
Abstract
This quantitative comparative study was conducted to examine if, and to what extent, differences in health and functioning and quality of life exist for community college students who complete an academic mindfulness course. Surveyed student responses were captured by the Quality of Life Index (QLI) (Ferrans and Powers, 1985), dependent variables measured, and a non-directional two-tailed independent (unpaired) samples t test conducted. A univariate post-test only comparison group design was conducted to measure results of the mindfulness coursework intervention at the conclusion of the courses. A non-probability convenience sampling of 154 participants was collected, with both descriptive and inferential statics calculated. Data results indicated a statistically significant difference in health and functioning between the comparison and the intervention groups as well as quality of life between the comparison and the intervention groups. Effect size (Cohen’s d) at a 95% confidence interval for those students who completed a mindfulness course was large for the overall QLI score as well as the health and functioning subscale. This study demonstrated positive results and statistical significance suggesting the utility of mindfulness coursework. Recommendations from this study include integrating mindfulness coursework in a classroom setting and offering mindfulness training as a stand-alone academic course.
Introduction
Mindfulness has become an increasingly popular tool for stress management, whole person health and wellness, and behavioral and lifestyle modifications. Integration of Eastern holistic and complementary interventions into Western medicine have bolstered the popularity of mindfulness as a mainstream ideology. Practical application and measuring outcomes of mindfulness practices remains under review as a valid and reliable medical intervention (Park et al., 2020). Studying the difference in an individual’s quality of life and health and functioning because of mindfulness training will help identify the efficacy of integrating mindfulness practices and training into academic coursework and social interventions. The problem is the plethora of anecdotal support for the utility of mindfulness training without a large representation of research-based evidence. Therefore, the purpose of this quantitative comparative study was to examine if mindfulness coursework has an impact on an individual’s perception of overall well-being, health and wellness. Two research questions were investigated through a survey of community college students in the Southwestern United States: “to what extent, if any, was there a difference in health and functioning for students based upon completion of mindfulness coursework,” and “to what extent, if any, was there a difference in quality of life for students based upon completion of mindfulness coursework.” The null hypotheses were that a statistically significant difference did not exist between the comparison and intervention groups for the two research questions, whereas the alternate hypotheses were that a statistically significant difference did exist.
Literature review
Mindfulness Theory posits being present and aware in the very moment, without distraction of the past or future (Langer, 1989). The practice and awareness of mindfulness has grown in social and research popularity, such as in an educational environment (Emerson et al., 2020) and even metacognition (Reina and Kudesia, 2020) as a potential benefit to improving lifestyle through behavior modification and as a supplement to conventional medicinal and therapeutic modalities. Mindfulness is the process by which attention is brought to the present moment, removing an individual’s fleeting thoughts and mental preoccupation with extrinsic stressors and worldly concerns and allows for attention to be placed on more personal needs and feelings (Kabat-Zinn, 1990).
Theoretical foundations
The Health Belief Model (HBM) focuses on an explanation of preventive health behavior (Rosenstock, 1974). Health behavior is defined as activity undertaken by an individual who believes they are healthy for the purpose of preventing disease and differs from illness behavior which is activity undertaken when a person feels ill for the purpose of discovering a suitable remedy and sick-role behavior which is activity demonstrated when a person considers themselves ill for the purpose of getting well (Kasl and Cobb, 1966). Understanding the three models of behavior is important as the HBM supports changing lifestyles and behaviors to impact health through self-efficacy and belief in outcomes (Rosenstock, 1974) and promotes the inquiry of dispositional mindfulness and total quality of life and improved human health and functioning as a result of increased trait mindfulness.
Complementary and alternative medicine
Recent exploration into complementary and alternative medicine (CAM) has demonstrated how lack of coping strategies and healthy lifestyle practices negatively impacts quality of life for cardiovascular patients (Somayeh et al., 2015). This research suggests non-pharmacological treatment options, including bringing the focus of mindfulness and CAM into the practice of self-care regimens for therapists, counselors, and teachers (Tsang et al., 2015). The focus of CAM evolved from patient self-management to practitioner self-care and ultimately sought to impact the value of mindfulness practices in the academic setting (Chulguen and Goralski, 2016; McConville et al., 2017).
Mindfulness in an academic setting
As mindfulness is evolving into more of a household word and garners commercial and media attention, the expressed interest in sharing formal mindfulness practices for community benefit has increased. Some research has suggested efficacy of mindfulness training in an academic setting and touched upon the need for expanded research to explore the relevance of integration of this subject into standard academic curriculum (Spadaro and Hunker, 2016). The introduction of mindfulness practices into the classroom has been explored as a tool for academic integration (Lee and Himmelheber, 2016), and further supported by research emphasizing a need to maintain a subjective nature within curricula (Chulguen and Goralski, 2016). There is an identified efficacy in capturing self-reported experiences of curricular-based mindfulness practices to determine perceived student-value, including capturing real-world experiences related to mindfulness as a means of demonstrating the impact of mindfulness training on self-reported quality of life (McConville et al., 2017). Based on recommendations from previous studies, there is a need for further research to explore the impact of mindfulness training on self-reported quality of life in an academic setting. The introduction of mindfulness into academic curriculum receives recommendation as an innovative approach to core curricular offerings, such as the efficacy of the pedagogy of mindfulness in the education of human services students (Banks, et al., 2016). Asynchronous online mindfulness meditation for American nursing students and practitioners has resulted in improved mood, stress levels, and cognitive focus (Spadaro and Hunker, 2016), and research involving European nurses has been conducted analyzing the benefits of mindfulness and how it impacted their own self-care and subsequent abilities to positively and effectively communicate with their patients (Sundling et al., 2017). Trends and analyses on the topic of mindfulness have been identified as a subject worth academic attention with the purpose of affecting and potentially modifying individual behavior, with suggestions that greater depth, breadth and awareness be brought to academic mindfulness topics with enhanced instructor training to align with intended personal outcomes (Schwind et al., 2017).
Methodology
A quantitative comparative design was used to explore the differences that exist between two groups of community college students through a self-reported survey instrument known as the Quality of Life Index (QLI). This study utilized an independent (unpaired) samples t test and examined the difference between two groups without random assignment as the groups are predetermined (Salkind, 2010). The comparison group consisted of students who did not take a mindfulness course and the intervention group consisted of students who did take a mindfulness course. The independent variable was assigned to the intervention group.
Population and sample selection
The setting for this study was a large Community College District in the Southwestern United States. The courses of interest surveyed were an entry-level online course that focused on stress management and mindfulness practices as a part of the curriculum and an entry-level online student success course without any focus on stress management or mindfulness practices. The population of interest was the community college student demographic. The target population was comprised of all students enrolled in a mindfulness course (intervention group) and all students enrolled in a specific non-mindfulness course (comparison group) during the 2021 academic year. Both groups were offered the same opportunity to participate in a voluntary survey and all respondents were de-identified. Non-probability convenience sampling was utilized for community college students within one institution stratified across one of two different community college courses (Saunders et al., 2012).
The a priori analysis determined the minimum target population to be 128 surveyed respondents from the combined treatment and comparison groups as calculated through G*Power Analysis (Faul et al., 2009) utilizing a medium effect size (d) of 0.50, an error probability (alpha) of 0.05, a power of 0.80, two groups (t test), and no covariate. This approach identified the mean differences between dispositional mindfulness and quality of life of the two groups of students. To account for respondent attrition an additional 15% was added to the a priori computed sample size resulting in a target sample size of 148.
Instrumentation
The validated survey instrument was the Generic III Version of the QLI, and demographic data (gender, age, ethnicity, marital status, highest completed level of schooling) were collected as a part of this survey. An optional field was available for participants to enter their email addresses for an opportunity to be entered into a raffle for one of five electronic gift cards. Completion of the survey was not a requirement for inclusion in the raffle. The QLI was utilized to answer the two research questions and allows for the calculation of five distinct scores: (1) overall quality of life score, (2) health and functioning subscale score, (3) social and economic subscale scores, (4) psychological/spiritual subscale score, and (5) family subscale score (Ferrans and Powers, 1985). The QLI identified to what extent, if any, there was a difference in health and functioning as measured by the results of responses to the second subscale of the QLI (health and functioning subscale score). To identify to what extent, if any, there was a difference in quality of life was the result of responses collected and scored responses to the entire QLI. The instrument is a 66-item questionnaire, divided into two sections (satisfaction with specific areas of life and the level of importance with those same areas of life) that measures quality of life in terms of life satisfaction and importance (Ferrans and Powers, 1985) with a 6-point Likert scale (Very Dissatisfied, Moderately Dissatisfied, Slightly Dissatisfied, Slightly Satisfied, Moderately Satisfied, Very Satisfied and Very Unimportant, Moderately Unimportant, Slightly Unimportant, Slightly Important, Moderately Important, Very Important, respectively). The QLI was administered as a between-groups post-test at the conclusion of the research period.
Validity and reliability
Validity of the QLI instrument was demonstrated by content and construct validity. Content validity was supported based on an extensive literature review of issues related to quality of life and on the reports of patients regarding the quality of their lives (Ferrans and Powers, 1985). Support for content validity was the result of an acceptably high rating using the Content Validity Index (Oleson, 1990). External validity has demonstrated application to the college-level demographics through internal consistency reliability with first-year community college students, measuring overall quality of life and health and functioning in both males and females, in Sweden (Vaez, et al., 2004). Internal consistency reliability for the QLI total scale was demonstrated through significance levels across 48 studies. Internal consistency reliability for the four subscales was supported by 24 studies (Ferrans, 2020). Temporal reliability for the QLI total scale was supported by test-retest correlations (Rustoen et al., 1999).
Data
Data from surveys (QLI) were collected from both the intervention and comparison groups. The first dependent variable was a measure of the perception of health and functioning as measured by a subcategory the QLI, the second dependent variable was a measure of perception of quality of life as measured by the total score of the QLI.
Both dependent variables were measured through the QLI instrument between the two groups. This was a univariate analysis comprised of two groups, post-test only measure with two distributions each with an average and variation assessing treatment effect. The mean, standard deviation, minimum, maximum, z-skewness, and z-kurtosis were reported for each of the dependent variables for each group. Data were analyzed through SPSS with a simple t test for differences of means between the two groups, G*Power Analysis (Faul et al., 2009) to determine statistical power, and test for mean differences at a medium effect size with two groups. Raw data were collected from results of a Survey Monkey communication sent to the two separate groups with incomplete submissions, missing responses, and incomplete data sets not utilized.
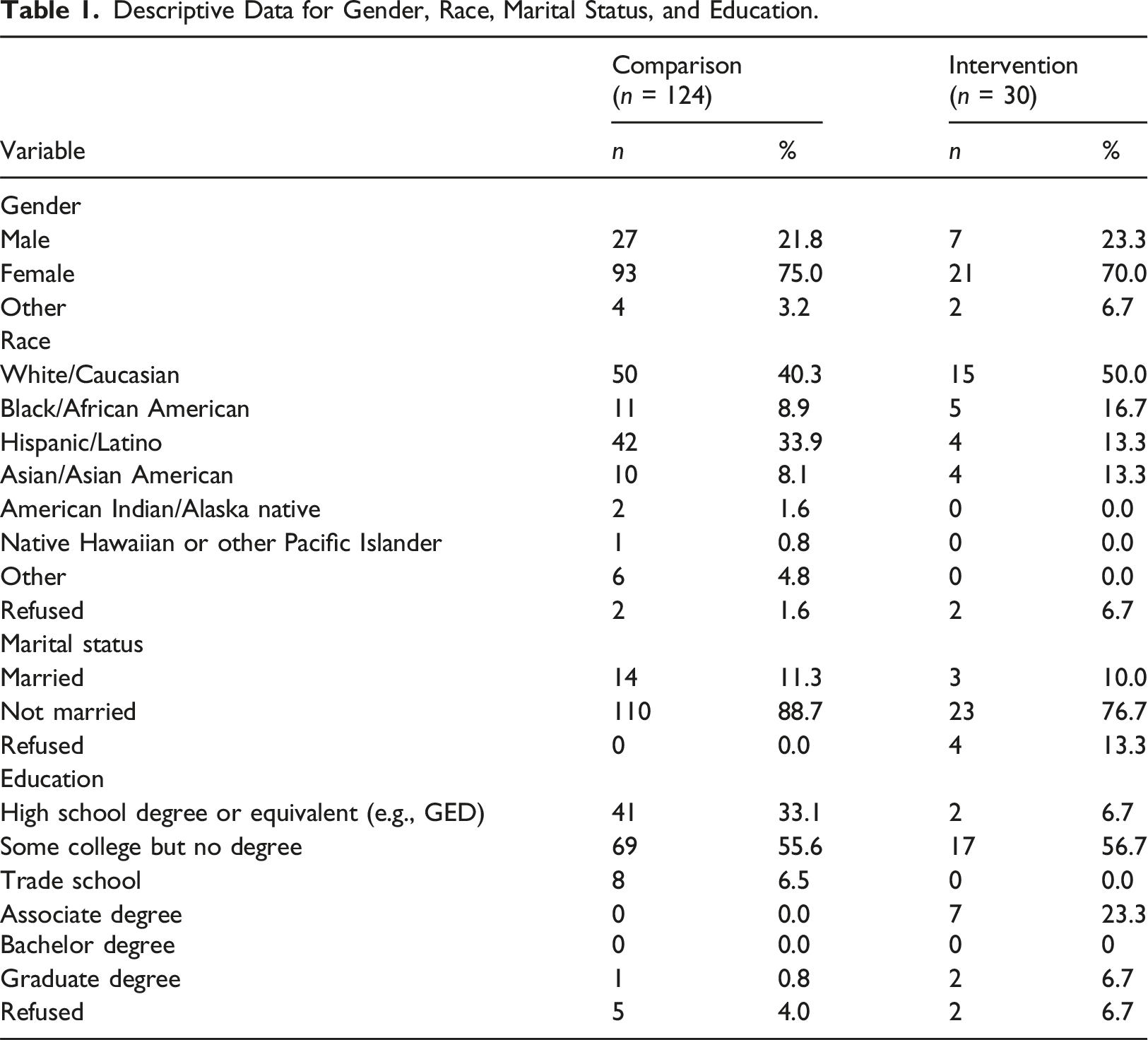
Raw data were collected via the Survey Monkey online collection tool in the form of two identical and separate surveys. There were 286 responses captured for the comparison group and 37 responses identified as the intervention group. Those who did not identify as being at least 18 years of age were removed from the respondent pool, resulting in a final clean data pool of 124 respondents for the comparison group and 30 respondents for the intervention group. The overall QLI score, and subscale scores, were scored according to the Description of Scoring provided by the QLI authors.
Analysis strategy
The a priori sample goal was to capture 74 respondents from both the comparison and intervention groups, resulting in 148 respondents which took into consideration a 15% attrition rate. Only 30 respondents were ultimately utilized to represent the intervention group, falling short of the intended 74. This is a substantial limitation as statistical power was based upon both the comparison and intervention groups reaching a minimum sample size of 74 each. However, the total sample size was 154 which still met the minimum target sample size while taking into consideration attrition.
Prior to conducting the inferential, non-directional two-tailed independent samples t-tests the data were checked for missing data using frequency counts. Data errors were checked using range scores to ensure all students had a score ranging from 0 to 30 for the QLI overall and subscale scores. Missing data were identified for 21 participants that were enrolled in the project and their data were omitted from the statistical analysis.
Descriptive Data for Gender, Race, Marital Status, and Education.
Descriptive data for age.

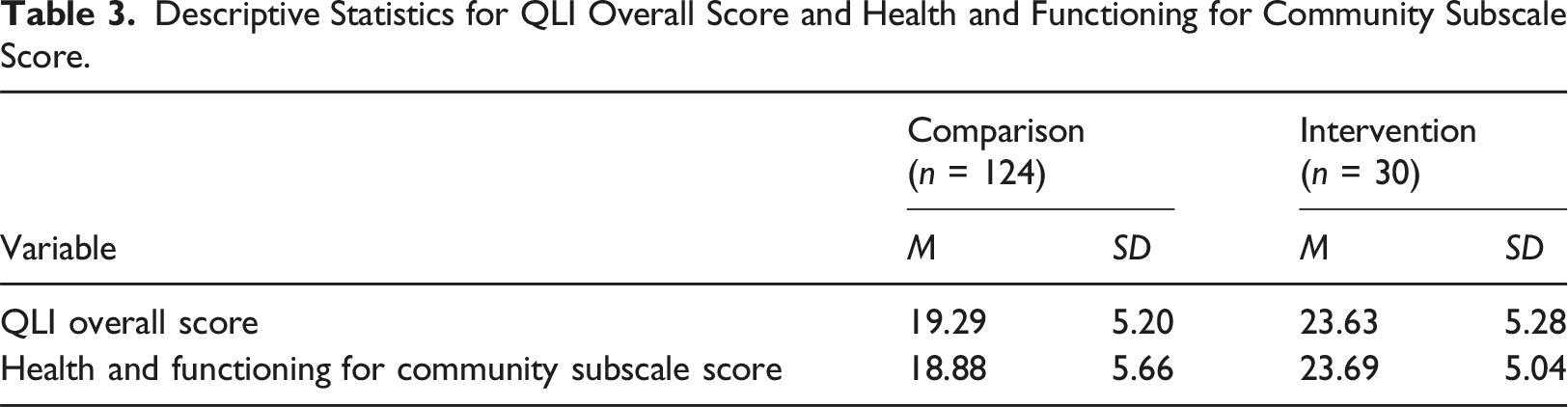
Descriptive Statistics for QLI Overall Score and Health and Functioning for Community Subscale Score.
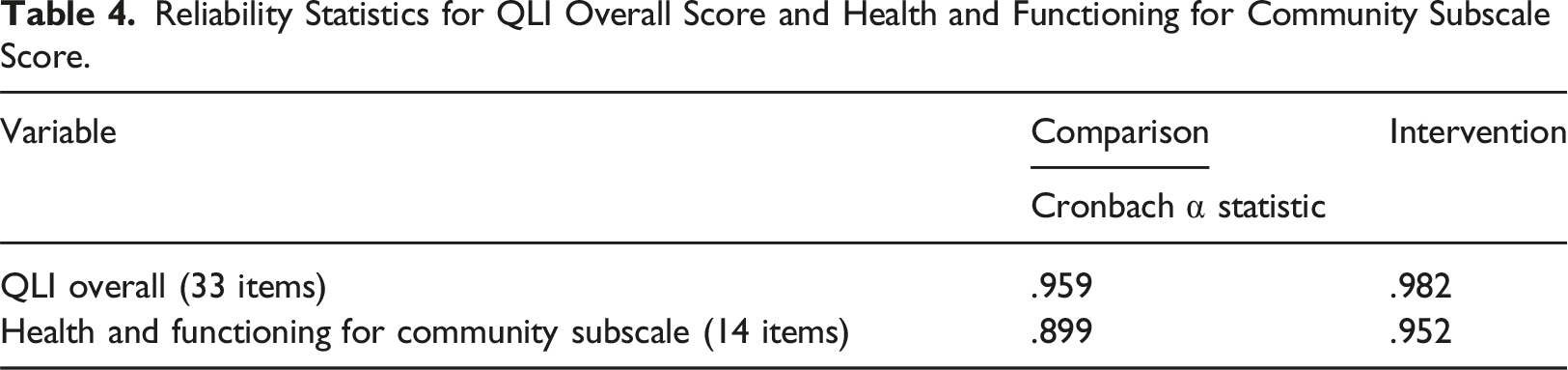
Reliability Statistics for QLI Overall Score and Health and Functioning for Community Subscale Score.
Post-hoc Cohen’s d Effect Sizes.
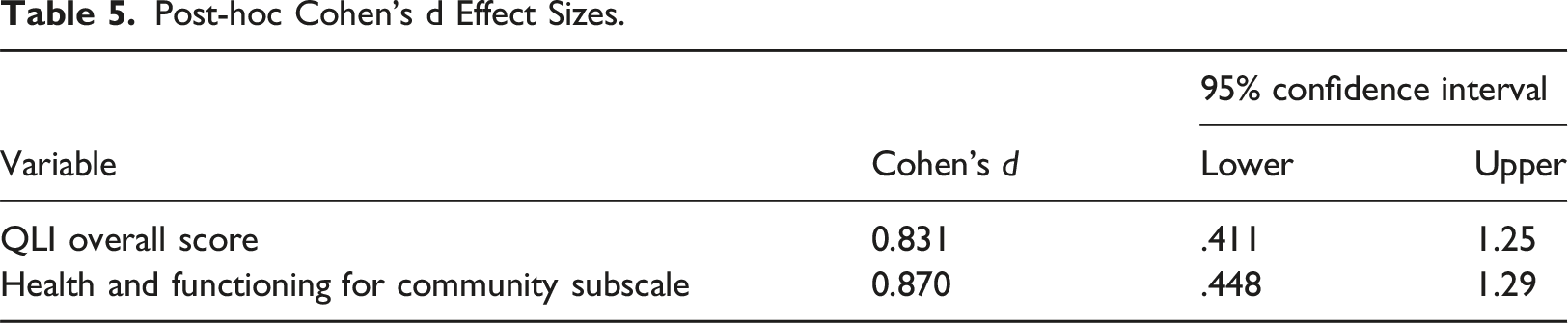
Post-hoc power analyses were conducted using G*Power 3.1.9.7 (Faul et al., 2009). The power calculated for the QLI Overall score results was 0.978 based on the effect size (d) of 0.831 and samples of 103 for the comparison group and 30 for the intervention group. For the Health and Functioning for Community Subscale, the effect size (d = 0.870) and samples showed an achieved power of .986.
Results
To what extent, if any, was there a difference in health and functioning for community college students based upon completion of mindfulness coursework? An independent samples t test was conducted to determine if the students who completed a mindfulness course had a significantly different health and functioning for community subscale score than the comparison group students (those who had completed a non-mindfulness course) on the QLI survey. The results are displayed in Table 6. The total sample size included in the analysis to address RQ was N = 132, as 22 of the 124 comparison group students had missing data for at least one item required to compute the health and functioning for community subscale score, thus, the sample size was n = 102 for the comparison group. All 30 students in the intervention group had complete data for the health and functioning for community subscale. There was a statistically significant difference in the health and functioning community subscale score between the comparison (M = 18.88, SD = 5.66) and the intervention group (M = 23.69, SD = 5.04), t (130) = -4.19, p < .001. The p-value is less than 0.05 which indicates a rejection of the null hypothesis, whereby demonstrating that there is a difference between the two groups. Direct comparison determined that the scores for the intervention group were higher than those for the comparison group. Therefore, the intervention group (M = 23.69, SD = 5.04) demonstrated greater health and functioning as compared to the comparison group (M = 18.88, SD = 5.66). This statistically significant result indicates strong evidence of rejecting the null hypothesis (H
01
: There is not a statistically significant difference in health and functioning by completing a mindfulness course compared to not completing a mindfulness course) as there is at least a 95% confidence level that perception of health and functioning is greater for those students who took a mindfulness course compared to those students who did not.
Independent Samples t test Results for Health and Functioning Scores.
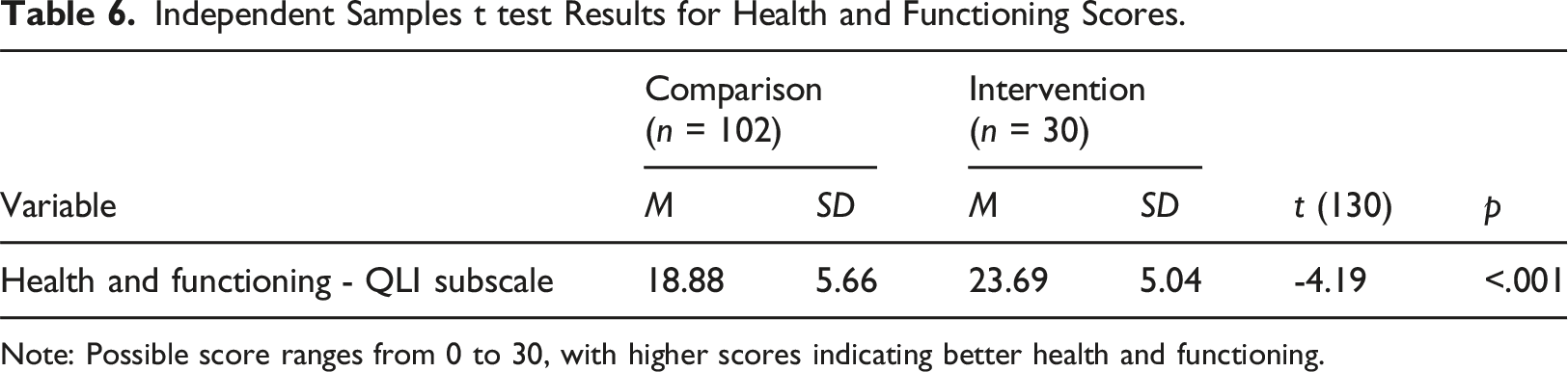
Note: Possible score ranges from 0 to 30, with higher scores indicating better health and functioning.
To what extent, if any, was there a difference in quality of life for community college students based upon completion of mindfulness coursework? An independent samples t test was conducted to determine if the students who completed a non-mindfulness course had a significantly different overall QLI index score than the comparison group students. The results are displayed in Table 7. The total sample size included in the analysis to address RQ was N = 133. This is because 21 of the 124 comparison group students had missing data for at least one item required to compute the overall QLI score, thus, the sample size was n = 103 for the comparison group. All 30 students in the intervention group had complete data for the health and functioning for community subscale. There was a statistically significant difference in the overall QLI score between the comparison (M = 19.29, SD = 5.20) and the intervention group (M = 23.63, SD = 5.28), t (131) = -4.01, p < .001. The p-value is less than 0.05, which indicates a rejection of the null hypothesis, whereby demonstrating that there is a difference between the two groups. Direct comparison determined that the scores for the intervention group were higher than those for the comparison group. Therefore, the intervention group (M = 23.63, SD = 5.28) demonstrated greater quality of life as compared to the comparison group (M = 19.29, SD = 5.20).
Independent Samples t test Results for Overall QLI Scores.
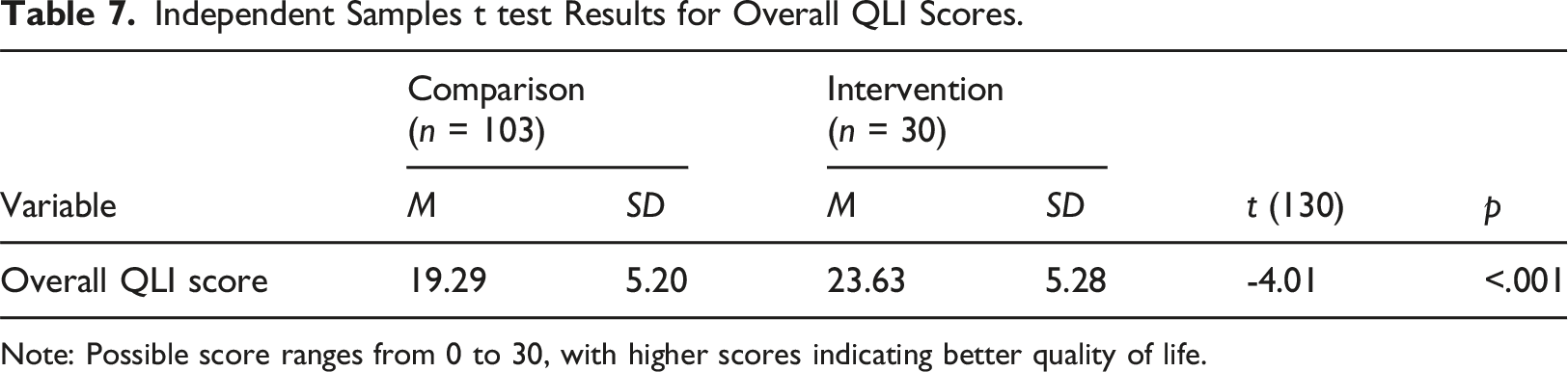
Note: Possible score ranges from 0 to 30, with higher scores indicating better quality of life.
Discussion
The results of this study demonstrated a statistically significant difference in health and functioning and quality of life between the comparison and intervention groups, contributing to the body of knowledge of mindfulness and informing theoretical, practical, and future implications.
There were several anticipated limitations prior to conducting this study based on the design and data collection approach that remained and were realized through the period of data collection: • Lack of response rates limited the scope of this study (Poynton et al., 2019). Although all students in both survey groups were provided the opportunity to participate, there was no control over how many actual respondents participated and furthermore provided adequate data to include in analysis. Having a reasonably equal data set from each response group was not achieved due to this limitation. However, sufficient statistical power was achieved with large effect sizes, indicating this limitation did not affect the ability to report significant findings. • As this was a posttest-only comparison group design (Thyer, 2012) the lack of a pretest did not account for predispositions of a mindfulness constant (covariate). By not identifying a respondent’s past experience with, or predisposition to, the tenants of mindfulness this indicates a possibility that their behavior and lifestyle at the time of this study was already mindful. Therefore, their responses may have been positive toward the benefits of mindfulness training regardless of whether they were in the comparison or intervention group. • This relatively straight-forward design also had the limitation of utilizing only a simple t test comparing two groups.
The theoretical foundation guiding this study included seminal theorists and applications supporting the research questions and presented hypotheses related to mindfulness theory. To align with mindfulness theory the intervention group for this research study were students enrolled in a mindfulness course, which offered an introduction to the theory, research and practice behind mindfulness and stress management as it relates to quality of life and personal self-care. The Health Belief Model focuses on the explanation of preventive health behavior (Rosenstock, 1974). Mindfulness Theory addresses being present and aware in the very moment, without distraction of the past or future (Langer, 1989). This seminal research encouraged further study into the interdisciplinary approach of palliative care for individuals with life-limiting conditions, such as relief from mental and physical stress, as well as pain and discomfort. The findings from this study provide evidence in agreement with recommendations of Rosenstock’s study that changing lifestyles and behaviors positively impacts overall perception of health through the tenants of Mindfulness (Langer, 1989).
Conclusion
There are three recommendations for future practice and four recommendations for future research based on the results and findings of this study.
Future practice
As an Element of the Classroom Setting. K-12 teachers, community college, and university faculty may benefit from integrating a mindfulness-based practice or element as a part of an opening classroom exercise. Bringing student attention back to the present moment and focus to the classroom experience without the distraction of outside stimuli can help ensure full attention to the task at hand. Decreasing outside stressors and improving sustained attention has been shown to improve self-regulation and improved classroom performance.
As a Stand-Alone Entry-Level Academic Course. College and University leadership teams may benefit from instituting a focused, stand-alone course on mindfulness for college students at the beginning of their program of study. Establishing healthy stress- and anxiety-management practices and behavior modification at the onset for brand new students could carry benefits not only throughout the semester but throughout the course of their academic journey.
As a Stand-Alone End-of-Program Academic Course. Post-secondary institutions offering professional programs and degrees rely upon successful practice-related licensure outcomes as a reporting mechanism of program success. Integrating a mindfulness-based intervention course prior to students sitting for licensure exams could help reduce test-taking stress and anxiety and prove to be a valuable student experience prior to the clinical experience and subsequent licensure testing.
Future research
Adopt an Experimental Research Methodology. Randomization was not utilized in this study’s comparative approach, therefore lacked the ability to conclude a causal association between the intervention and the reported outcomes (Padsakoff and Padsakoff, 2019). This proposed approach will afford the ability to measure causation based on an intervention.
Utilize a Control Group Pretest–Posttest Design. As this was a posttest-only comparison group design (Thyer, 2012), the lack of a pretest did not account for predispositions of a mindfulness constant (covariate). A pronounced limitation identified in this study was potential past experience with mindfuln1ess practices or meditation (Halamová et al., 2018).
Ensure Reasonably Equal Numbers of Respondents from Each Group. Lack of response rates also limited the scope of this study (Poynton et al., 2019). Although all students in both survey groups were provided the opportunity to participate, there was no control over how many actual respondents participated and furthermore provided adequate data to include in analysis. It is recommended that future research within this topic of mindfulness ensure that the pool of potential respondents is reasonably equal between both comparison and intervention groups.
Consider a Mixed-Method Research Design. Utilizing a quantitative method in a social science allows for the opportunity of individuality and respondent bias versus a study in the biological or physical sciences. It is recommended that future research within this topic of mindfulness introduce a qualitative survey element, should the same QLI survey instrument be utilized, in order for respondents to clarify and expand upon their responses.
Supplemental Material
Supplemental Material - A comparative study of an online mindfulness coursework: Implications for health and functioning and quality of life
Supplemental Material for A comparative study of an online mindfulness coursework: Implications for health and functioning and quality of life by Steve Peterson in Power and Education
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient or public contribution
De-identified and voluntary survey participation of community college students was involved in this study.
Data Availability Statement
Peterson, Steve (2023): Research Data - Steve Peterson. figshare. Dataset. https://doi.org/10.6084/m9.figshare.22818056.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.