promoting public health during a health crisis: a qualitative study of COVID-19 responses in South Africa and Zambia
Supplemental material, sj-docx-1-ped-10.1177_17579759231205854 for Exploring the role of community health organizations in promoting public health during a health crisis: a qualitative study of COVID-19 responses in South Africa and Zambia by Jamie Sewan Johnston, Kelly Zhang Aluri, Nophiwe Job, Kira-Leigh Kuhnert, Charles Prober, Victoria Ward and Nadine Ann Skinner in Global Health Promotion
Footnotes
Acknowledgements
We thank the organizations that agreed to participate in the study and are grateful to the digital medic team from the Stanford Center for Health Education and the faculty advisory board for providing critical feedback throughout the development and implementation of the study.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Stanford Center for Health Education.
Disclaimer
The findings and conclusions expressed in this article are those of the authors.
Ethical approval and participant consent
Ethical approval for this study was obtained from the Institutional Review Board of Stanford University School of Medicine (Protocol ID 57373). Verbal informed consent was obtained from all participants before interviewing them.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.