
Abstract
Consistent and proper condom use offers a safer, economically cheap and practically effective means of preventing HIV infection. Using the 2014 Ghana Demographic and Health Survey with a sample of 2779 sexually active youth (males = 682 and females = 2,097) in the age range 15–24, this study explored the prevalence of, and factors associated with consistent condom use among sexually active young adults in Ghana. Multivariate logistic regression was used to analyse the data. Our results showed that approximately 11% of the respondents reported consistent condom use in their previous sexual activity. Females were more likely than males to have used a condom consistently. The logistic regression results showed that females who had tested for HIV were less likely to use a condom consistently. However, those who have obtained family planning information from print media and those from the northern part of Ghana were more likely to practise consistent condom use. Furthermore, males who professed the Traditional African religion were less likely to use a condom consistently. In contrast, males in the rich wealth category were more likely to use a condom consistently. These findings underscore the need for behavioural change campaigns targeting young adults, particularly those who are sexually active, to encourage consistent condom use. These interventions should target young adults with less family planning knowledge, those who know their HIV status and those who profess the Traditional African religion.
Introduction
Globally, young adults account for nearly half of all new HIV infections (1), and unsafe sex is one of the leading causes of disease due to the transmission of HIV/AIDS (1). HIV transmission is primarily heterosexual in sub-Saharan Africa (SSA), and Ghana is no exception (1,2). Indicatively, consistent condom use could be a safe, economically cheap and effective method of preventing sexually transmitted infections (STIs), including HIV and AIDS (1,3,4). However, a condom is only effective when used correctly and consistently (4,5).
Apart from the prevention of HIV/AIDS, consistent condom use can prevent other STIs and also unintended pregnancy, which is another reproductive health problem confronting adolescents and young adults. For example, in Ghana, about 12% of adolescent girls are either pregnant or mothers already, with one in every 10 births occurring among young people (6). This phenomenon makes condom use one of the reliable ways young adults can protect themselves from unintended pregnancies and STIs, besides having sex with an uninfected person (1,7). Previous studies on condom use among young adults focused on identifying and explaining the determinants of inconsistent condom use and are well documented (8,9). Some factors attributed to the inconsistent use of a condom include low perceived sexual satisfaction derived from condom use, low personal STI risk, condom fatigue, having a steady sexual partner and low condom self-efficacy (8,9). Some studies propose the need for behavioural campaigns to encourage self-efficacy in relation to condom use to improve take-up (8,10).
Although consistent use of a condom has an important role to play in providing safer sexual and reproductive health for young people, only a few studies have investigated the determinants of consistent use of condoms among young adults (7,11,12), whereas studies on the determinants of inconsistent condom use in general abound. Most studies on consistent condom use focus on sex workers, and observed that consistent condom use effectively prevented the transmission of HIV/AIDS (13). In a study on HIV risk perception and consistency in condom use among young adults in urban Cape Town, South Africa, it was observed that perceived risk of HIV/AIDS infection was not a significant determinant of consistent condom use, and consistency in condom use declined with increasing age (12). However, the same study indicated that the perceived risk of HIV/AIDS was associated with increased condom use (12). Studies on determinants of consistent condom use are important for public health in Ghana, given the fact that, increasingly, young adults are engaging in sexual activities at an early age and marrying later. The median age at first sex among people in the age range 25–29 in Ghana is 18.4 years, and 11% of women in the age range 25–49 had had their first sex by age 15 (6). The gap between age at first sexual intercourse and age at marriage is widening, with more people being sexually active before marriage than in the past (14,15). Evidence from Ghana suggests that being female, of a younger age, of low socio-economic status and living in a rural area are independently associated with early sex among sexually active young people (16). Further exploration of these factors indicated that young people from rich households residing in urban areas are less likely to initiate early debut. However, an interactive effect showed that female youth residing in urban areas from rich households were more likely to initiate early debut (17). The extent to which socio-demographic characteristics influence consistent condom use among these sexually active young people remains unexplored within the Ghanaian context.
To help understand how different multilayered factors interact in creating pathways to young people’s sexual activity, including consistent condom use, various theoretical models have been formulated. In this study, we used the information–motivation behavioural skills model (18) and Campbell’s community characteristic (19) as frameworks to guide the study. The information–motivation behavioural skills model (18) indicates that individuals will engage in self-protective behaviours, such as consistent condom use, when they know that such behaviours reduce the risk of infection, are motivated to engage in the behaviours and have the requisite skills and self-efficacy to do so. Campbell’s community characteristic framework (19) also focuses on several community chara-cteristics associated with reduced vulnerability to HIV infection such as condom use. These include availability of information and resources related to HIV prevention, awareness of socio-cultural conditions that predispose youth to risky behaviour, the community commitment to addressing threats posed by HIV and the presence of social networks that support behavioural changes among youth. Thus, exploring adolescents’ consistent condom use requires an in-depth examination of factors both at and beyond socio-demographic, individual and family levels to encompass a focus on community systems as emphasised by the Ghana AIDS Commission’s five-year strategic plan. Using the 2014 Ghana Demographic Health Survey (GDHS), this study’s aim is to determine the socio-demographic factors associated with consistent condom use among sexually active young people in Ghana. The two main objectives of the study are as follows: (a) to determine the prevalence of consistent condom use among young people in Ghana; and (b) to examine the socio-demographic factors asso-ciated with consistent condom use among sexually active young people in Ghana. Our findings could be critical in developing HIV prevention strategies that encourage consistent condom use among sexually active young adults.
Methods
Sampling procedure and participants
The 2014 GDHS was conducted using a stratified two-stage cluster design consisting of 427 clusters, 216 in urban areas and 211 in rural areas. The first stage was a random selection of clusters, followed by a systematic selection of households at the second stage (6). The survey successfully interviewed 11,835 households, yielding a response rate of 98.5%. Moreover, 9396 and 4388 eligible females and males participated in the survey, producing response rates of 97.3% and 95.2%, respectively. For the current study, sexually active youths in the age range 15–24 who responded to the consistent condom use questions were used as the basis for analysis. Thus, a sample size of 2779 (males = 682 and females = 2097) was used for the current study.
Procedure
Data for this study were obtained from the 2014 GDHS. The GDHS is a nationwide survey with a representative sample of women and men in the age ranges 15–49 and 15–59, respectively (N = 13,784). The Ghana Statistical Service (GSS), the Ghana Health Service (GHS) and the National Public Health Reference Laboratory of the GHS supervised the 2014 GDHS. Ethical approval for the study protocol was given by the GHS Ethical Review Committee in Accra, Ghana and the Institutional Review Board of ICF International. The survey asked households questions related to HIV testing. Besides these questions, individuals were asked to state their age at first sexual intercourse during the last 12 months. Moreover, socio-demographic key indicators such as age, sex, place of residence, region, religion, education level and ethnicity were also part of the questions in the questionnaires. Each household selected for the GDHS was eligible for interview with the household questionnaire. Data collection was carried out by the 25 field teams from early September to mid-December 2014. Senior staff members from the GSS and the GHS coordinated and monitored the fieldwork. Paper questionnaires were used to conduct the interviews. After the interviews, field editors entered the questionnaire data into laptops, using passwords to protect the files. Electronic data files were transferred to the central office every few days via the secured Internet File Streaming System. Fieldwork monitoring was carried out by staff from the GSS and the GHS, and two survey technical specialists from the Demo-graphic and Health Surveys Program. Data collection took approximately four months.
Measures
Outcome variable
The main outcome variable was derived from three questions answered by the survey participants. They were asked if they used a condom every time they had sex with their (a) third to most recent partner, (b) second to most recent partner and (c) most recent partner in the last 12 months. On each of these three occasions, the responses were ‘Yes’ and ‘No’. A composite variable was created from these three variables to derive the variable ‘consistent condom use’ for participants who consistently used a condom on at least one occasion. Thus, this variable was coded as follows: 0 = No and 1 = Yes. The binary nature of the outcome variable necessitates the use of a logistic or probit regression for consistent estimates. The choice between the two estimators is based purely on preference.
Explanatory variables
The explanatory variables used in this study included residence (urban and rural), gender (males and females), religion, employment status, level of education, regions, HIV test status, source of family planning information, ethnicity and household wealth. The GSS constructed a wealth index from a household’s ownership of selected assets, such as televisions and bicycles, materials used for housing construction and the type of water access and sanitation facilities. The index places individual households on a continuous scale of relative wealth. The GDHS, however, only provides a wealth quintile based on the wealth index. We further subcategorised the households into three wealth categories based on the reported wealth quintile: poor (quintiles 1 and 2), average (quintile 3) and rich (quintiles 4 and 5).
Statistical analyses
The estimation samples were analysed using STATA 16.0. We accounted for the survey design by using the weight and cluster variables in the data. Doing this improves the precision of our estimates and ensures external validity. Consequently, our findings are nationally representative. We apply a Chi-square test and multivariate logistic regression to examine the relationship between the selected explanatory variables and consistent condom use. As we found gender differences in consistent condom use among the participants, we stratified our analysis accordingly and conducted logistic regression for males and females differently. The logistic regression results are presented as odds ratios (ORs) with 95 % confidence intervals (CIs). Statistical significance was defined as a two-tailed p-value < 0.05 in all analyses.
Results
Demographic characteristics of the sample
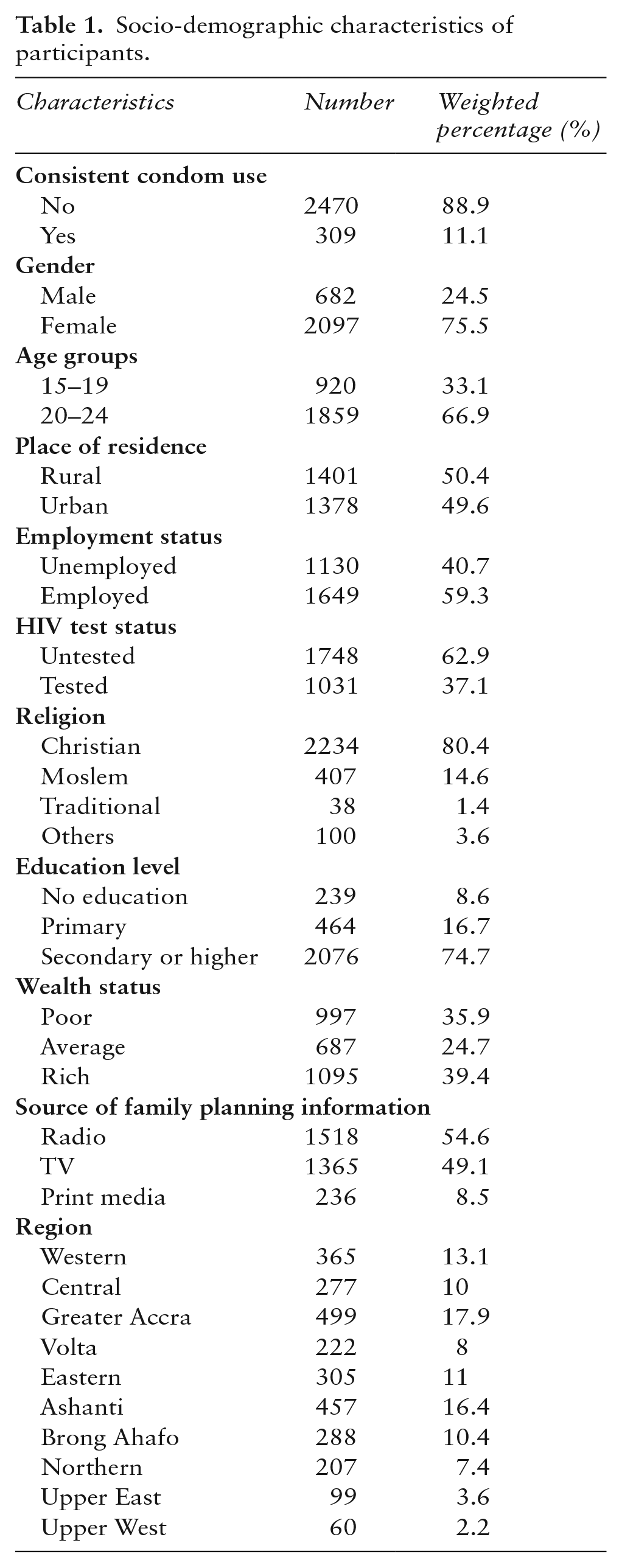
The socio-demographic characteristics of the participants are presented in Table 1. Females (75.5%) constitute the majority of the participants in the study, and over 66% of the participants were in the age range 20–24. Approximately half of the participants lived in rural settings (50.4%) and were employed (59.3%). Over a third of the participants (37.1%) had tested for HIV, and approximately three out of four participants (74.7%) had at least secondary education. Radio (54.6%) and television (49.1%) were the main sources of information for family planning, and over 80% of the participants self-identified themselves as Christians. About 39% of the participants considered themselves rich, while approximately 36% self-identified themselves as poor. Approximately 11% of the respondents reported consistent condom use in their previous sexual activity.
Socio-demographic characteristics of participants.
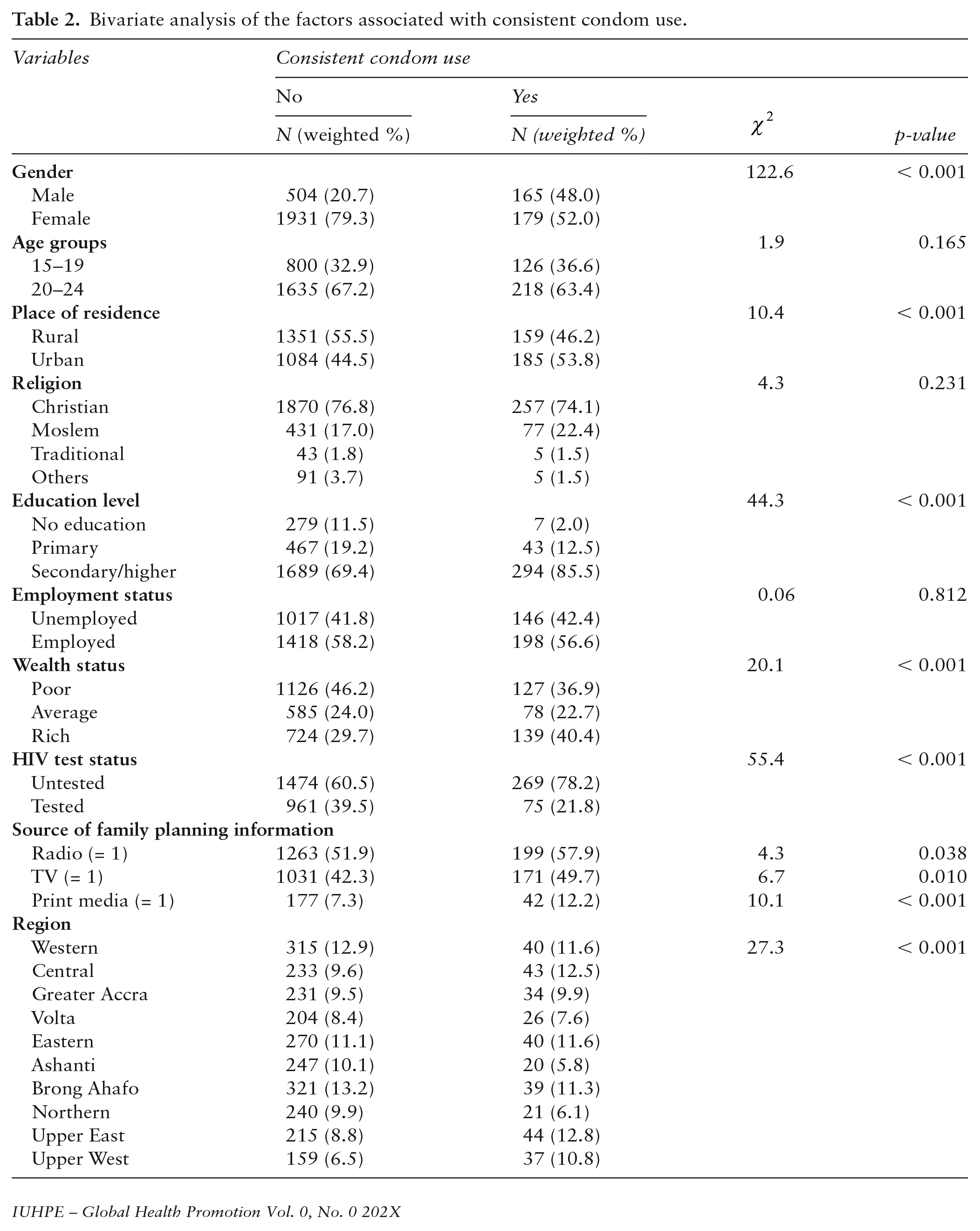
Bivariate analysis of consistent condom use with socio-demographic characteristics
Bivariate findings are presented in Table 2. Generally, the majority of the variables showed significant bivariate associations with consistent condom use. However, among the socio-demographic variables, gender (
Bivariate analysis of the factors associated with consistent condom use.
Multivariable analyses of consistent condom use with socio-demographic characteristics
The results of the logistic regression presented in Table 3 are stratified by gender. For females, those who had not tested for HIV had reduced odds of using a condom consistently (OR = 0.38, 95% CI: 0.25–0.59; p < 0.001). On the contrary, those who obtained family planning information through print media (OR = 3.01, 95% CI: 1.63–5.56; p < 0.001) and from the two northern regions, Upper East (OR = 2.80, 95% CI: 1.14–6.90; p < 0.05) and Upper West (OR = 3.38, 95% CI: 1.32–8.63; p < 0.05) were uniquely associated with increased odds of consistent condom use. For males, affiliation with the Traditional African religion (OR = 0.22, 95% CI: 0.05–0.89; p < 0.05) was associated with reduced odds of using a condom consistently, but the rich wealth category (OR = 2.47, 95% CI: 1.23–4.95; p < 0.05) was associated with increased odds of consistent condom use.
Multivariate logistic regression of the predictors of consistent condom use.
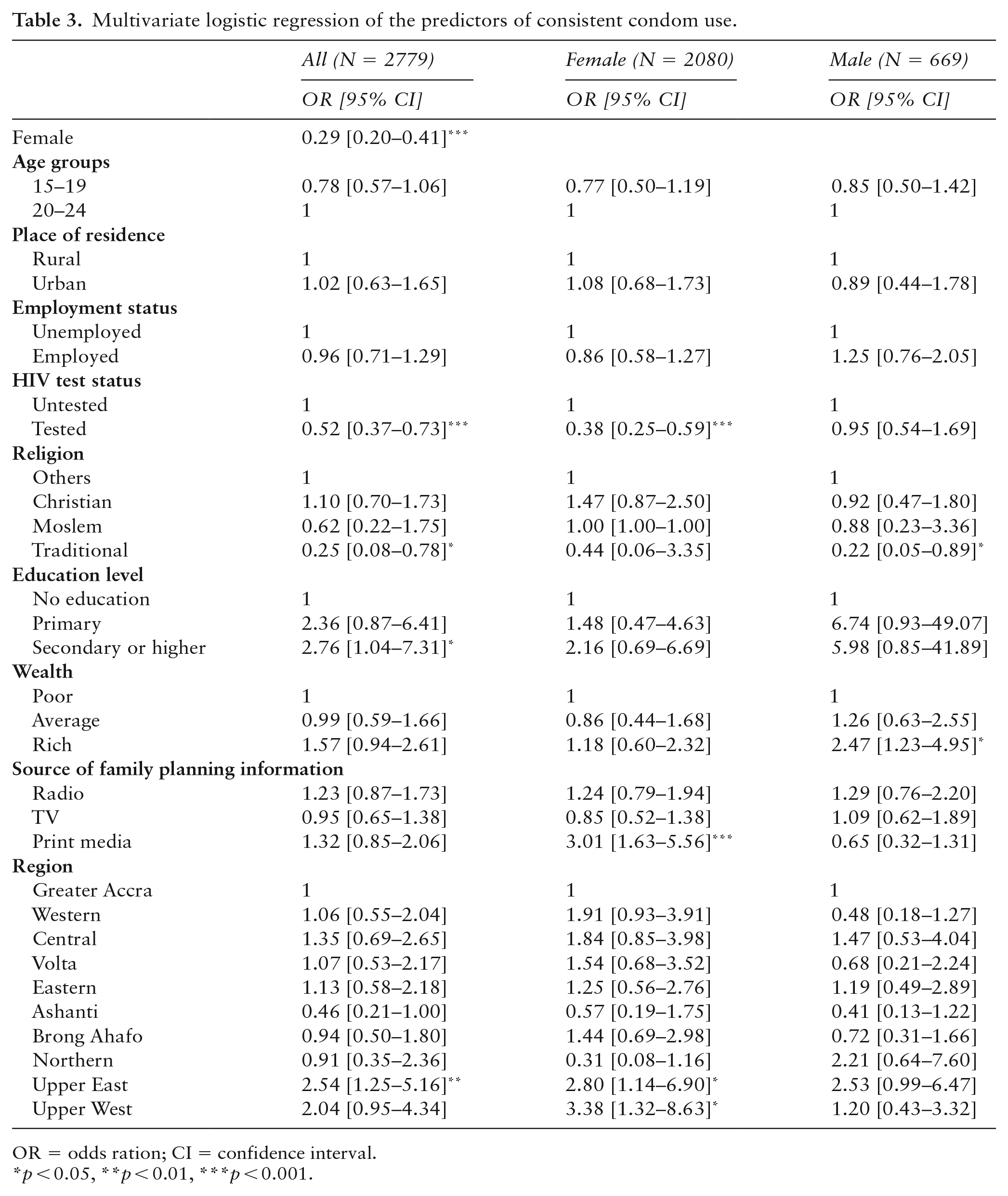
OR = odds ration; CI = confidence interval.
p < 0.05, **p < 0.01, ***p < 0.001.
Discussion
This study explored the prevalence and determinants of consistent condom use among sexually active young adults in Ghana. Our results showed that approximately 11% of the respondents reported consistent condom use in their previous sexual activity. Among the youth that were sexually active, females were more likely than males to have used a condom consistently. In the final logistic regression, females who had tested for HIV were less likely to use a condom consistently. However, those who had obtained family planning information from print media and those from the northern parts of Ghana were more likely to practise consistent condom use. For males, those who professed the Traditional African religion were less likely to use a condom consistently. In contrast, those in the rich wealth category were more likely to use a condom consistently.
Our consistent condom use prevalence estimate (11%) is low compared to earlier studies on SSA use (25%–40%) (20–24). The conservative Ghanaian culture may explain the low prevalence rate. Young people in Ghana may be hesitant about purchasing a condom since sexuality and condom use issues are rarely discussed. Unlike in the less conservative cultures, condoms are not freely distributed to young adults of school age in Ghana. An earlier study in Ghana has established that although the majority of young adults in institutions of higher education use a condom, only a third indicated that they do this consistently due to issues of trust, non-availability and not liking condoms (24). Also, a recent study revealed that most adolescents had difficulties maintaining a budget for contraceptives, mainly condoms, to prevent unintended pregnancy (25). These factors have been identified within SSA as strong determinants of consistent condom use among young people and adults (8,10,21,23). The use of a single item to measure consistent condom use warrants a cautious interpretation of the reported estimate, as single-item measures may often result in higher estimates. Notwithstanding these plausible explanations, the low prevalence of consistent condom use among the sexually active sample in this study underscores the need for intensive public education on consistent condom use, particularly sexually active young adults.
Our logistic regression results showed that sexually active females who had tested for HIV were less likely to use a condom consistently, but those who had obtained family planning information from print media and those from the northern parts of Ghana were more likely to practice consistent condom use. The negative relationship between consistent condom use and knowledge of HIV status contradicts previous studies indicating that an HIV test encourages protective sexual behaviours among the general population (8,26). Our plausible explanation for this relationship is that knowing one’s HIV status may create a false sense of invincibility that allows one to engage in high-risk behaviours, including non-consistent condom use. Young people generally believe that consistent condom use reduces sexual pleasure; therefore, their desire for maximum fun from any sexual intercourse overrides the need to prevent STIs, including HIV.
Receiving family planning information from print media was associated with increased odds of consistent condom use. This finding is consistent with other studies conducted within SSA where exposure to family planning information is associated with contraceptive use, including condom use (27–31). This finding is encouraging and calls for governmental agency to increase the discussion of family planning issues in various media, especially through the radio. We also observed in this study that female sexually active young adults from the northern parts of Ghana were more likely to practice consistent condom use. These findings are encouraging as condom use in some regions in northern Ghana is influenced by misconceptions. Notably, those who use contraceptives, including condoms, are stigmatised and ridiculed as promiscuous (32). Consistent condom use among female young adults confirms a current study that found condom use to be the most popular contraceptive method among young women in northern Ghana (33). It is also plausible that these young females may not want to be pregnant to continue their education, although sexually active. This change in attitude towards condom use in northern Ghana may partly be as a result of the ongoing numerous intervention programmes on sexual and reproductive health in these parts of the country (34).
We also found that males who professed the Traditional African religion were less likely to use a condom consistently. Conversely, males in the rich wealth category were more likely to use a condom consistently. Religion is one key social and cultural factor (35) with a pervasive influence on the norms, values, structures and institutions that have a profound impact on individuals’ behaviours and decisions (36). For participants who professed the Traditional African religion, the consistent non-use of a condom could be attributable to their norms and show of sexual prowess. It is also possible that the lack of consistent condom use among young males professing the Traditional African religion could be the result of masculine validation of the fulfilment of cultural norms and beliefs. Only a few studies have explored the relationship between financial resources/wealth and consistent condom use. The finding that wealth increases the odds of consistent condom use is not surprising because people with sufficient resources can ensure the constant purchase and use of condoms. These findings underscore the need for the Ministries of Education and Health of Ghana to collaborate to ensure that affordable condoms are made available and distributed to young adults across the country. This strategy will ensure that access to condoms (and their subsequent use) may be available to youth irrespective of their socio-economic status.
Limitations of the study
The findings of this research should be interpreted cautiously due to the following limitations. First, the cross-sectional nature of the data weakens the evidence of causal relationships among the study variables. Second, the study relied on self-report measures, which could be affected by social desirability or memory bias. In the Ghanaian context, where sexual communication and education are scarcely discussed, it is possible that the responses to the consistent condom use variable could have been overestimated due to social desirability bias. Finally, we found that several variables such as low self-efficacy with regard to condom use, condom use fatigue and low personal risk of STIs [8,10], which are known to influence consistent condom use, were not explored in this study. It is therefore recommended that future studies address these limitations to help provide a better understanding of the factors that influence consistent condom use among adolescents and young adults who are sexually active. A qualitative research approach should also be used to explore some possible power dynamics in condom use. Notwithstanding these limitations, our findings are consistent with some previous studies, an indication that our results may apply to other sexually active young adults in Ghana. Additionally, the large sample size provides the study with sufficient power, and the representativeness of the sampling strategy and the nationwide nature of the data boost the study’s generalisability to other settings.
Conclusion
Using the 2014 GDHS, this study explored the determinants of consistent condom use among sex-ually active young adults in Ghana. Approximately 11% of the respondents reported consistent condom use in their previous sexual activity. Females are more likely than males to have used a condom consistently. Our findings underscore the need for behavioural change campaigns targeting young adults, particularly those who are sexually active. These interventions should target young adults who have less knowledge about family planning, know their HIV status and who profess the Traditional African religion. Additionally, HIV testing should be encouraged and be accompanied by other measures such as pre- and post-test counselling geared towards appropriate sex education.