
Abstract
Background
Dispatcher assistance can help to save lives during layperson cardiopulmonary resuscitation during cardiac arrest. The aim of this study was to investigate the influence of different camera positions on the evaluation of cardiopulmonary resuscitation performance during video-assisted cardiopulmonary resuscitation.
Methods
For this randomized, controlled simulation trial, seven video sequences of cardiopulmonary resuscitation performance were recorded from three different camera positions: side, foot and head position. Video sequences showed either correct cardiopulmonary resuscitation performance or one of the six typical errors: low and high compression rate, superficial and increased compression depth, wrong hand position or incomplete release. Video sequences with different cardiopulmonary resuscitation performances and camera positions were randomly combined such that each evaluator was presented seven individual combinations of cardiopulmonary resuscitation and camera position and evaluated each cardiopulmonary resuscitation performance once. A total of 46 paramedics and 47 emergency physicians evaluated seven video sequences of cardiopulmonary resuscitation performance from different camera positions. The primary hypothesis was that there are differences in accuracy of correct assessment/error recognition depending on camera perspective. Generalized linear multi-level analyses assuming a binomial distribution and a logit link were employed to account for the dependency between each evaluator's seven ratings.
Results
Of 651 video sequences, cardiopulmonary resuscitation performance was evaluable in 96.8% and correctly evaluated in 74.5% over all camera positions. Cardiopulmonary resuscitation performance was classified correctly from a side perspective in 81.3%, from a foot perspective in 68.8% and from a head perspective in 73.6%, revealing a significant difference in error recognition depending on the camera perspective (p = .01). Correct cardiopulmonary resuscitation was mistakenly evaluated to be false in 46.2% over all perspectives.
Conclusions
Participants were able to recognize significantly more mistakes when the camera was located on the opposite side of the cardiopulmonary resuscitation provider. Foot position should be avoided in order to enable the dispatcher the best possible view to evaluating cardiopulmonary resuscitation quality.
Keywords
Sudden cardiac arrest (SCA) is responsible for about half of all deaths from cardiovascular disease, 1 which makes it one of the leading causes of death in industrialized countries1–4 It has been identified that immediate bystander cardiopulmonary resuscitation (CPR) can significantly improve survival from SCA,5,6 while only waiting for the emergency medical services (EMS) to arrive without bystander CPR leads to severe neurological impairment or death in up to 92%.3,5
Unfortunately, most bystanders who call the emergency services are laypersons, for whom the identification of cardiac arrest may be difficult due to residual brain stem reflexes. Moreover, they may often also be emotionally distraught when witnessing an emergency of a family member, relative or friend. 7 Thus, EMS dispatchers play a substantial role to help bystanders identify cardiac arrest, and to instruct bystanders to initiate CPR efforts by phone, also known as telephone-CPR (T-CPR). 8 T-CPR is associated with better survival, 9 and is thus strongly endorsed by international CPR guidelines. 10
Video-assisted CPR (V-CPR) is a relatively new technology that enables the EMS dispatcher not only to hear the depiction of the scene, but also to see the video footage from a smartphone's camera.11,12 This can both help to better recognize the nature and severity of an emergency, and to support and correct basic life support. 12 For decades attempts for implementing this technology have been made and newer randomized, controlled trials with contemporary technology have clearly demonstrated that V-CPR can lead to a more accurate compression depth than T-CPR, and that both V-CPR and T-CPR lead to better resuscitation quality compared to unassisted CPR. 13 However, video resolutions and framerates of the video have varied widely in these studies, making the results difficult to compare – this may be an explanation of varying results concerning the usefulness of V-CPR. 14 Surprisingly, little to no attention has been paid to the position of the camera. To the best of the author’s knowledge, there is no study about the influence of the camera position on V-CPR.
This study aims to analyze the influence of different camera perspectives in relation to the patient in need of CPR, regarding the percentage of recognition of standardized problems that may lead to insufficient CPR in real life.
Materials and methods
Study design
This randomized, controlled simulation trial was conducted in the University Hospital of Cologne and the EMS Department of the Fire Brigade of Kerpen, Germany.
Ethics
The study was approved by the Ethics Committee of the University Hospital Cologne (Approval no. 18-130, February 12, 2019; Chairperson: Prof. Dr R. Voltz) and was registered at the German Clinical Trial Register (Registration no. DRKS00015297) prior to beginning. Data were collected from September 2019 to February 2020. Written and informed consent was obtained from each participant prior to inclusion.
Materials
CPR was simulated using a standardized CPR training manikin (Ambu Man, Ambu GmbH, Bad Nauheim, Germany). Beforehand, video sequences showing one-helper compression-only CPR were recorded at the Skills Lab (i.e. the simulation hospital) of the University Hospital of Cologne, to standardize conditions and eliminate environmental influences. Video sequences were recorded with a Tamron objective (Tamron SP 24–70 mm F/2.8, Tamron Corporation, Saitama, Japan) on a Nikon D750 (Nikon Corporation, Tokyo, Japan) with a resolution of 1920 × 1080 pixels per inch and 30 frames per second, to obtain a video with maximum quality and exclude influences on evaluation that might result from lower resolution videos.
The camera was placed on a tripod (height 140 cm, which represents the height in which a typical male adult would hold a smartphone to take a video), and video sequences were recorded sequentially from three different positions: side perspective (camera position laterally from the manikin, on the opposite side of the helper), foot perspective (camera position at the feet end of the manikin) and head perspective (camera installed at the head side of the manikin), as shown in Figure 1. Distances from camera position to the scene were chosen in a way that both helper's head, arms (in full length) and manikin's torso were fully visible in the video.
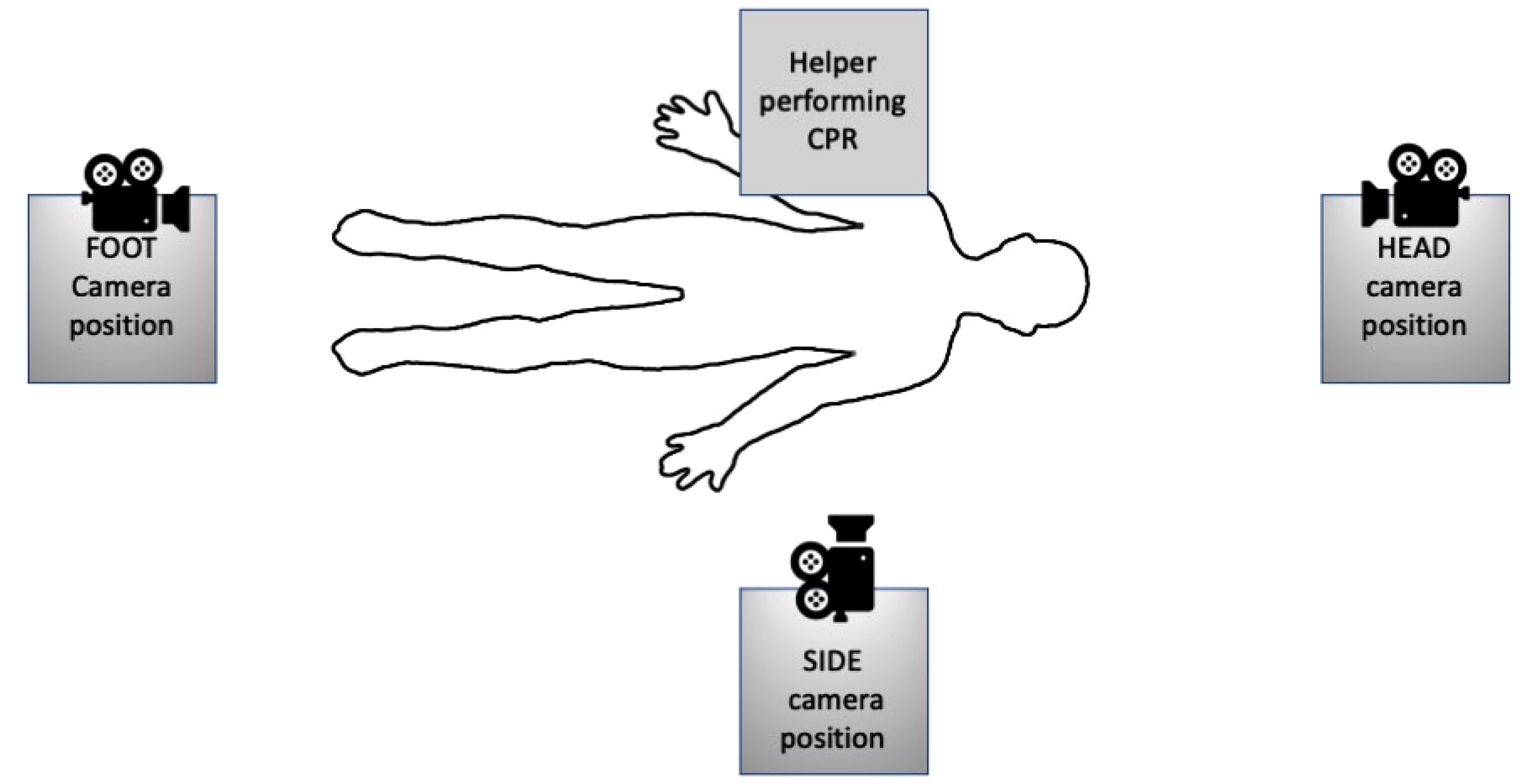
Setup of the simulation setting, showing the positions of a manikin, cardiopulmonary resuscitation (CPR) provider, and the three camera positions (“foot”, “head,” and “side”).
A metronome (Metronom Beats App, Stonekick, London, UK; downloaded from Google Play Store) was set to 110 bpm to ensure guideline-conformant compression frequency, and the internal compression depth indicator of the manikin was used to ensure sufficient compression depth. Videos were recorded repeatedly until the desired conditions were exactly fulfilled. In the final video sequences, neither metronome nor compression depth indicator was visible respectively audible. Seven high-quality video clips of 12 s each from every perspective were recorded sequentially, showing either guideline-conformant compression-only CPR, or a typical error made often during CPR (Table 1). The same person performed CPR in all clips; typical errors were deliberately implemented in the videos. The 12 s were chosen to give a sufficient number of compressions to be evaluated (guideline-conformant frequency of 100–120 min−1 would allow to observe 20–24 chest compressions), and to give a certain time constraint.
CPR parameters and errors shown in the video sequences.
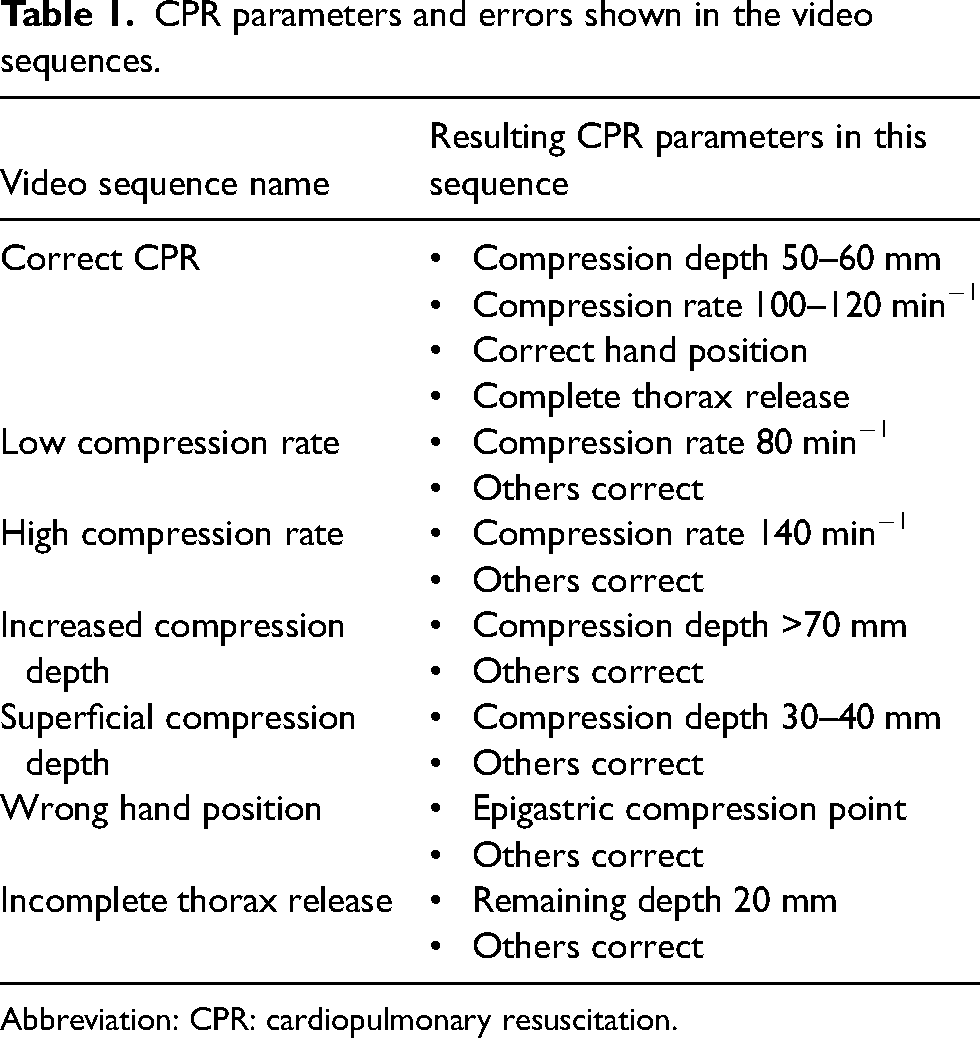
Abbreviation: CPR: cardiopulmonary resuscitation.
Video sequences were randomized regarding CPR errors and perspectives with a randomization algorithm provided by the Institute of Medical Statistics and Computational Biology (IMSB) of the University of Cologne as described below. During the evaluation phase, every study participant evaluated seven video sequences on a 15.6″ laptop (ASUS, Taipeh, Taiwan). A standardized questionnaire with multiple-choice answers was used to evaluate CPR quality.
Study protocol
There were no primary exclusion criteria. Each participant was asked to view video sequences alone in a room with the supervisor. Participants were recruited from the staff of the Fire Department of Kerpen, Germany, and consisted of paramedics (trained as dispatchers) and emergency physicians. They were consecutively shown seven video sequences of one-helper compression-only CPR, and were asked to evaluate CPR performance after each video sequence, using a standardized questionnaire with multiple-choice answers about compression rate, compression depth, compression point, and release after compression. The video was only shown once in full length (12 s), repeating was not allowed. As shown in Table 1, only one single CPR parameter was altered in each video sequence. However, participants were not explicitly informed about the number of mistakes per video sequence and, thus, an indication of more (allegedly) mistakes was possible.
Further, we formed four categories in which the seven CPR performances were assorted for statistical analysis (see Table 1): “compression rate” (low and high compression rate), “compression depth” (low and high compression depth), “hand position,” and “thorax release.”
During the evaluation process, evaluators had the possibility to indicate each category as “not evaluable.” There was no time limit for answering the questionnaire.
Measurements and outcomes
The primary outcome parameter was the correct
Secondary outcome parameters consisted of:
classification of CPR performance depending on the presented error, false classification of correct CPR performance, frequencies of CPR performances evaluated as “impossible to evaluate,” comparison of results between paramedics and emergency physicians.
Statistical analysis
The primary hypothesis of this study was that correct assessment/error recognition depends on the camera perspective. The required sample size was calculated in order to achieve 80% power at a significance level of 5% to detect a minimal difference in the percentage of error recognition between different perspectives of 25%, that is, assuming a detection rate of 95 versus 70%. Sample size calculation was accounted for (a) the dependency of the seven ratings conducted by the same evaluator by assuming an intra-class correlation coefficient of 0.8 and (b) a drop-out rate of 10%. When recruiting a total of 100 evaluators, the actual power of a χ2 test to detect a difference in proportions of 25% was estimated as 81% (SAS 9.3, Cary, North Carolina, USA).
Each evaluator had to judge seven video sequences. Six of those included the six different error types, while only one error type was included per video sequence (see Table 1). Furthermore, one of those seven video sequences did not comprise any error. Separately for each evaluator, perspectives were randomly assigned to video sequences with the seven different CPR performances, so that each evaluator had to judge each CPR performance once and each perspective at least twice. Note that, for example, evaluator “A” may have to judge a certain CPR performance from side camera position whereas evaluator “B” may have to judge the same CPR performance from a foot perspective. For random assignment of CPR performances and perspectives, the software “R” (The R Foundation for Statistical Computing, Vienna, Austria) was employed.
Descriptive analyses present numbers and percentages for categorical variables. Generalized linear multi-level analyses assuming a binomial distribution and a logit link were employed to account for the dependency between each evaluator's seven ratings (random intercept). In our primary analyses (model 1) we modelled the association between perspective (foot/head/side (reference); fixed effect) and correct assessment of CPR performance (yes = 1/no = 0; outcome) adjusted for a profession (paramedic, emergency physician (reference)), and error type/correct performance (reference). To investigate the primary hypothesis, based on model 1, an overall post-hoc test was performed to investigate whether a correct assessment of CPR performance differs by perspective. Subsequent pairwise comparisons of estimated marginal means between perspectives were adjusted according to Bonferroni-Holm.
Logistic regression analyses were run to perform subgroup analyses by error type and correct CPR performance, respectively (model 2; outcome: correct assessment of CPR performance, independent variables: perspective, profession).
To investigate whether the influence of perspective on a correct assessment of CPR performance differs by profession an interaction term (perspective × profession) was added to model 1 as well as to model 2 (to investigate the interaction separately for each error type/correct performance).
Additional generalized linear multi-level analyses were run for the outcomes “CPR quality not evaluable” (yes/no; fixed effects: perspective, profession, error type; model 3) and further mistakes (yes/no; fixed effects: perspective, profession, error type; model 4).
Missing data were not imputed.
Regarding our primary hypothesis, a p value <.05 was regarded as statistically significant.
The secondary results of our subgroup analyses were considered exploratory and not interpreted with respect to statistical significance.
Statistical computations were carried out using IBM SPSS Statistics (Version 26.0.0.1, 64-bit version; IBM Inc., Armonk, NY, USA).
Results
A total of 46 paramedics (all of them actively working and all also trained as EMS dispatchers) and 47 emergency physicians (all of them actively working, but without dispatching experience) were randomly recruited from staff of the EMS Department of the Fire Brigade of Kerpen, Germany, and the University Hospital of Cologne, Germany. Neither of the participants was experienced in evaluating CPR from a video sequence, nor had used V-CPR before. Each participant evaluated seven video sequences, showing guideline-conformant CPR or a typical mistake during CPR, from three different perspectives.
In total, 93 participants observed and evaluated 651 videos (322 videos by 46 paramedics and 329 videos by 47 emergency physicians, as shown in Figure 2).
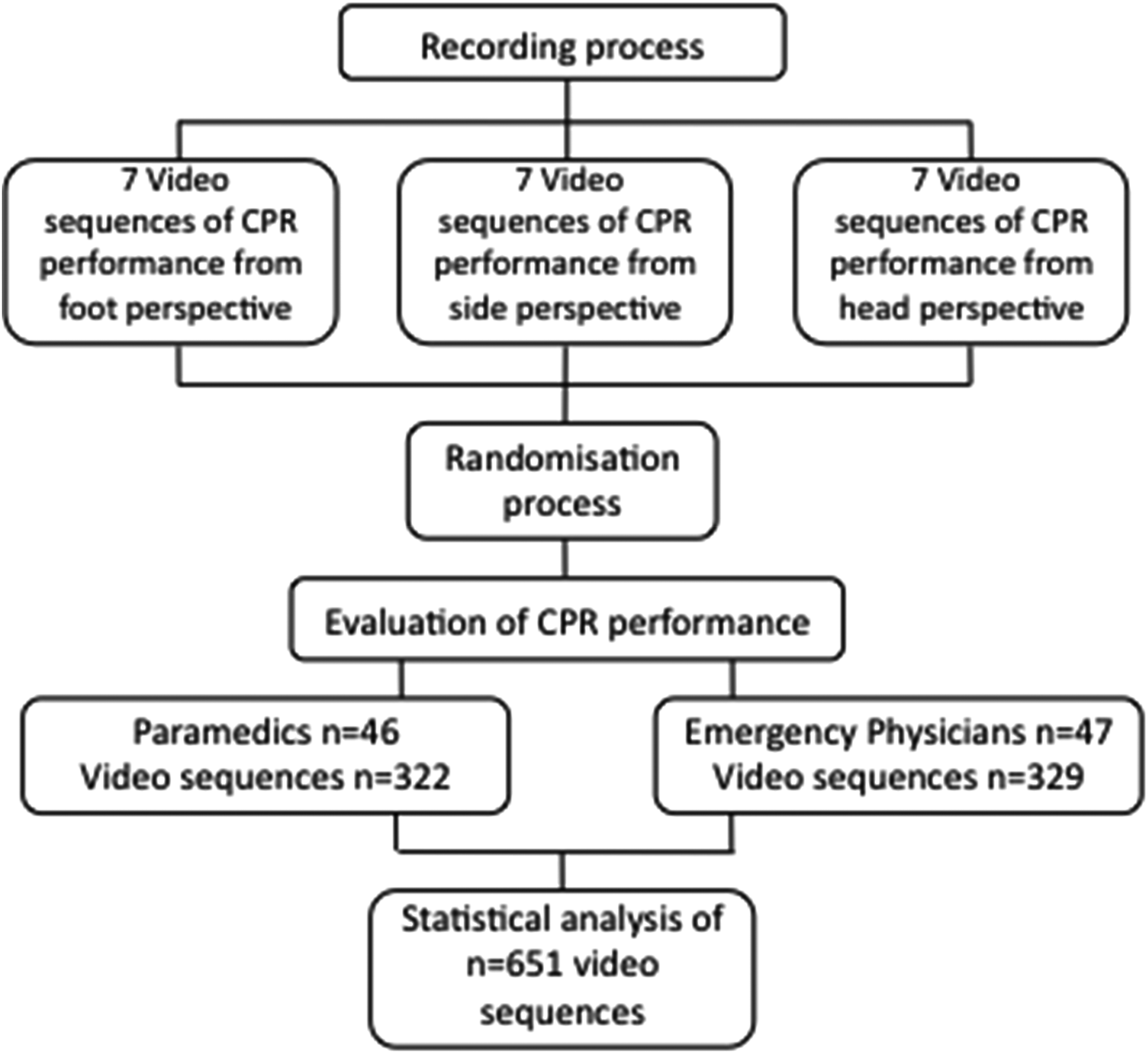
Study flowchart. During the recording process, seven video sequences of cardiopulmonary resuscitation (CPR) from three different camera positions were recorded. Each evaluator (paramedic or emergency physician) had to judge seven video sequences, whereby CPR performances and camera positions had been randomly combined during the randomization process.
Classification of CPR performance depending on camera perspective
Errors presented in the video sequences were overall evaluated correctly in 74.5% (Figure 3). Overall, perspective had a significant influence on whether CPR performance was correctly assessed (p < .001).
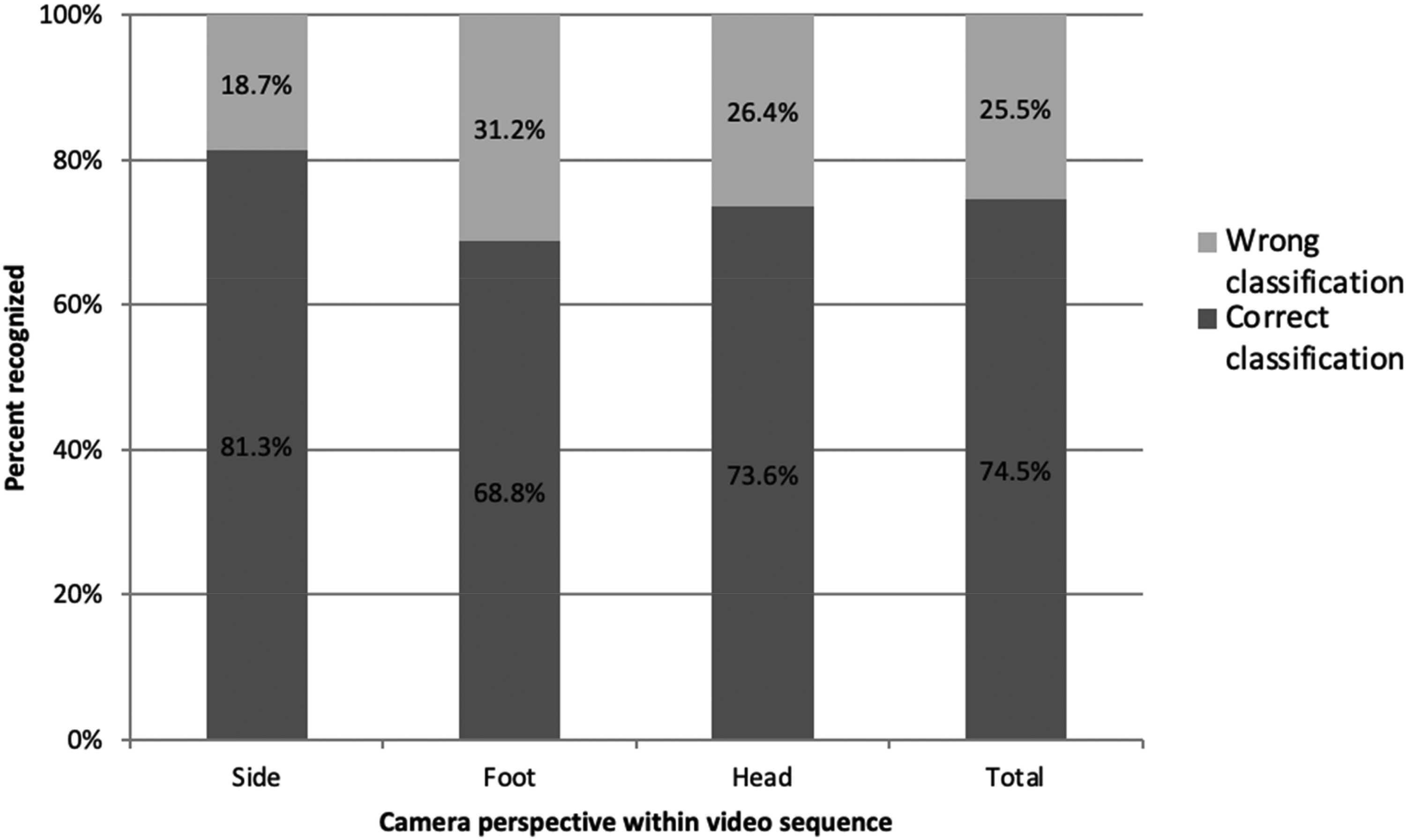
Classification of cardiopulmonary resuscitation (CPR) performance in video sequences from different camera perspectives (n = 651).
From a side perspective, CPR performance was classified correctly in 81.3%, whereas from a foot perspective CPR was correctly evaluated in 68.8% and from a head perspective in 73.6%.
Pairwise post-hoc tests reveal significant differences between side and foot perspective (Bonferroni-Holm adjusted p value = .011) as well as between side and head perspective (Bonferroni-Holm adjusted p value = .014). Corresponding odds ratios (OR) indicate a better performance in terms of correct assessment from a side perspective (OR (foot vs. side) = 0.43 (95% confidence interval (CI) = 0.26–0.74); OR (head vs. side) = 0.45 (95% CI = 0.26–0.78)). No significant difference was observed for head versus foot perspective (Bonferroni-Holm adjusted p value = .864).
Figure 4 shows the results of subgroup analyses comparing CPR performance classifications (correct/incorrect) between camera perspectives by recorded error type. Differences between different camera perspectives were found for the identification of only two CPR types: correct CPR performance and incomplete thorax release.
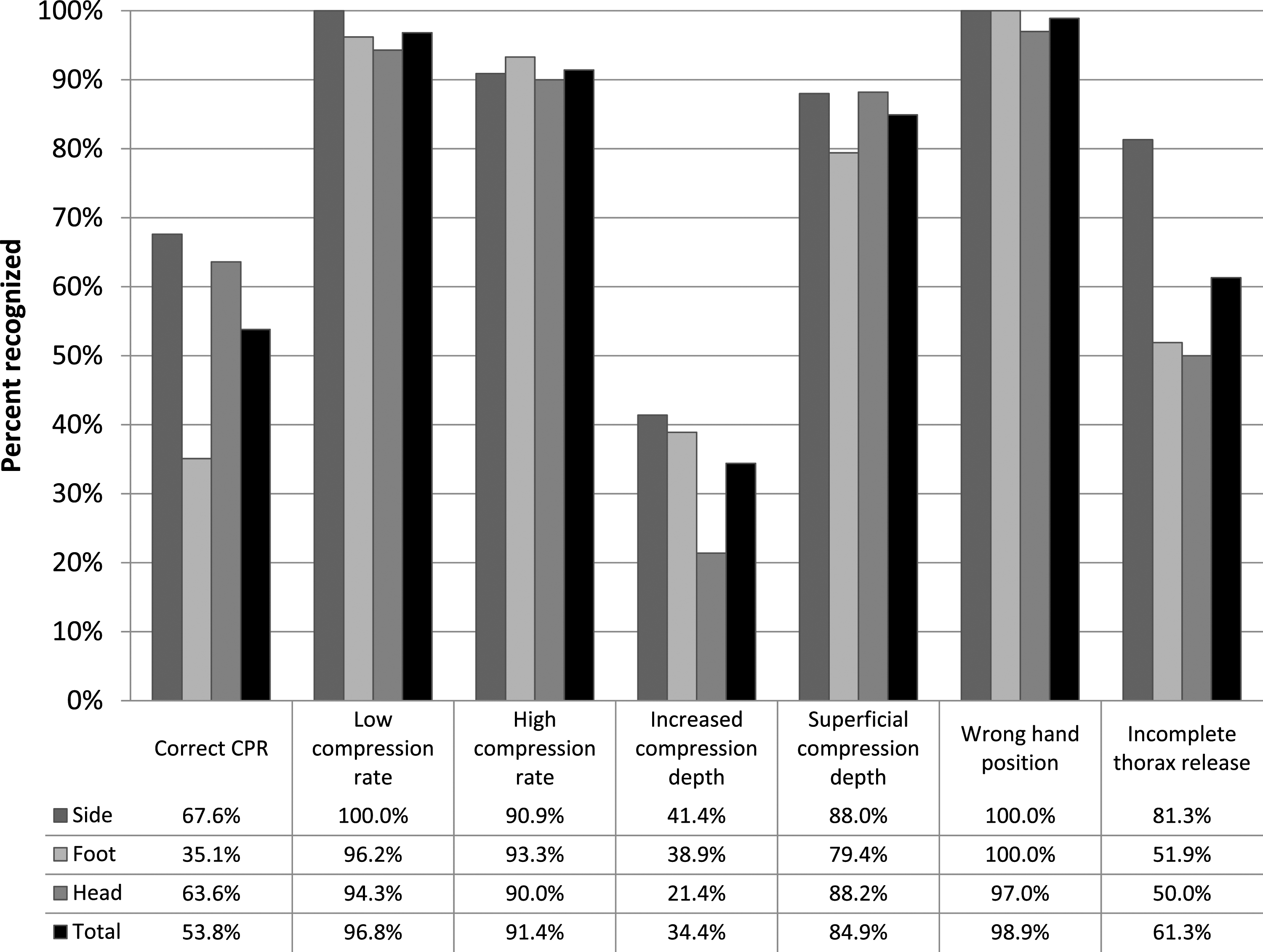
Correct classification of mistakes during cardiopulmonary resuscitation (CPR), depending on different camera perspectives (n = 651).
For correct CPR, there was a noticeable association between perspective and correct assessment (p = .018), head versus side: p = .749, OR = 0.83 (95% CI = 0.27–2.57), foot versus side: p = .008, OR = 0.25 (95% CI = 0.09–0.70), showing a better assessment from side compared to a foot perspective.
In regard to incomplete thorax release, there was a significant association between perspective and correct assessment (p = .025), head versus side: p = .013, OR = 0.24 (95%CI = 0.08–0.74), foot versus side: p = .019, OR = 0.25 (95% CI = 0.08–0.80), also indicating a better assessment from a side perspective.
False classification of correct CPR
Over all camera perspectives, correctly performed CPR was falsely classified in 46.2%. For the falsely classified video sequences with correct CPR, Figure 5 shows the frequency of the different attributed errors.
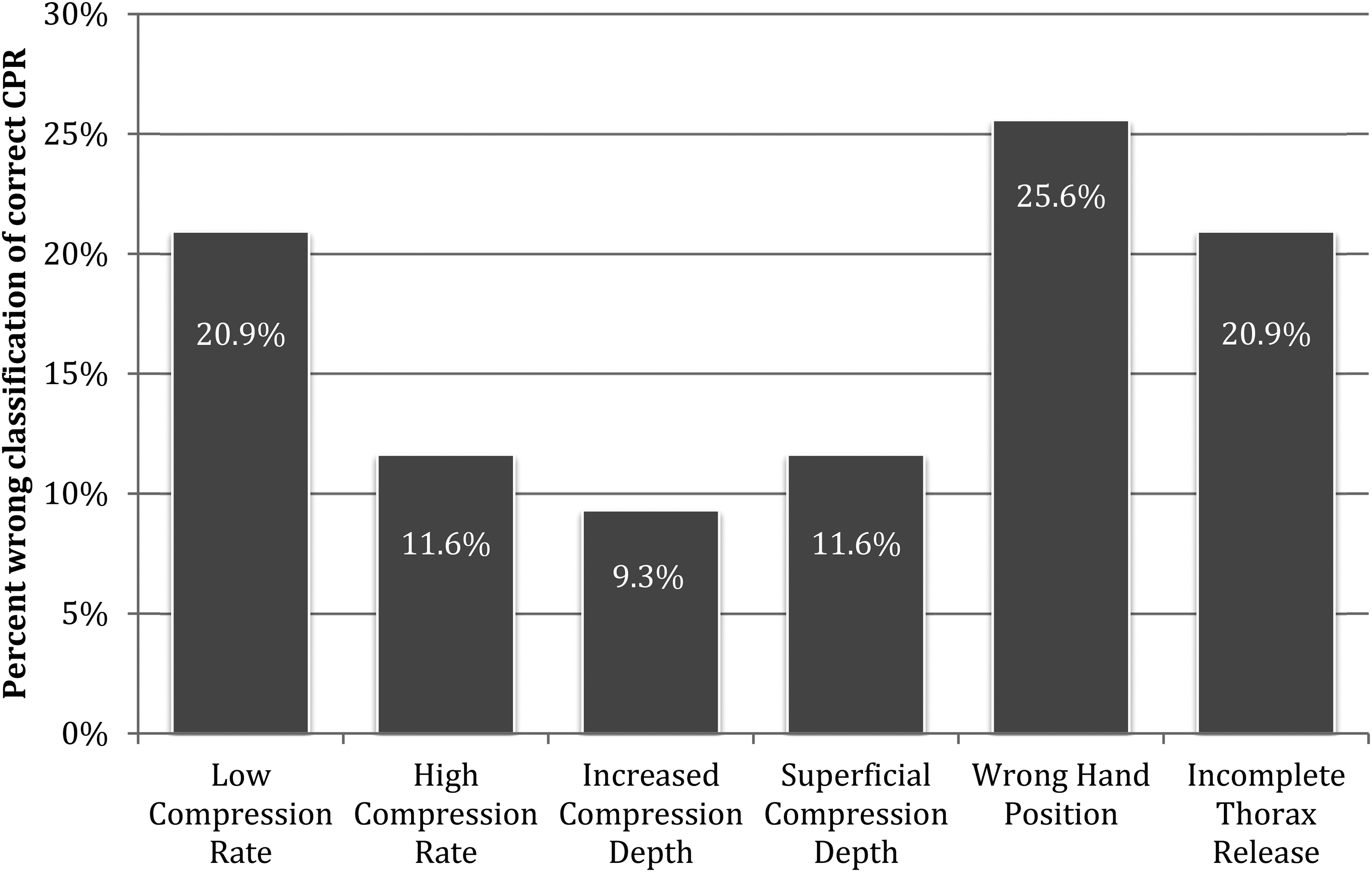
False classification of correct cardiopulmonary resuscitation (CPR) over all video sequences (n = 651).
Frequencies of CPR quality not evaluable
In 21 of 651 video sequences (3.2%) a CPR category was marked as “not evaluable.” From a side perspective, evaluators indicated a CPR category to be not evaluable in three video sequences (0.4%), from a foot perspective in 12 video sequences (1.8%) and from a head perspective in six video sequences (0.9%). There was no noticeable difference depending on the camera perspective (p = .829).
Comparison of results between paramedics and emergency physicians
This study was not powered to find differences in the evaluation between paramedics and emergency physicians. However, our results reveal some interesting findings regarding inter-professional differences between these two groups. Summarizing all video perspectives, correct classification of the presented errors was achieved in 76.4% for paramedics and in 72.6% for emergency physicians, showing no significant inter-professional difference (p = .282). When analyzing the results of emergency physicians and paramedics separately, there was no significant difference in error classification depending on the camera perspective. However, there was a significant influence of the camera perspective on the correct classification of incomplete thorax release when evaluated by emergency physicians. For this specific error, from a side perspective, 85.7% were identified correctly, whereas only 50% were correctly identified from a foot perspective, and 42.9% from a head perspective (p = .03). Finally, there was no inter-professional difference regarding indicating “mistake unassessable” (p = .735) and indicating further mistakes (p = .319).
Discussion
This is the first study to evaluate the impact of the camera position on the evaluation of a video showing CPR. Our main finding was that CPR could significantly be better interpreted from the side, and comparable from the head side, whereas evaluation from the foot side was inferior. Interestingly, we observed that correct CPR was disproportionately often evaluated as “wrong CPR.”
In general, we found that evaluation of a video CPR sequence was feasible in 96.8%.
Our data show that significantly more resuscitation errors were identified from the side perspective than from the foot perspective. However, there was no significant difference in the side perspective compared to the head perspective. The side perspective showed statistical superiority regarding the identification of incomplete thorax release compared to the other two camera perspectives (head and foot). Interestingly, the side perspective also showed statistically noticeable results regarding the recognition of correct CPR compared to the foot and head perspective. However, our study could not find statistically noticeable differences between the different camera perspectives concerning low or high compression rate, increased compression depth, superficial compression depth or wrong hand position.
Interestingly, participants did not recognize “correct” CPR very well, in comparison to the “wrong” CPR sequences. We assume that this might be attributable to the fact that the last guidelines had a strong focus towards “push harder and faster.” Furthermore, some kind of Hawthorne effect cannot be excluded; the fact that we showed them videos and asked them to find mistakes therein may have made them “hyper-vigilant.”
V-CPR has been scarcely reported in only a few studies that describe the potential value of video communication with emergency services, for example, during cardiac arrest.11–17 In these simulation studies, dispatchers were enabled to assist during CPR and to give instructions based on the visual information they receive from the scene of the incident—a technique that has become known as Video-CPR (V-CPR). Newer studies showed advantages and some superiority of V-CPR over T-CPR concerning the CPR quality. 18 Since the terms “V-CPR” and “video assisted CPR” are not limited to live video connection from a dispatcher to a CPR provider, we could identify only seven studies investigating V-CPR in this context.11–17 Three of these studies were conducted nearly a decade ago,11,14,16 while three studies were published in 2020.13,15,17 In summary, none of these studies report the exact camera position, nor was the camera position standardized in any of them. To the best of the author’s knowledge, camera position during V-CPR has not been investigated and reported yet.
All of these studies used different video devices, generally the best technology available to them at the time. However, smartphone technology is rapidly evolving as we all know, and better video quality in video calls is to be expected with every new smartphone generation. Furthermore, the study designs and study settings of the above-mentioned studies were heterogeneous. Irrespective of differences in the group of participants (e.g. students, layperson, etc.) and dispatchers (e.g. medical students, nurses, EMS dispatchers), V-CPR was always performed on a training manikin, except for one study from South Korea, 17 where it was performed in real pre-hospital emergencies. Results, in regard to their effectiveness to CPR, of all these studies show high variance.
As in most of the cases in real-life situations, a camera tripod will most certainly not be available, and the feasibility of V-CPR may be limited. Thus, the availability of a direct line of sight depends on a second bystander or a fixed point to mount the camera.
Thereby, a compromise needs to be found between installing video connection and time without chest compressions. So far, the use of V-CPR stays rare and requires—in case of use in a real CPR setting—a certain amount of flexibility and ingenuity. Nevertheless, there is a need for standardized V-CPR protocols, comparable to T-CPR protocols, for the future use of V-CPR in real-life situations.
Taken together, the results of the present study are encouraging for V-CPR, as resuscitation errors were correctly classified in over 70% of the cases regardless of the camera perspective. From our results, we conclude that the perspective of the camera is important and has to be specified, as it may have a significant impact on the viewer's ability to correctly assess the CPR quality shown in the video. From our results, we can recommend that the camera position should be on the opposite side of the helper, or at the head of the patient, but not at the foot side.
Limitations
This study was conducted with a resuscitation manikin made for education and evaluation of medical personal, which is only a substitute for real patients. In accordance with the current ERC guidelines, we are confined to a compression-only CPR approach. Future studies might incorporate ventilation in their CPR scenario. All participating paramedics were also experienced as EMS dispatchers, but the emergency physicians were not, as this is not part of their regular duty in Germany. It must be kept in mind that our study was conducted with a collective of individuals who did not have specific V-CPR training. Results might be even better in a trained collective.
In this study, we evaluated only three camera angles on a CPR situation. Of course, numerous more possible camera angles might be superior or inferior to the ones we investigated in this study. Apart from that, further studies should take into account the influence of the camera position, and thus should report the camera angle to ensure valid and comparable results.
Video footage was recorded in a closed environment with sufficient light, constant weather, no disturbances, and perfect technical facilities (e.g. tripod), and with a high (full HD) resolution. Further evaluation with different video resolutions and environments is necessary before the implementation of this technology.
Conclusion
During V-CPR, the camera position had a significant impact on the ability of a dispatcher to correctly evaluate a CPR performance. Dispatchers were able to recognize significantly more mistakes when the camera was located on the opposite side of the CPR provider. From the head position, results were comparable, but from a foot position, significantly fewer mistakes could be identified. Hence, foot position should be avoided in order to enable the dispatcher the best possible view to evaluating CPR quality.
Footnotes
Acknowledgements
This study was supported by the ERC Research NET.
Declaration of conflicting interests
Bernd W. Böttiger is European Resuscitation Council (ERC) Board Director Science and Research; Chairman of the German Resuscitation Council (GRC); Member of the Advanced Life Support (ALS) Task Force of the International Liaison Committee on Resuscitation (ILCOR); Member of the executive committee of the German Interdisciplinary Association for Intensive and Emergency Medicine (DIVI); Associated Editor of the European Journal of Anaesthesiology (EJA), Co-Editor of “Resuscitation”; Editor of the Journal “Notfall + Rettungsmedizin.” He received professional fees for lectures from the following companies: “Forum für medizinische Fortbildung (FomF),” ZOLL Medical Deutschland GmbH, C. R. Bard GmbH, GS Elektromedizinische Geräte G. Stemple GmbH. The other authors do not have a conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.