
Abstract
It has been recognized since antiquity that the organization of society and how it distributes resources are the primary determinants of health. Yet most definitions of health in the academic and practice literatures limit their focus to the individual’s experience of health and functional abilities, neglecting the structures and processes of societies in which the individual is embedded. We draw upon developments in the critical health communication and critical materialist political economy of health literatures to provide a definition of health that directs attention to the role that economic and political systems play in either equitably or inequitably distributing the resources necessary for health. Since these distributions interact with the individual’s unique biological and psychological dispositions and situations to produce health, it is important to identify their sources and means of making their distributions more equitable. Because it is through communication that humans interpret society, themselves, and others, a concise definition of health that draws attention to these societal features and their roles on a day-to-day basis in promoting or threatening health is essential.
Introduction
In 1948, the World Health Organization (WHO) provided its iconic definition of health which continues to influence contemporary discourses in health (1). Its definition, like most others, is focused on the individual rather than the environment in which the individual is embedded. This was not completely inappropriate considering the attention paid to promoting well-being during the immediate post-World War II era. However, much has changed since the ‘Golden Age of Capitalism’ which provided many of the resources necessary for health (2). It seemed to us that in the current era of unbridled capitalism, global accepta-nce of neo-liberal approaches to governance, and imposition of austerity, a definition of health that incorporates contemporary political and economic trends was in order. In this article we provide such a definition within a critical materialist political eco-nomy perspective with the purpose of spurring rec-ognition of these forces and the threats they pose to health (3). Such effort is important since, as pointed out by Leonardi (4):
The definition of health is not just a theoretical issue, because it has many implications for practice, policy, health services, and health promotion. The definition of health affects health professionals, and in turn they strongly affect how health is socially constructed in modern societies. The social representations of health influence the demands and expectations of health, the health care systems, the policy makers, and many other key aspects of health (p.736).
The most widely used definitions of health focus on the individual and their subjective sense of health and functional abilities. We draw upon a critical health communication approach that recognizes that since language shapes our understandings of health and means of promoting it, a definition of health that moves beyond the individualistic approaches that dominate health care, health promotion, and health messaging towards one that makes explicit how societal structures and processes shape health is necessary.
To do so, we apply a critical materialist political economy analysis of health that directs attention to the economic and political structures that shape health. Conveying this concept within a definition of health will stimulate recognition and understanding of the forces that shape ‘society, nature, themselves, and each other’ (5, p.85). Ultimately, we aim to contribute to ‘an emancipatory politics that seeks structural transformation’ in the service of health (6, p.1).
Critical materialist political economy
A critical materialist political economy analysis of health considers health to be an outcome of economic and political systems as well as societal structures and processes (7), and is explicitly concerned with the imbalances of influence and power amongst societal sectors that shape these forces (8). The mediating mechanism between these structures, processes, and forces is the quality and distribution of social determinants of health such as income, employment security, working conditions, food and housing security, and health and social services (9).
In addition to their material effects upon health, these structures, processes, and forces also shape the ideas a society holds about health and the means of promoting it (9). More specifically, a critical materialist analysis identifies how the power and influence of specific societal sectors – usually the corporate and business sector – create public policies that lead many to lack the economic, political, and social resources necessary for health. Through a definition of health that considers these issues, new ways of thinking about health and the means of promoting it can be communicated.
Critical health communication
Health communication theory and research is dominated by traditional approaches that do little to question existing structures of domination and influence (10). Critical health communication theory aims to rectify this.
Lupton (11, p.57) considers the role culture plays in health communication with culture including ‘ideas, beliefs, language, institutions, and structures of power’ such that ‘health, illness, and disease may be considered products of cultural practices.’ For Lupton (11), then, the critical health communication approach sees health as a product of social systems and ideological processes (p.58), a point more recently made by Ellingson (12, p.2): ‘Body-selves are constituted both through relationships within others – interpersonally, organizationally, in communities – and within larger social and political structures.’
Critical health communication studies ‘focus on how communication constructs ideology, taken for granted assumptions about reality that structure social decision making and everyday life in ways that systematically reinforce the interest of dominant groups’ (13, p.351). Zoller and Kline (14, p.119) argue that critical health communication research ‘addresses issues of health meanings’, ‘articulates... linkages among communication and politics, policy and social power; deconstructs taken-for-granted assumptions about health and illness and conceptualizing alternatives; and describes direct implications for practice.’
Dutta (15) concurs, stating critical health communication scholarship seeks to uncover ‘the structures within which meanings of health are constituted’ (p.534), urging scholars to be critical of power, structures, processes, and practices that create and disseminate knowledge.
The WHO definition of health
The WHO’s definition of health was first articulated in 1948 (1): ‘Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.’ This definition helped broaden understanding of health and its determinants, opening the concept to a wider community where previously it had been the sole domain of the healthcare system and its professionals.
The core criticisms of the WHO’s definition as ‘difficult to measure and impossible to achieve’ is presented by Blaxter (16, p.2). The WHO definition is a product of its times, situated within the immediate post-World War II period where Keynesian reforms were dominant, market forces were subject to state management, and the modern welfare state established. The post-war period was also characterized by a demand for globally recognized human rights including the right to health (17).
Indeed, Nobile (18) argues that during the era of the WHO definition, global peace and health were inseparable, with recognition that health was related to economic and political conditions and an apparent willingness on the part of governments to act on these understandings to promote the health of populations. While the WHO’s definition of health has been contested, most of the new definitions do not take account of changing political and economic conditions.
Methods
We used Google ScholarTM to identify existing definitions of health in the academic literature from 1948 – the year of the WHO definition – to the present by searching the terms ‘definitions of health,’ ‘defining health,’ and ‘health definitions.’ Martín-Martín et al. (19) show that Google ScholarTM yields significantly more citations than ScopusTM, WoS Core CollectionTM, and Web of ScienceTM in the coverage of academic literature in humanities and social sciences. We did the same search using GoogleTM to identify definitions created by agencies and organizations.
We reviewed these definitions to determine their foci and the extent to which they were concerned with the individual versus broader societal factors that shape health. Of particular interest was their consideration of how economic and political systems and structures and processes of society and the power and influence of specific sectors such as the corporate and business sector shape the quality and distribution of a variety of social determinants of health.
Findings indicated the need for a definition of health that considered how economic and political systems and the power imbalances inherent in them create the living and working conditions that determine health. The following sections provide details on how we did so.
Findings
Additional definitions – individualistic approach to health
We found numerous definitions of health in the academic and practice literature. Most focus on the individual and set parameters around the meaning of health as experienced by an individual. Many of these – like the WHO definition – continue to have the individual as their focus (see examples in Table 1 (1,4,20–26)).
Examples of health definitions that focus on the individual.
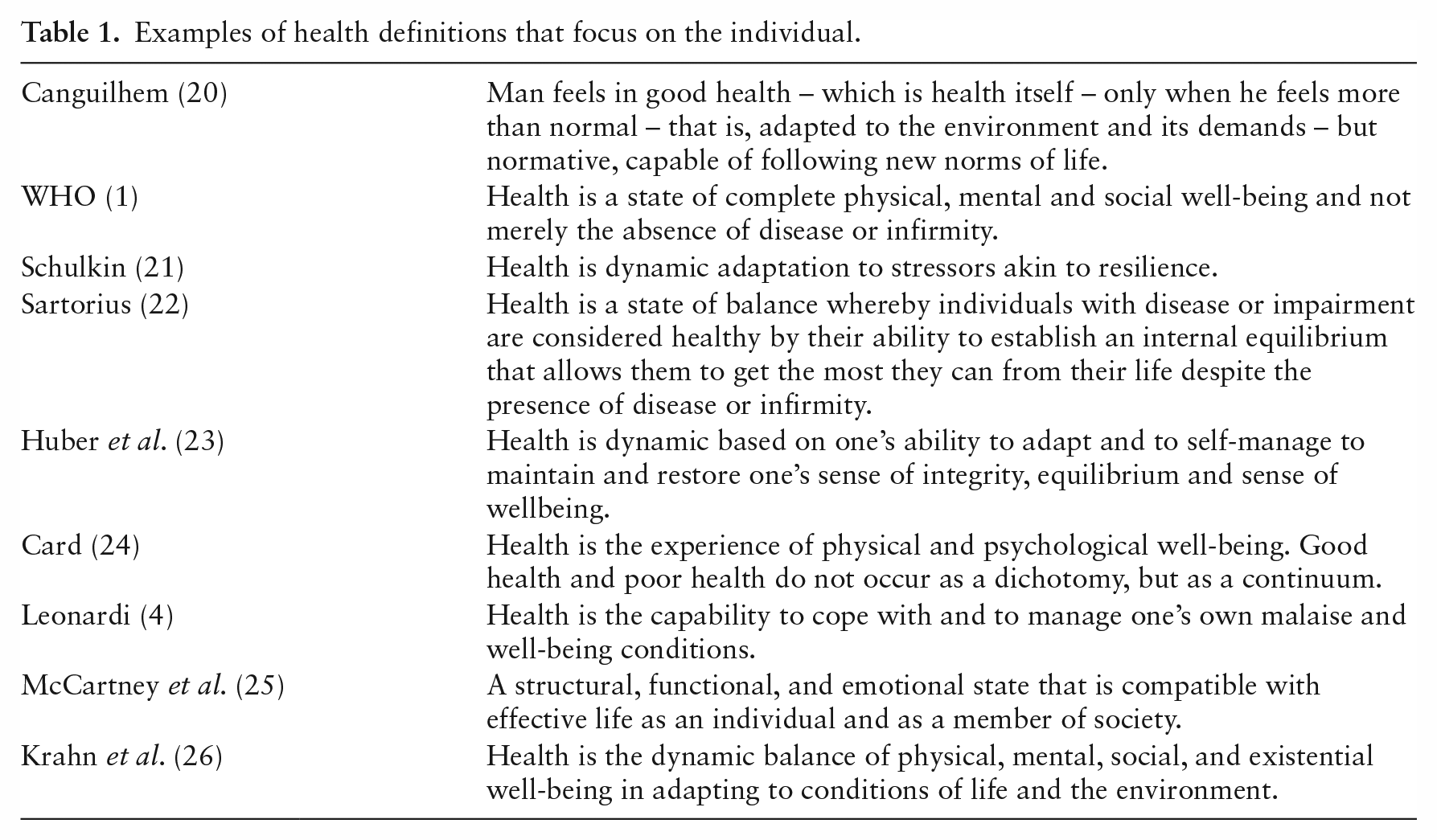
Most definitions focused on the individual (25,26) with what Kelman (27) identified as experiential and functional components. Kelman (27) defines experiential health as ‘freedom from illness, the capacity for human development and self-discovery, and the transcendence of alienating social circumstances’ (p.7) and uses Parson’s definition for functional health: ‘State of optimum capacity of an individual for the effective performance of the roles and tasks for which he has been socialized’ (27, p.14). The functional approach is open to the critique that health can be primarily defined as being able to contribute to existing modes of production in capitalist society.
A Lancet editorial (28) enthusiastically endorses Canguilhem’s (20) definition of health as the ability to adapt to environmental demands and while emphasizing important aspects of personal agency is also somewhat limited: ‘It puts the individual patient, not the doctor, in a position of self-determining authority to define his or her health needs.’ It is limited in that it removes from explicit attention the structures and processes of society and consideration that the individual may have mistaken understandings of these structures and processes that impede their health.
The decoupling of health from the presence or absence of disease in many of these definitions has certainly advanced understanding of the experience of chronic illness and disability and removed medical stigma from those experiencing these states. Yet, the continuing focus on the individual in these definitions, rather than the political and economic systems in which individuals are embedded, does not direct attention towards the structures and processes of society that determine health. The following section provides examples of attempts to do so.
Additional definitions – moving beyond the individual
Table 2 (29–32) provides some exemplars of definitions moving beyond the individual and most do so by mentioning various social determinants of health. In 1986, the Ottawa Charter for Health Promotion (29) brought social resources into its definition of health and identified important pre-requisites of health, peace, shelter, education, food, income, a stable eco-system, sustainable resources, social justice and equity. These features are now commonly referred to as social determinants of health; factors incorporated into Shilton and coll-eagues’ (30) definition of health.
Examples of definitions of health moving beyond the individual.
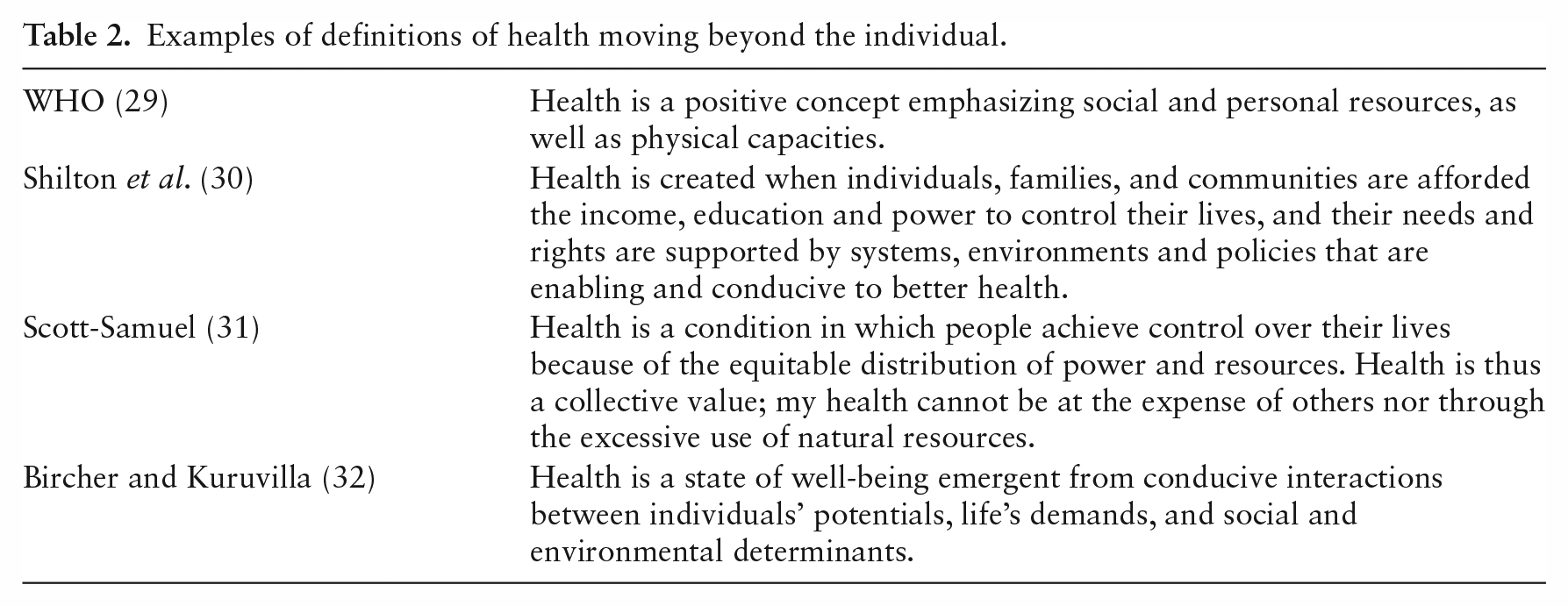
Scott-Samuel (31) employed aspects of a critical materialist analysis to chide Shilton et al. (30) for neglecting the role neo-liberal capitalism plays in threatening health: ‘They also fail to point out that the inequity which as they say, rations global access to health, is a systematic product of the neoliberal capitalism which so dominates global public policies and international relations.’
More recently, Bircher and Kuruvilla (32) made the role of social and environmental factors more explicit, but even then, their definition does not draw attention to the structures and processes of economic and political systems that shape the living conditions they identify such as housing, food security, income, working conditions such as employment security, wages and benefits, work demands and control; and other supports and services like health care, social services, and universal benefits.
The contribution of civil society and non-governmental organizations
We also found a variety of discussions that make explicit some of the economic and political forces that shape health, although none of these examinations provide a precise definition of health that could serve the purpose of shifting day-to-day discourse around health and the forces that shape it. The People’s Health Movement’s (33) People’s Charter for Health states:
Health is a social, economic and political issue and above all a fundamental human right. Inequality, poverty, exploitation, violence and injustice are at the root of ill-health and the deaths of poor and marginalised people. Health for all means that powerful interests have to be challenged, that globalisation has to be opposed, and that political and economic priorities have to be drastically changed (p.2).
UBC Health’s (34) definition is also helpful: ‘Health is an attribute of individuals, communities, and societies and is a fundamental resource for daily living.’ The Lincy Institute (35) states: ‘A person’s health is a product of their environment. As such, a healthy community is one in which all residents have access to a quality education, safe and healthy homes, adequate employment, transportation, physical activity, and nutrition, in addition to quality health care.’ However, neither the People’s Health Movement nor the other agencies provide a concise definition of health that considers the role played by economic and political structures in determining the quality and distribution of these resources.
A critical materialist political economy analysis
From a critical materialist political economy perspective, the primary issue with individually focused definitions of health is their lack of recognition of how economic, political, and social forces enable or threaten health. Second, these definitions usually assume that the state or the government – can and will – take some res-ponsibility for the health of its people through public policy action. Increasingly, this is not the case (9).
We offer a definition that makes explicit that health is dependent on four interconnected and interdependent conditions: economic, political, social, and individual. We employ a critical realist analysis to identify what has been termed the real, actual, and empirical levels of reality (36). Such an analysis allows for consideration of what is possible in addition to what currently exists.
In our analysis, the real involves an explication of the societal structures and powers of the economic and political systems that have the capacity to promote or threaten health. This focuses attention on the means of production and distribution in a society and how the political system facilitates or inhibits these processes. The actual in our present effort are the forces that activate these structures and processes. What are the means by which some jurisdictions act to support health through the equitable and health promoting provision of economic, political, and social resources while others do not? Finally, the empirical is the world of experience or the observable with regard to the provision of the resources necessary for health. These involve the distribution of what have been termed the social determinants of health as well as the experience of health itself.
Economic conditions
Any analysis of economic conditions can begin either with examination of the structures and processes of the economic system, the forces that activate or inhibit these structures and processes, or their manifestations in concrete lived experience (3). Most nations produce and distribute economic resources under the aegis of capitalism (the real) and analyses of their structures and processes are abundant. In some forms, the capitalist system is managed (the actual) such that arguably almost all have access to the resources necessary for health. The forces leading to the actual are working class power, extent of unionization and collective agreement coverage, and dominant political parties, usually influenced by the presence of proportional representation in the electoral process (37).
The empirical are the working conditions and work environments that either promote or threaten health. These can include gender pay equity, protection against child labor and exploitation of young workers, protection against racism in the workplace, access to parental leave compensation, access to wage compensation in the case of loss of or change in ability (for oneself or of dependents), and compensation for caregiving supports, among others.
Political conditions
The structures and processes of the political system constitute the real level, with how these come to shape the distribution of power through the enactment of laws and regulations constituting the actual (38). The extent of political expression, participation, and influence among those of differing social locations represents the empirical.
At the level of the real, the political system can enact proportionate representation in the electoral process, regulate the market through enactment of laws and regulations governing wages, benefits, and working conditions, implement taxation to provide support programs and decommodified services such as health and social care, child benefits, unemployment benefits, pensions, active labor policy, affordable and quality housing, agricultural, food pricing, water and sanitation regulations, and access to affordable education, among many others (39).
The extent to which they actually occur represents the empirical level and is activated at the actual level by many of the same forces working on the economic system: governing parties, working class power, unionization and collective agreement coverage.
Social conditions
Social conditions include the ability to build social and community networks to foster social engagement and participation, as well as the avoidance of racism, sexism, ableism, and ageism, and an environment open to debate and free expression (3). The development of human potential, however defined, can also be included. These manifest as a result of the organization of the economic and political systems and the manner in which they produce and distribute resources as described above.
Individual factors
While individual factors interact with political, economic, and social conditions, there is no denying that there are distinct biological characteristics such as inherited genetic conditions and gene mutations, stages of the life course, psychological dispositions such as resilience and coping strategies, and life events (40). While certainly important to the individual, the overall contribution of the individual factors of genetic and psychological characteristics to population health are rather limited since the main killers – cancers, cardiovascular, and respiratory diseases – are related to environments rather than the effects of unfolding genetic dispositions and psychological characteristics which themselves are shaped by environmental circumstances (41,42).
Our definition of health
Based on these considerations, we offer a definition of health which incorporates Kelman’s (27) concepts of experiential and functional health and the critical materialist political economy analysis of how economic and political systems distribute the resources necessary for health:
Health – as experienced by the individual (experiential) and their ability to carry out life’s activities (functional) – is a product of the interaction of economic and political systems’ equitable or inequitable distribution of financial resources, political power, and social supports with the individual’s unique biological and psychological dispositions and situations.
Discussion
Most definitions of health direct attention to the individual’s experiential and functional health rather than the political, economic, and social conditions that shape it. As a result, inquiry into the public policies and the economic and political forces that shape how these policies distribute the social determinants of health is frequently neglected. An explicit examination of how economic and political systems shape health is even less common. We believe our definition of health addresses this neglect and will direct attention to these and additional issues discussed below.
Making the economic and political determinants of health visible
Bates et al. (43) argue that individualized and decontextualized definitions of health are ‘removed from the social, economic, and environmental contexts in which that individual resides’ (p.2). This removal advantages dominant regimes and reproduces existing systems that threaten health. We want to force health providers, health pro-moters, and policymakers on a day-to-day basis to face the question: How do existing societal structures and processes – both economic and political – shape health?
There is growing interest in how the capitalist economic system threatens health with its generating economic crises, declining quality and equitable distribution of the social determinants of health, and a climate crisis moving Earth towards a climate catastrophe (44,45). Our definition of health makes these broader issues difficult to ignore.
Health, functional health, and capitalism
The concern with the health effects of capitalism is not new. Fifty years ago, Kelman (27) argued that in capitalist society, where capital accumulation is the primary goal of economic and political organization, there is an inherent contradiction between functional health – the ability of the individual to contribute to the capitalist accumulation process primarily through labor – and experiential health – avoiding objectification of the self, alienation from self, others, and society, and the experience of illness. This contradiction comes about because of the constant imperative of business and industry to increase profits set into motion by two prominent processes: the expansion of markets and the reduction of costs. Indeed, Das (46) details how the processes inherent to capitalism create health threatening living and working conditions.
Consistent with our analysis, Kelman (27) pointed out how concern with individualized functional and experiential health in the absence of attempts to transform the economic and political systems causing these health problems led to an array of biomedical and psychological interventions to remedy health problems. The continuing emphasis upon biomedical and behavioral approaches to health illustrates how Kelman’s observations of 50 years ago of health as defined under capitalism remain germane today (47).
Gaining the attention of clinicians, health promoters, researchers, and policymakers
We believe therefore that our definition of health will spur health promoters, researchers, and policymakers in their day-to-day work to move beyond focus on the individual and consider the social determinants of health and how economic and political systems produce and distribute them within their society. There have been many calls for this to occur; our new definition of health makes this an ongoing imperative. Experiential and functional health continue to be important, but these are now explicitly placed within their societal context.
Bircher and Kuruvilla (32) provide suggestions on how many of the concepts in our definition can be applied at the individual and population levels. Clinicians can assess the present state of patients’ current exposures to various social determinants of health and identify resources that can provide assistance. They suggest ‘Governments could use the Model to think through how best to provide adequate health and social interventions, and the related legal rights and entitlements’ (p.382).
From our perspective our definition can help identify how economic and political systems and other societal structures and processes shape the quality and distribution of numerous social determinants of health. Especially important would be consideration of how the power and influence of specific societal sectors such as the corporate and business sector threaten the quality and make equitable distribution of various social determinants of health difficult.
Environmental conditions
We do not place environmental conditions – including the climate crisis – in our definition, to not over complicate an already complex definition. Yet these conditions and overall planetary health are important determinants of health and are closely related to the economic and political systems we describe above. Although environmental conditions have a significant impact on health, in this article we focus on economic and political structures and processes yet do not deny that environmental issues provide a strong background context to our definition of health.
Conclusion
Definitions of health direct attention to what is important for promoting health through research, public policy, and health care services. We offer a definition of health that makes these usually invisible forces – especially how the economic and political systems distribute resources to either promote or threaten health – visible on an ongoing basis and therefore provide targets for action. These targets will include clinical activities on a day-to-day basis to meet the needs of patients, develop research agendas to illuminate the societal structures and processes that either promote or threaten health, and public policy advocacy to improve the quality and distribution of the social determinants of health. Our definition of health may also help build social and political movements to transform health threatening economic and political systems (48).