
Abstract
Background:
There is a higher incidence of cardiac arrest in economically deprived areas; however, data show that bystander cardiopulmonary resuscitation (CPR) in those areas is lower. This results in lower survival rates, placing those communities at a double disadvantage. This systematic review explored the barriers and facilitators to engaging with bystander CPR in deprived communities.
Methods:
Studies were eligible for inclusion if they addressed any barrier or facilitator to performing bystander CPR or being trained in CPR or training others. Studies had to either be set in a deprived area or examine a deprived population. Selected studies were published between January 2000 and December 2017 and reported on primary research. No language limitations were applied. Searches were conducted in the following databases: Cumulative Index to Nursing and Allied Health Literature (CINAHL), MEDLINE, PsycINFO, PubMed, and Web of Science Core Collection. Unpublished ‘grey’ literature was also searched as well as the reference lists of any relevant studies.
Results:
The systematic review highlighted several main factors acting as barriers or facilitators to engaging with bystander CPR in deprived communities: (1) the willingness to learn or perform CPR, (2) the confidence to perform CPR, and (3) self-reported likelihood of performing CPR. The review also revealed additional barriers to engaging with CPR which are specific to – or more acute for – individuals from socioeconomically deprived backgrounds or areas.
Discussion:
We found little evidence suggesting that the willingness to perform or learn bystander CPR is lower in deprived communities compared to the general population. However, the confidence to perform CPR in deprived communities was affected by some measures of socioeconomic status. The results also crucially highlighted other barriers more acute in deprived communities: the risk to personal safety in administering CPR; the fear of legal consequences; and the lack of community cohesion and other cultural barriers.
Introduction
Out-of-hospital cardiac arrests (OHCAs) are a major cause of mortality worldwide, and the burden they represent on health services is not fully known.1,2 Globally, survival from OHCA remains low and variable within regions with estimates ranging from 7.6% in Europe, 6.8% in North America, 3.0% in Asia, and 9.7% in Australia. 1
OHCA survival rates remain poor and have seen little improvement in recent decades. 3 One of the main factors influencing the rate of survival is the administration of bystander cardiopulmonary resuscitation (CPR). 4 There is an apparent willingness among the general population to administer bystander CPR, 5 born out of a desire to save lives especially if the victim is a family member. 6 However, a number of barriers often prevent people from performing bystander CPR, regardless of whether they are CPR trained or not. Some of these barriers include a reluctance to perform CPR on a stranger, 5 particularly if the victim seems unkempt or under the influence of drugs or alcohol, 7 a fear of being sued,8,9 or a fear of performing CPR wrongly and of potentially doing more harm than good.5,10,11
Countries that have renewed their efforts to increase the number of people trained in CPR have seen significant improvements in their OHCA survival rates. For instance, in Sweden, a CPR training policy which saw a third of the total population trained over three decades resulted in an increase in OHCA survival at 1 month from 5% in 1992 to 11% in 2011.12,13 A similar strategy in Denmark resulted in a rise in overall survival to discharge from hospital from 6.5% to 19.1% between 2001 and 2010 14 .
Rates of bystander CPR are generally lower in socially and economically deprived areas, in rural areas, and within certain ethnic populations.9–11 Sasson et al. 15 found that victims of OHCA in low-income black neighbourhoods in the USA were less likely to receive bystander CPR than those in high-income white neighbourhoods. Another study in North East England found that residents living in the least deprived areas were significantly more likely to receive bystander CPR than those in the most deprived. 16
Besides the fact that they are less likely to receive CPR, people living in socially deprived communities are also less likely to be trained in CPR. Studies have found that lower education and lower incomes were associated with a decreased likelihood of being trained in CPR.17,18 Furthermore, Anderson et al. analysed data on over 13 million people who had received CPR training across all 3143 counties in the USA between 2010 and 201. They concluded that the rates of CPR training were lower in black and minority ethnic communities and in lower income households. 19 However, it is still unclear why people living in deprived communities are less likely to give life-saving CPR and what factors could improve this.
Therefore, the aim of this systematic review was to identify the barriers and facilitators perceived by individuals in socioeconomically deprived circumstances to engage with bystander CPR. We defined the term ‘engaging with bystander CPR’ as encompassing the willingness/confidence to learn CPR, to perform bystander CPR, and to teach/encourage others to learn/engage with bystander CPR.
Methods
This systematic review was conducted according to a registered (PROSPERO CRD42017081944) and published protocol. 20 Studies were eligible for inclusion if they addressed any barriers or facilitators to performing bystander CPR for OHCA or being trained in CPR or training others, from a potential OHCA bystander’s perspective. The following data items were sought: authors; country; year of data collection; study aims; sample; design; and barriers/facilitators outcome measures and analysis themes. An inductive approach was used to identify barriers and facilitators in keeping with definitions proposed by Bach-Mortensen et al. 21 Facilitators were defined as any factor that contributes to the delivery of bystander CPR. Barriers were defined as any factor that obstructs the delivery of bystander CPR. Studies had to either be set in a deprived area or examine a deprived population. Selected studies were limited to those published between January 2000 and December 2017 and reported on primary research. No language limitations were applied.
Search strategy and selection criteria
Searches were run on 5 December 2017 in the following: CINAHL, MEDLINE, PsycINFO, PubMed (Ahead of Print Citations and articles published in the last 6 months only) and Web of Science Core Collection (Science, Social Sciences and Arts and Humanities Citation Indices; Science and Social Science & Humanities Conference Proceedings and Books Citations Indices; and Emerging Sources Citation Index). (See sample search strategy, S1 in Supplementary Materials.) Search results were examined for relevant studies already known to the review team. Selected search terms were used in Google.co.uk, experts contacted, and reference lists checked for further studies.
We excluded studies that only addressed bystanders’ use of defibrillation as our focus was on the second stage in the chain of survival (‘early CPR’) 21 and the defibrillation evidence was recently reviewed. 23 We included any age group from all community settings (e.g. homes, schools, workplaces, public and private communal spaces for lay perspectives). We excluded studies with people trained and certified in CPR as part of their professional (including medical and pharmacy students), statutory (e.g. care-home staff) or voluntary roles, and studies set in medical and primary, secondary, and tertiary healthcare settings. Qualitative, quantitative, and mixed methods studies were eligible provided they collected primary data or conducted secondary analysis of existing data. Conference abstracts and unpublished ‘grey’ literature were also eligible and were sought through web searches, informal stakeholder interviews (from the wider project team), and our study advisory group. The reference lists of all relevant reviews were checked for additional studies to reduce the risk of bias through omitted inclusion of relevant papers.
Systematic reviews, evidence-based guidelines, and opinion pieces were excluded. Studies were eligible if they used any indicator of socioeconomic deprivation for the setting or sample including, but not limited to: educational status; employment status; income; occupation; poverty; social change; social class; social condition; or neighbourhood/area status. Study findings could report entirely from a socioeconomically deprived population or area or be segmented by a socioeconomic indicator and report from a deprived sub-population or area. For studies where the whole sample was from a socioeconomically deprived population or area, the deprivation criteria was required to be reported by the study’s authors. The review was part of a wider study to inform the development of an intervention for deprived UK communities, thus only studies from Organisation for Economic Co-operation and Development (OECD) member countries were eligible (http://www.oecd.org/about/membersandpartners). These tend to have high-income economies but may also have socio economic inequalities and deprived communities.
10% of records were double-screened on title and abstract by two reviewers to pilot the screening checklist. Following refinements, a further two batches of 10% of records were triple-screened on title and abstract by reviewers until high agreement was reached. Disagreements over inclusion were resolved by discussion. The remainder were single-screened by the same three reviewers. Coding conflicts mostly related to the reason for excluding a record, not whether it should be included or excluded. A disproportionately large number of full-text studies required assessment against the inclusion criteria as it was unclear from study records whether findings were segmented by socioeconomic indicators or not. A full-text fast-screening stage was developed to assess the deprivation inclusion criterion only. Two reviewers single-screened full texts, using socioeconomic terms and deprivation terms from our search strategy. If no deprivation terms were identified, they closely read the sample and setting sections, and the results text and tables. The remaining full texts were assessed independently against the complete inclusion checklist by one reviewer performing the assessment and another checking the decision. Disagreements over inclusion were resolved by discussion.
Critical appraisal
A quality assessment was made of all studies, using an appropriate tool by study design: the CASP Qualitative Checklist, 24 the NIH Quality Assessment Tool for observational cohort and cross-sectional studies, 25 and the NIH Quality Assessment Tool for before-after (pre-post) studies with no control group. 26 We deviated from the tools stated in the protocol as none were suitable for the latter two study designs. One reviewer applied the criteria to assess the quality of the included papers. A second reviewer made a detailed check of all the assessments. Any discrepancies were resolved through consensus.
Data analysis
Relevant data were extracted into a customised form: aim, design, country and year of data collection, sample and setting, outcome measures, and findings. For studies where the sample was segmented by a socioeconomic indicator, only data related to the deprived sub-population or area were extracted. Data were extracted by one reviewer and a proportion checked for accuracy by a second. Review authors were not contacted for missing data. The extracted data (outcome measures and results) were heterogeneous, so neither a quantitative nor a qualitative meta-analysis was appropriate. To inform the narrative synthesis, data were organised thematically, and the analysis was refined through discussion. Significance and p-values are reported if they were provided in the original articles.
Results
The searches produced 1219 unique records to be screened against our criteria, with 338 assessed as full-text articles (see Figure 1). Nineteen studies, reported in 21 papers, met the criteria and were included for analysis.7,27–46 Characteristics of included studies are listed in Table 1. Four studies were rated on the quality of their methods as ‘good’ (their findings had a low risk of bias); eight were rated as ‘fair’; and seven were rated as ‘poor’ (their findings had a high risk of bias) (See S2 in Supplementary Materials). Most studies were conducted in Europe (n = 8; from Denmark, England, France, Ireland, Italy, Spain (n = 2), Sweden), followed by North America (n = 6; United States), Asia (n = 3; from Japan (n = 2), South Korea), and Australia (n = 2). All were published articles (no grey literature), published between 2000 and 2017 with data collected between 1998 and 2015 (unreported by three studies).
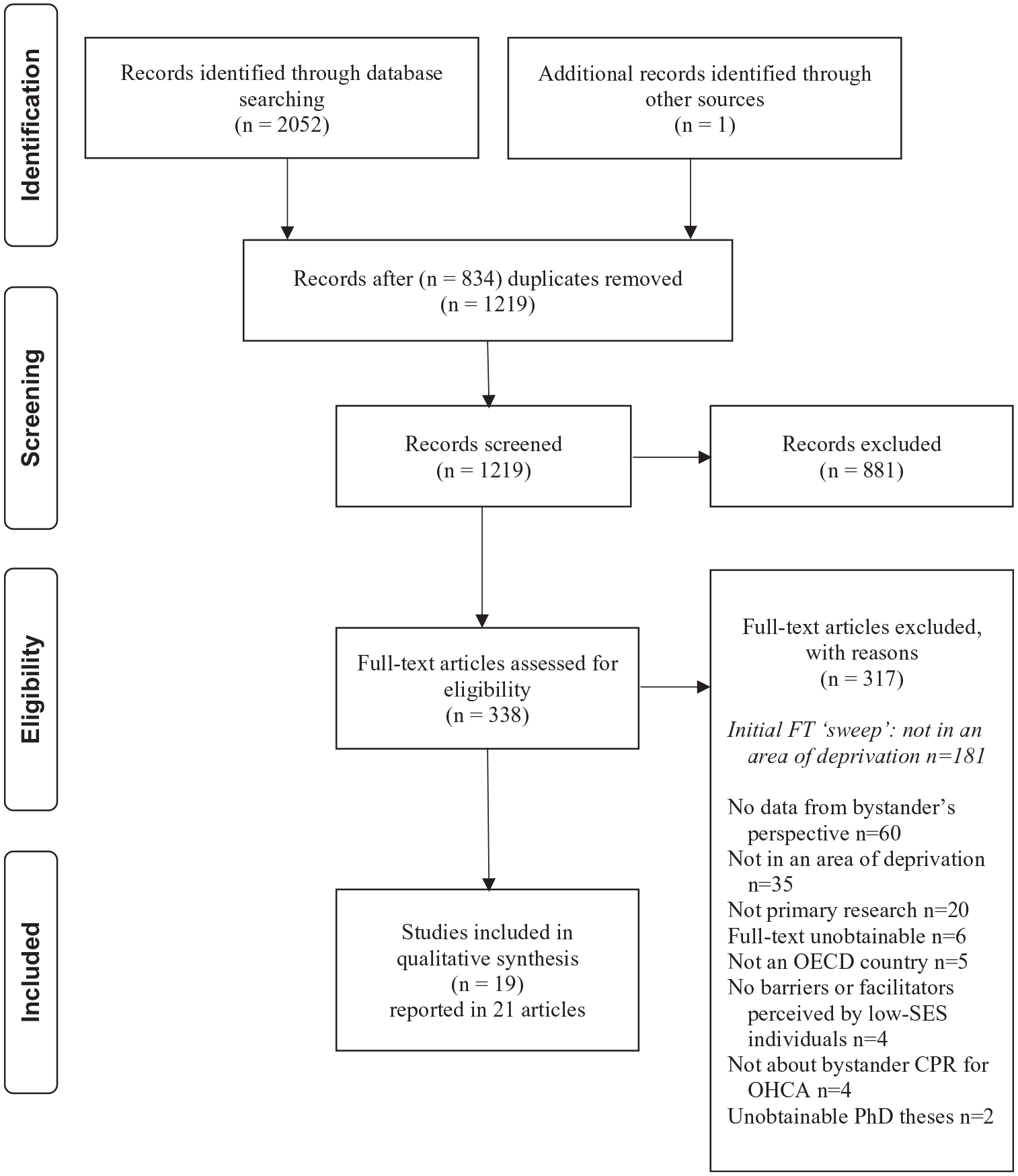
Flow of information through the phases of the systematic review.
Characteristics and quality appraisal grading of the included studies.
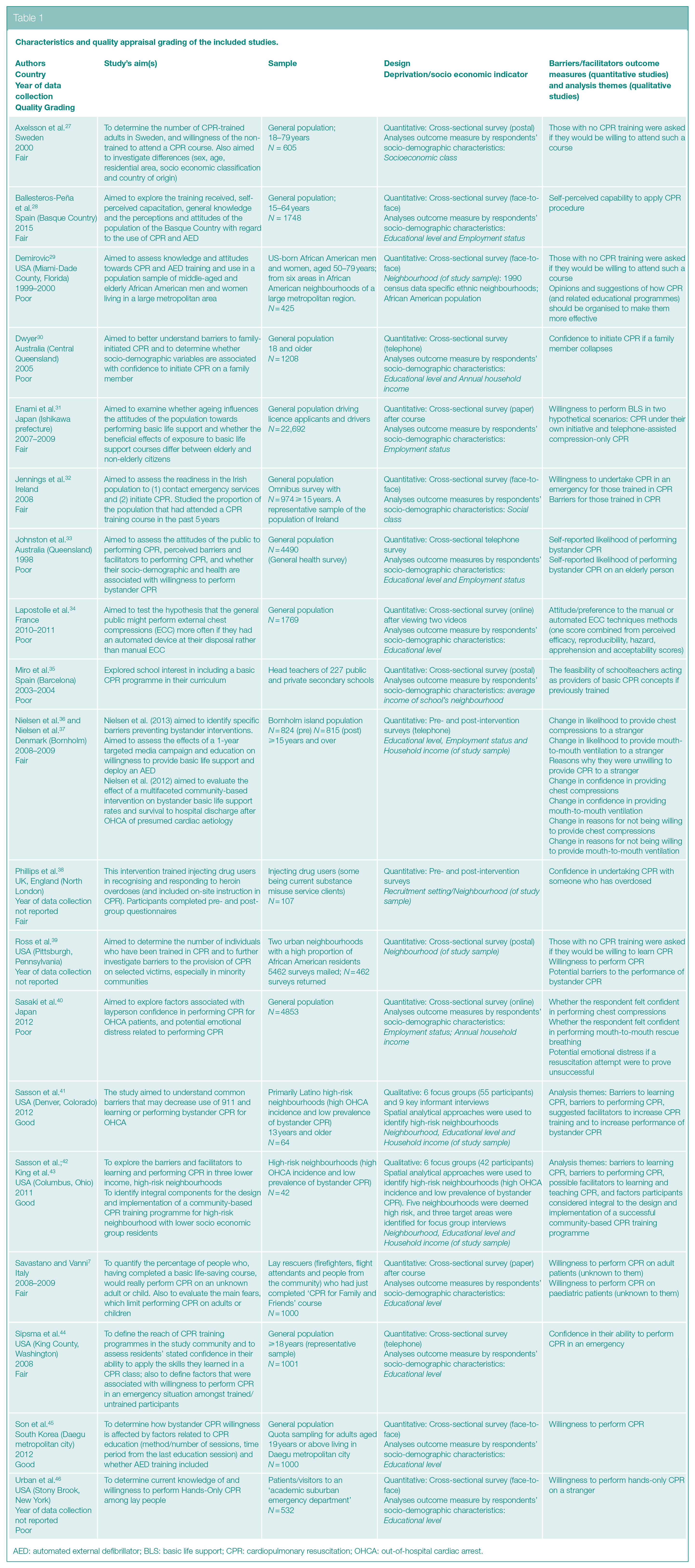
AED: automated external defibrillator; BLS: basic life support; CPR: cardiopulmonary resuscitation; OHCA: out-of-hospital cardiac arrest.
Socio-demographic indicators
Six studies (reported in eight articles) specifically targeted a socioeconomically deprived population or area.29,36–39,41–43 Four were studies in deprived urban neighbourhoods in the USA29,39–43 described as having ‘economic disadvantage’, ‘lack of health insurance’, and being ‘underserved’: three in predominantly African American neighbourhoods (one qualitative study,42,43 and two surveys)29,39 and one qualitative study in a Latino neighbourhood. 41 A UK intervention study recruited from a drug dependence unit, hostels for homeless people and primary care facilities 38 and a Danish intervention study took place in a rural area with lower educational levels and higher unemployment and absence due to illness rates than the rest of country36,37 (See S3 in Supplementary Materials for full descriptions of indicators). The remaining 13 studies were cross-sectional general population surveys and were eligible because the sample was segmented by a socio economic indicator with findings reporting potential barriers or facilitators for the lowest category of the socio-demographic indicator. Eight studies reported findings by education level,28,30,33,34,44–46 six by employment status or social class,27,28,31,32,33,40 four by household income,30,40,45,46 and one by neighbourhood income. 35 (Some studies reported by more than one indicator.)
A Synthesis of Findings from the Included Studies
Learning bystander CPR
Six studies examined willingness to learn CPR, the feasibility of teaching it in schools, or barriers to learning.27,29,35,39,41–43 Three surveys27,29,39 explored willingness to learn CPR, among untrained populations. A Swedish population survey 27 indicated that people with a lower social-economic classification (unemployed or manual work) were willing to learn CPR, although at lower levels than professionals and students/military. Two small surveys29,39 set in low-income, predominantly African American urban neighbourhoods found mixed results: a survey in Pennsylvania of a mixed age group found a high proportion of participants were willing to learn CPR; 39 however, results were much lower in a survey with older respondents in Florida. 29 The latter also found that few respondents were aware of places where CPR training took place or who to contact to attend. A further survey found that schools sited in below-average income Barcelonan neighbourhoods were as likely to be assessed as suitable for CPR training as average and above-average neighbourhoods. 35
Two qualitative studies in lower income predominantly Latino 41 and African American42,43 city communities found that residents may be less motivated to participate in CPR classes when learning CPR was not a job requirement. These studies also found financial barriers related to the high cost of attending classes, and difficulties finding transport and childcare to attend.
Willingness to perform bystander CPR
Seven surveys31,32,34,39,45,46 and one intervention study22,24 measured willingness to perform bystander CPR, some for CPR on specific victims.36,37,39,46 Four cross-sectional surveys measured willingness to perform bystander CPR and found few differences by socio economic status. A general population survey revealed that willingness to perform CPR did not vary significantly by social class in Ireland. 32 However, the survey question was asked only of those who had received CPR training in the last 5 years and respondents from lower socioeconomic classes were significantly less likely to have had training (p < 0.0001), meaning few would have been asked this. Using two hypothetical scenarios (CPR under one’s own initiative and telephone-assisted compression-only CPR), a large survey in Japan measured willingness to perform basic life support, which it reported by occupation: 31 there was no difference between students and those with no secure employment. The third survey, in a South Korean city, found no difference in willingness to perform CPR based on monthly income but willingness increased with level of education (from middle school graduate or under, to high school graduate, up to college graduate or higher (p < 0.001)). 45 A small survey in France found no differences by education level associated with preferred techniques to perform bystander CPR (manually, by automated device, or no preference (p = 0.09)). 34
A survey in a low-income, predominantly African American urban neighbourhood 39 found that a high proportion of respondents were willing to perform CPR ‘on anyone’. Of the three other studies that measured willingness to perform bystander CPR on specific groups or victims, neither a lower level of income nor level of education made a difference to survey responses. A small, New York survey 46 found no significant differences in the rates of willingness to perform hands-only CPR on a stranger, when analysed by income (p = 0.82) or education level (p = 0.16) Similarly, a small Italian survey on newly CPR-trained community members 7 found no differences in rates of willingness to perform CPR on an unknown adult (p = 0.670) or child (p = 0.661), when analysed by educational attainment. Finally, a before-and-after study evaluated a bystander CPR intervention on an island with higher levels of unemployment and low educational attainment in relation to the rest of Denmark.36,37 Although the intervention had no significant effect (p = 0.15), participants were as willing to perform CPR (chest compressions only) on a stranger before as after the intervention (85% and 87%, respectively). The reasons study respondents gave for being unwilling to provide CPR to a stranger was because they did not know how to give CPR or were afraid of doing harm. 36
Confidence to perform bystander CPR
Nine studies examined respondent’s confidence in administering bystander CPR.28,30,33,36,37,38,39,40,41,43,44 Five general population surveys reported their findings by socioeconomic status28,30,33,40,44 and provided a mixed picture regarding confidence to perform CPR, with some socioeconomic factors affecting confidence more than others. A general population survey in Ireland found no demographic differences, including social class, among the respondents who had been recently trained but still had concerns, like lack of confidence. 33 A survey in Washington, USA, 44 found level of education had no effect on confidence to administer CPR, whether trained or not. Conversely, a small survey in Spain 28 found that participants with ‘elementary [education] or no studies’ were almost three times more likely than the rest (odds ratio (OR) = 2.7; 95% confidence interval (CI): 1.4–5.5) to respond that they felt incapable of performing CPR (90.3%) (p = 0.005), but occupations were not a significant factor with regard to confidence (p = 0.05). Similarly, in a large survey in Japan, 40 working status had no effect on confidence in people’s abilities (for chest compressions, p = 0.178 or rescue breathing, p = 0.298) but household income did; those in highest income brackets were significantly more likely than those in the lowest to be confident in their ability to perform chest compressions (p = 0.045). One survey measured confidence to initiate bystander CPR on specific people – family members. 30 The large survey in Central Queensland, Australia, found that people with a lower education level and lower household income were less likely to feel confident at administering CPR to a family member if required. Confidence increased with income (from 63% on the lowest income to 85% on the highest) and level of education (from 57% with ⩽10 years to 77% with >15 years). Survey respondents with 11 or more years of education were as much as two and a half times more confident to initiate CPR if a family member collapsed than those with less education (p-values unreported for individual bands, none were < 0.05).
A qualitative study42,43 that used focus groups with residents from an economically disadvantaged, predominantly African American community in Columbus, Ohio, indicated that low confidence in one’s capability to perform bystander CPR could be caused by lack of knowledge about how and when to perform CPR and confusion caused by guidelines changing. A small survey with older respondents in a lower income, predominantly African American Florida city neighbourhood found between 16% and 20%, who had been trained in CPR did ‘not feel at all comfortable with their CPR skills’ (p. 66). 39
Finally, two training interventions targeted at increasing engagement with CPR facilitated an improvement in their confidence and capability to perform bystander CPR.36,37,38 In a post-training survey in England, more injecting drug users felt confident to undertake CPR with a person who had overdosed than before 38 and residents on a Danish island with higher unemployment and lower educational attainment than the national average had a small increase in confidence at providing CPR after training and media campaigns.36,37
Likelihood of performing bystander CPR
Two studies examined the perceived or declared likelihood of administering bystander CPR if the situation arose.33,41 In a large household survey in Queensland, Australia, 33 both employment status (p < 0.001) and education level (p < 0.001) were found to be significantly associated with the likelihood of performing bystander CPR. The article did not report the significance of individual levels of education or occupation, but proportions for declaring they were ‘extremely likely’ to perform bystander CPR ranged from those on home duties (44%) and unemployed (52%) to full-time workers (62%) and students (67%); and from those who had completed primary school (38%) to ‘trade/tech/dipl.’ (63%) education level. The same survey identified that neither employment status nor education level had a significant association with whether they were more or less likely to perform CPR on an elderly victim. In a qualitative study 41 in a low-income, predominantly Latino city neighbourhood in Colorado, a commonly cited barrier affecting residents’ likelihood of performing bystander CPR was the age and sex of the bystander being different to the victim’s. Residents also expressed that the existence of Latino and Black gangs in their own communities may make bystanders less likely to get involved in performing CPR, depending on the race of the victim involved.
Other factors influencing delivery of bystander CPR
Risk to personal health and safety
Five studies raised the issue of personal risks from performing bystander CPR.32,36,37,39,41–43 Fear of catching a disease or infection from administering mouth-to-mouth ventilation was raised by focus group participants in two qualitative studies41–43 and in one small survey, 39 all conducted in lower income, predominantly minority ethnic neighbourhoods in three US cities. Fear was also cited as a barrier to performing CPR by some survey respondents on an island with higher unemployment and lower educational attainment compared with the rest of Denmark gave for being unwilling to provide CPR to a stranger;36,37 and by participants in a household survey in Ireland who had been recently trained in CPR. 32 Two qualitative studies41–43 identified that being in a location which may place the bystander in danger, for example, at risk of being attacked or robbed was also perceived as a potential barrier to performing CPR.
Fear of legal consequences
Four studies, three from the USA, revealed that fear of legal consequences may be a barrier to bystander CPR.32,39,41–43 Two qualitative studies reported that the fear of lawsuits and legal consequences acted as a main barrier to performing bystander CPR among the participants from lower income Latino 41 and African American42,43 urban neighbourhoods. A small survey with older respondents in a lower income Florida city neighbourhood found the same, 39 as did the household survey in Ireland, for those who had been recently trained but had concerns. 32
Lack of community connectedness
Two qualitative studies found that engaging in CPR was difficult in the economically disadvantaged, predominantly African American community in Columbus, Ohio,42,43 and the predominantly Latino community in Denver, Colorado, 41 owing to a heightened lack of community connectedness. In focus groups in both cities, some residents conveyed that they did not know their neighbour or felt emotionally disconnected from them. This disconnection made them more reluctant to assist a victim in the street whom they did not know.
Cultural barriers for a specific community
A qualitative study, 41 where participants were from lower income, predominantly Latino neighbourhoods in Denver, Colorado (USA), raised additional culturally specific factors for engaging with bystander CPR in their communities. Participants feared that if they administered bystander CPR, they would be asked for identification or blamed for the victim’s condition when police and paramedics arrived on scene. Language concerns and touching someone in a way that could be perceived as inappropriate were cited as additional barriers to performing bystander CPR.
Discussion
The review identified key barriers and facilitators that impact on the ability of individuals who live in socioeconomically deprived circumstances in OECD nations to engage in bystander CPR: the willingness to learn or perform CPR; the confidence to perform CPR; and self-reported likelihood of performing CPR. Additional identified barriers and facilitators to engaging with CPR appeared to be specific for individuals from socioeconomically deprived backgrounds or areas. Few studies measured the self-reported likelihood of performing CPR.
As previously identified, 18 the findings indicate that many people in within the included study settings were willing to learn CPR, regardless of their level of education or income. However, lower community affluence or socioeconomic backgrounds of participants appeared to impact on the likelihood of individuals receiving training.19,47 Findings from some studies suggest that low levels of motivation to become trained if it is not a job requirement, unaffordability of training, or inaccessibility of training due to lack of childcare, all acted as barriers with their study contexts.41–43 The review identified that individuals’ confidence in their ability to perform bystander CPR was mixed. Some measures of socioeconomic status appear to affect confidence levels more than others. Overall, populations with low education or household income levels appear to have low confidence in administering CPR to either a family member or a stranger. This review revealed other barriers to engaging with CPR: the risk to personal health linked to the environment, a fear of legal consequences, a lack of community cohesion, and a number of cultural barriers. Moreover, in some of the deprived communities that were studied in this review, there was a perception potential risk to bystanders’ safety from helping victims in situations where they themselves could be robbed or attacked.
Since the systematic search for studies in December 2017 and the results were synthesised, two relevant studies have been published. (The search strategy was rerun in Medline only, in August 2020.) A cross-sectional survey of public gatherings in Baltimore, USA, 48 found that those from the high-poverty areas (27% of all respondents) preferred instructor-led CPR training and that most disliked the idea of training occurring at a local learning station (at events or in shops) and preferred libraries. Non-college graduates (46% of all respondents) preferred school settings as well as instructor-led education. The survey found that preferences for training locations and formats were comparable across all respondents. A small prospective survey by the same authors conducted before and after free community compression-only CPR classes in Baltimore 49 found that a lower level of education (29% of all respondents) increased the likelihood that participants feared being sued or risk of disease or hurting someone and were unlikely to perform CPR on strangers or family, even after training. Household income was not found to affect the likelihood of performing CPR. Neither of these studies substantially alter our results.
The findings from this review have a number of implications for the development of interventions aimed at improving bystander CPR in deprived communities. Although such populations show a willingness to learn CPR, they are often among the least trained in CPR. Therefore, interventions to support bystander CPR must make training more flexible, affordable, and accessible to people in deprived communities. More education needs to occur and to be targeted at deprived communities focusing not only the practical skills to give bystander CPR but also the confidence that anyone may be ‘CPR ready’ and capable to give bystander CPR, even if they are weaker or disabled, or at least that they may be able to give help. The findings of this review informed the analysis of a qualitative research study on bystander CPR with deprived communities in Scotland which identified similar individual and environmental barriers to be targeted through tailored interventions. 50
Limitations
A key limitation of the review’s method was the range of proxy socio-demographic indicators used for signifying a socially or economically disadvantaged community. Some of the included studies were unambiguously conducted with people living in deprived circumstances. Other studies employed single indicators like low educational attainment or large geographic areas where employment status and incomes were averaged across all residents are more uncertain for labelling the respondents as living in deprived circumstances. Other limitations include the potential for introducing reviewer bias and missing relevant studies by single-screening at the ‘fast screening’ stage, as none of the papers excluded were double-checked. Few of the included studies’ main aims were to identify barriers and facilitators of bystander CPR in deprived communities. Many of the included (and excluded) surveys collected barriers and facilitators data but did not analyse all outcome measures by socio-demographics. Finally, thresholds for deprivation may not be defined in the same way across countries. This had an impact on the way the studies presented their results and made it difficult to compare findings.
Conclusion
This review suggests that people living in deprived communities in different contexts face significant and specific barriers to becoming ‘CPR ready’. Tailored interventions for deprived communities are required to increase engagement with bystander CPR, including information and awareness raising (through context-specific and community-led social marketing campaigns) and more innovative and accessible CPR training (through peer and social network interventions, online, shorter and cheaper CPR training, support for childcare, and transport costs).
Supplemental Material
sj-docx-1-rsh-10.1177_17579139211055497 – Supplemental material for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review
Supplemental material, sj-docx-1-rsh-10.1177_17579139211055497 for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review by I Uny, K Angus, E Duncan and F Dobbie in Perspectives in Public Health
Supplemental Material
sj-docx-2-rsh-10.1177_17579139211055497 – Supplemental material for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review
Supplemental material, sj-docx-2-rsh-10.1177_17579139211055497 for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review by I Uny, K Angus, E Duncan and F Dobbie in Perspectives in Public Health
Supplemental Material
sj-docx-3-rsh-10.1177_17579139211055497 – Supplemental material for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review
Supplemental material, sj-docx-3-rsh-10.1177_17579139211055497 for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review by I Uny, K Angus, E Duncan and F Dobbie in Perspectives in Public Health
Supplemental Material
sj-docx-4-rsh-10.1177_17579139211055497 – Supplemental material for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review
Supplemental material, sj-docx-4-rsh-10.1177_17579139211055497 for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review by I Uny, K Angus, E Duncan and F Dobbie in Perspectives in Public Health
Supplemental Material
sj-docx-5-rsh-10.1177_17579139211055497 – Supplemental material for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review
Supplemental material, sj-docx-5-rsh-10.1177_17579139211055497 for Barriers and facilitators to delivering bystander cardiopulmonary resuscitation in deprived communities: a systematic review by I Uny, K Angus, E Duncan and F Dobbie in Perspectives in Public Health
Footnotes
Acknowledgements
Our thanks to Anne Marie MacKintosh (ISMH) for assistance with interpreting some of the studies’ statistical data and to the advisory group for sharing relevant papers. We acknowledge members of the wider study for their support: Martine Stead, Douglas Eadie, and Nathan Critchlow (ISMH, University of Stirling), and Gareth Clegg, Liz Hasseld, and Lisa MacInnes (Resuscitation Research Group, University of Edinburgh).
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The systematic review was conducted as part of a project funded by the Chief Scientist Office HIPS /17/10. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The corresponding author had final responsibility for the decision to submit for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.