
Abstract
Introduction
ADHD is increasingly recognized as a lifelong condition, affecting an estimated 9% of children (Bloom, Cohen, & Freeman, 2012) and 4.4% of adults (Kessler et al., 2006) in the United States.
Numerous studies have investigated the negative impact of ADHD in adults on educational attainment, employability, and productivity in the workplace, as well as on functional ability, self-esteem, and social functioning (Agarwal, Goldenberg, Perry, & IsHak, 2012; Bernfort, Nordfeldt, & Persson, 2008; Biederman et al., 2006; Fredriksen et al., 2014). One study involving a large manufacturing company found that ADHD was associated with a 4% to 5% reduction in work performance (p = .001), as well as greater odds of sickness absence (p = .013) and workplace accident injuries (p = .024) (Kessler, Lane, Stang, & Van Brunt, 2009). Another study demonstrated a higher rate of work-related injury claims by individuals with ADHD than by individuals without ADHD (21.5% vs. 15.7%; p < .0001; Hodgkins, Montejano, Sasane, & Huse, 2011). The loss of productivity observed in adults with ADHD may be partly caused by poor time management, procrastination, and distractibility, factors which also have a negative impact on quality of life (Asherson et al., 2012). Quality of life can be further impaired by comorbidities such as anxiety and mood disorders, which are common in adults with ADHD (Kessler et al., 2006; Rosler, Casas, Konofal, & Buitelaar, 2010). Furthermore, adults with ADHD have impaired social functioning, including problems sustaining stable relationships, antisocial behaviors, and lower self-esteem, compared with individuals without the condition (Asherson, 2005).
Historically, ADHD was perceived to be a childhood disorder that individuals would outgrow as they matured (Baron, Pato, & Cyr, 2011). In fact, approximately 50% to 75% of children with ADHD continue to meet diagnostic criteria for the disorder in later life as adolescents and also as adults (Montejano, Sasane, Hodgkins, Russo, & Huse, 2011). However, few published data are available on the burden of ADHD symptoms on undiagnosed adults. In 2007, it was estimated that less than 20% of adults with ADHD are diagnosed and/or treated (Newcorn, Weiss, & Stein, 2007). Both the presence of common comorbidities, such as depression and anxiety, and variability in presentation throughout development can complicate diagnosis (Wilens & Dodson, 2004). A lack of diagnosis is reported to impair psychological health (Adler et al., 2008).
The Validate Attitudes and Lifestyle Issues in Depression, ADHD and Troubles with Eating (VALIDATE) study of the 2012 and 2013 U.S. National Health and Wellness Survey was undertaken to estimate the symptom burden of ADHD in a nationally representative sample of U.S. adults. The study collected information on ADHD diagnosis, and assessed ADHD symptoms, health-related quality of life (HRQoL), functioning, and productivity.
Using the VALIDATE study data, the aim of our analysis was to explore the association between diagnosis and outcomes in adults with symptoms of ADHD. The impact of an ADHD diagnosis on HRQoL, work productivity, functioning, and self-esteem in U.S. adults was estimated by comparing these outcomes in respondents diagnosed with ADHD at some point in their life with those in respondents with self-reported ADHD-like symptoms but no previous clinical diagnosis.
Method
Study Design
The overall study procedures and recruited sample have been previously described (Cossrow et al., 2016; Pawaskar, Witt, Supina, Herman, & Wadden, 2017). Briefly, a representative sample of 69,972 U.S. adults aged 18 years or older who completed the 2012 and 2013 U.S. National Health and Wellness Survey were invited to participate in the VALIDATE study (conducted between 9 October and 29 October 2013). The study protocol was reviewed and approved by an Institutional Review Board (Sterling, Institutional Review Board #4509) before study data collection. Study participants provided consent before completing the survey and received panel points to be used for consumer goods (e.g., gift cards) as reimbursement for their time. The information collected was de-identified to ensure respondent privacy and confidentiality.
The VALIDATE survey consisted of a customized questionnaire designed to collect data on sociodemographic and clinical characteristics and lifestyle, as well as responses to several validated HRQoL, work productivity, daily functioning, and self-esteem questionnaires. Responses to the Adult ADHD Self-Report Scale (ASRS) version 1.1 questionnaire (Kessler et al., 2005) incorporating the definition of ADHD from the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000) were also collected to assess symptoms of ADHD experienced in the past 6 months.
Respondents were divided into two groups: those who reported having received a diagnosis of ADHD by a health care provider at any point in their lives (ADHD-diagnosed respondents), and those who responded negatively when asked if they had ever received an ADHD diagnosis, but who had symptoms potentially consistent with ADHD based on their responses to the ASRS-V1.1 (symptomatic respondents). Women who were pregnant or who reported being pregnant over the 12 months preceding the study were excluded from the analysis.
Outcome measures that were compared between the two groups included the following: the Work Productivity and Activity Impairment: General Health (WPAI:GH) version 2.0 questionnaire; the Sheehan Disability Scale (SDS); the EuroQoL five-dimensional five-level (EQ-5D-5L) questionnaire; and the Rosenberg Self-Esteem Scale (RSES). Sociodemographic characteristics and reported comorbid physical and mental health conditions were also compared between the two groups.
Statistical Analyses
To control for potential diagnosis selection bias, respondents diagnosed with ADHD were matched, according to sociodemographic characteristics and comorbid conditions, with a variable number of symptomatic respondents within the same sex-by-age group strata (ages 18-39, 40-54, and 55+ years) using propensity score matching (Rosenbaum & Rubin, 1983). The propensity score of diagnosis was estimated using separate logistic regressions for each sex-by-age group and included only baseline sociodemographic and comorbid condition covariates. Logistic regression covariates were entered in a stepwise fashion with a probability significance of p < .1 for both entry and removal.
Respondents were matched by propensity score within each sex-by-age group stratum using variable optimal matching, with up to four controls per case (Stuart, 2010). The Statistical Analysis Software (SAS) VMATCH macro (SAS Institute Inc., Cary, NC, USA) was used for the matching based on Euclidean distances between cases and controls (Kosanke & Bergstralh, 2004).
The effect of ADHD diagnosis on each outcome measure was estimated using an indicator variable for the diagnosed group, and was adjusted for covariates that remained imbalanced after matching within at least one of the six sex-by-age group strata comparisons. A family-wise significance level of p < .0085 was used for comparison tests based on Šidák’s correction method. Generalized mixed models were fitted and implemented using the SAS MIXED procedure (SAS/STAT® 9.3 User’s Guide, 2011), accounting for matched sets clustering. Non-linear mixed Tobit regression models were used for EQ-5D-5L index values to accommodate censoring of values at 1 (perfect health; Scott Long, 1997; Tobin, 1958). Least-squares (LS) means (95% confidence intervals) for respondents diagnosed with ADHD and for those with symptomatic ADHD were provided, and the difference in the LS means was calculated.
All statistical tests were two sided and there was no p-value adjustment for multiple comparisons other than that mentioned above. Data were summarized using descriptive statistics (number of respondents [n], mean, standard deviation, median, minimum, and maximum) for continuous variables, and frequency and percentage for categorical variables.
Results
Respondent Characteristics Before Matching
Of the 22,937 respondents to the VALIDATE survey, 444 participants had been diagnosed with ADHD and 1,055 participants reported ADHD-like symptoms but had no previous clinical diagnosis. Key sociodemographic, lifestyle, and comorbid condition characteristics before matching are summarized in Table 1. Mean ages were 42.5 and 43.9 years (p = .070) for respondents diagnosed with ADHD and for those with symptomatic ADHD, respectively. In total, 53.4% of respondents diagnosed with ADHD and 46.9% of symptomatic respondents were men (p = .023). Other statistically significant differences in sociodemographic and lifestyle characteristics between groups before matching were the following: more respondents diagnosed with ADHD (86.7%) were of second or higher generation living in the United States compared with symptomatic respondents (77.3%; p < .001), and respondents diagnosed with ADHD were more likely to be white (80.0% vs. 69.2%; p < .001) or of mixed racial background (5.2% vs. 3.0%; p < .001) and were more likely to be employed (55.2% vs. 47.4%; p = .024) than the symptomatic respondents (Table 1).
Key Sociodemographic, Lifestyle, and Comorbid Condition Characteristics Among Unmatched Respondents Diagnosed With ADHD and With Symptomatic ADHD.
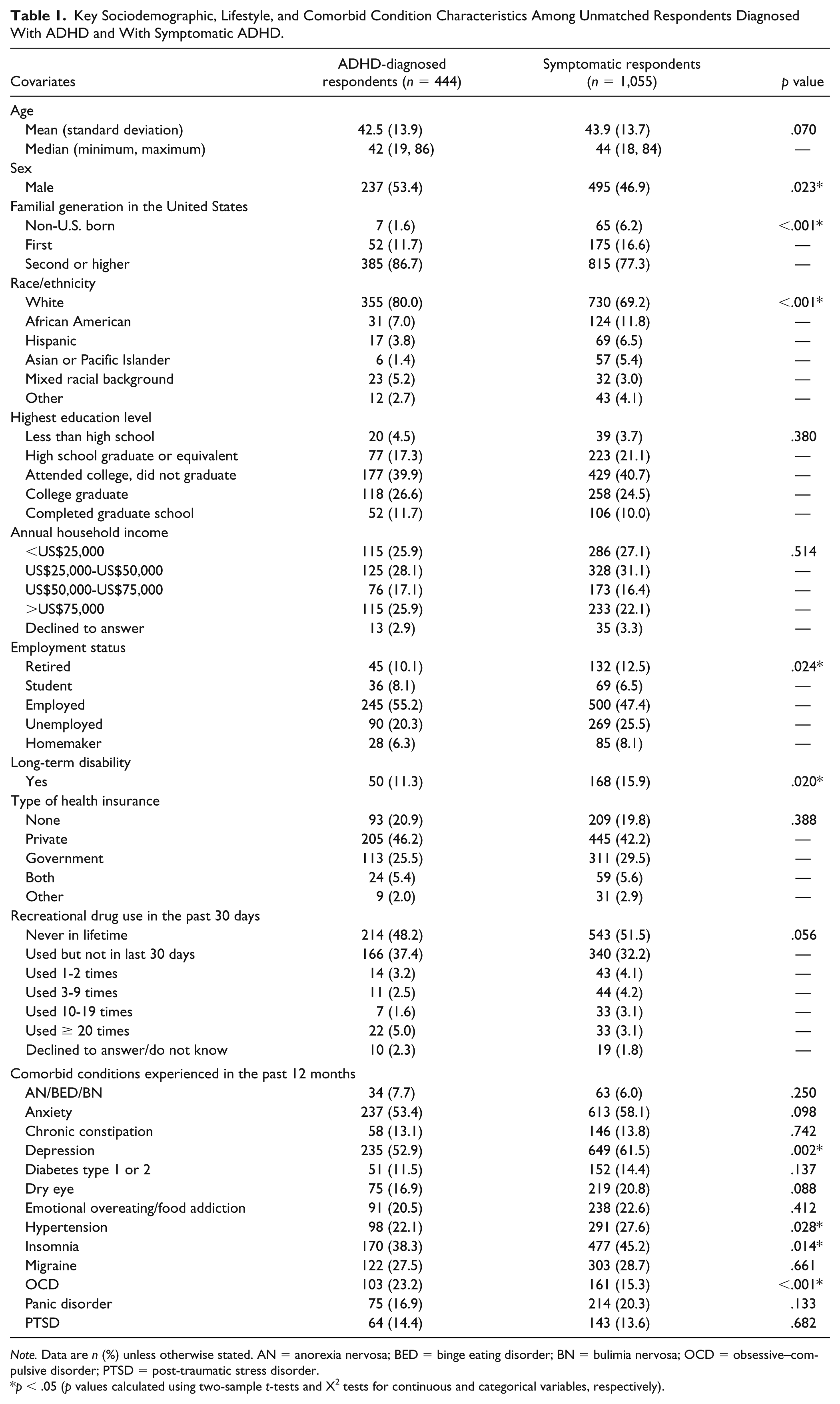
Note. Data are n (%) unless otherwise stated. AN = anorexia nervosa; BED = binge eating disorder; BN = bulimia nervosa; OCD = obsessive–compulsive disorder; PTSD = post-traumatic stress disorder.
p < .05 (p values calculated using two-sample t-tests and X2 tests for continuous and categorical variables, respectively).
Before matching, significant differences in the prevalence of comorbidities were observed between the two cohorts. Depression, hypertension, and insomnia were more common among respondents who were symptomatic than among those diagnosed with ADHD, whereas respondents diagnosed with ADHD had higher rates of obsessive-compulsive disorder.
Sociodemographic Characteristics, Comorbidities, and Lifestyle Variables After Matching
After matching, comparisons of covariates were conducted between respondents diagnosed with ADHD (n = 436) and symptomatic respondents (n = 867) within each of the six sex-by-age groups. Values for generations of family living in the United States (non-U.S. born, first generation, or second or higher generation) and rates of depression in the past 12 months were found to be significantly different (after correction for multiple comparisons) in at least one comparison (data not shown). These covariates were carried forward as independent variables in the subsequent regression models.
Comparing Outcomes After Matching
Compared with symptomatic respondents, respondents with a formal diagnosis of ADHD had significantly better unadjusted mean scores for WPAI:GH Work Productivity Loss (29.32 vs. 49.15; p < .001), WPAI:GH Activity Impairment (36.97 vs. 53.00; p < .001) and significantly better mean SDS total and subscale scores (all p < .001) (Table 2). Respondents diagnosed with ADHD also had better unadjusted mean EQ-5D-5L Index (Utility) scores (0.78 vs. 0.70; p < .001), EuroQoL visual analog scale (EQ VAS) Health State scores (72.46 vs. 65.05; p < .001) and RSES scores (19.30 vs. 15.17; p < .001) compared with symptomatic respondents (Table 2). EQ-5D-5L subscale scores showed that respondents diagnosed with ADHD had significantly lower rates of problems associated with mobility, self-care, usual activities, pain/discomfort, and anxiety/depression than symptomatic respondents (p < .05; data not shown).
Comparison of Outcomes Between Matched Respondents with Diagnosed ADHD and With Symptomatic ADHD (Unadjusted).
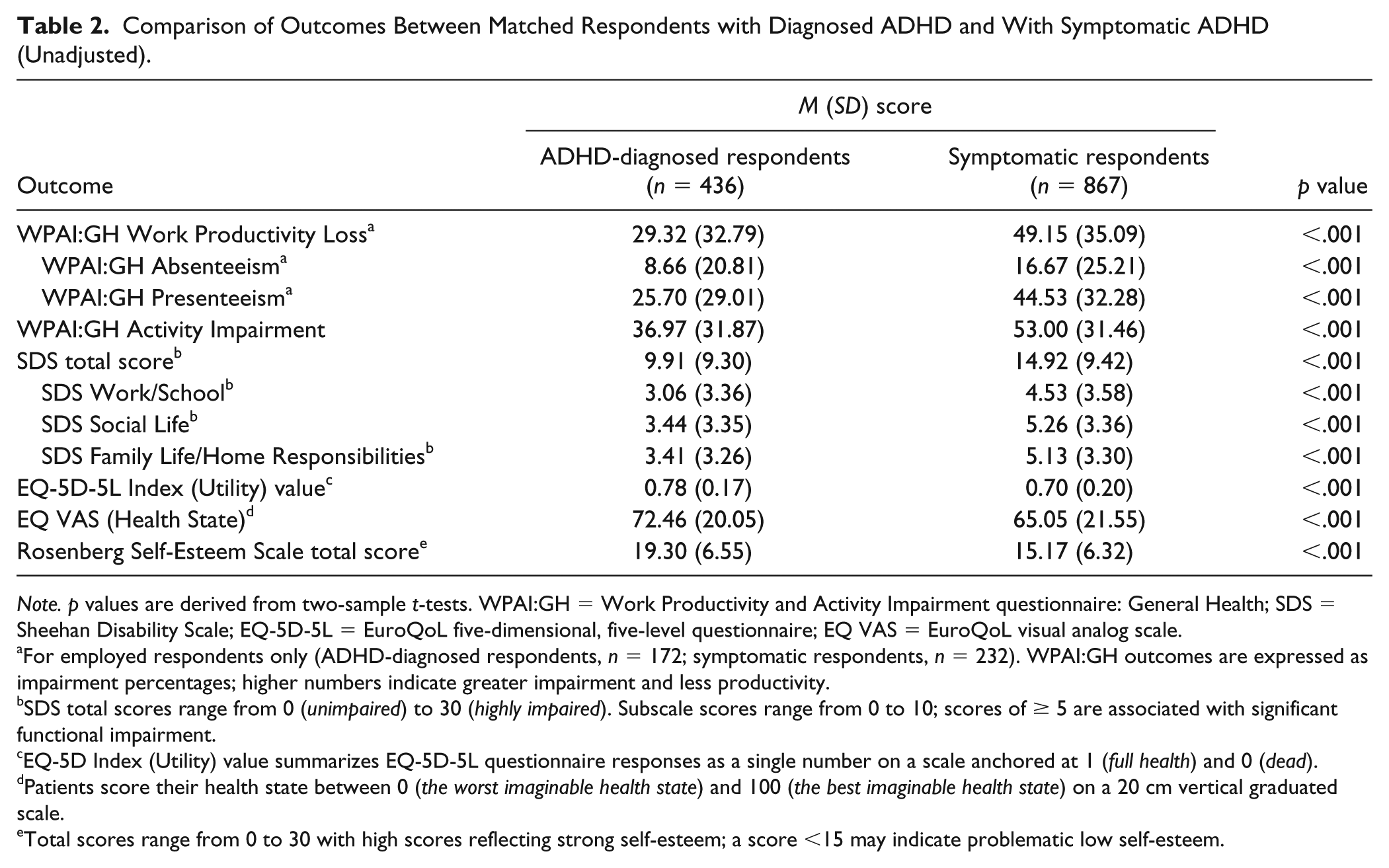
Note. p values are derived from two-sample t-tests. WPAI:GH = Work Productivity and Activity Impairment questionnaire: General Health; SDS = Sheehan Disability Scale; EQ-5D-5L = EuroQoL five-dimensional, five-level questionnaire; EQ VAS = EuroQoL visual analog scale.
For employed respondents only (ADHD-diagnosed respondents, n = 172; symptomatic respondents, n = 232). WPAI:GH outcomes are expressed as impairment percentages; higher numbers indicate greater impairment and less productivity.
SDS total scores range from 0 (unimpaired) to 30 (highly impaired). Subscale scores range from 0 to 10; scores of ≥ 5 are associated with significant functional impairment.
EQ-5D Index (Utility) value summarizes EQ-5D-5L questionnaire responses as a single number on a scale anchored at 1 (full health) and 0 (dead).
Patients score their health state between 0 (the worst imaginable health state) and 100 (the best imaginable health state) on a 20 cm vertical graduated scale.
Total scores range from 0 to 30 with high scores reflecting strong self-esteem; a score <15 may indicate problematic low self-esteem.
Relationship Between Diagnosis and Outcomes—Adjusted Analysis After Matching
LS means for WPAI:GH Productivity Loss and WPAI:GH Activity Impairment were significantly lower in respondents diagnosed with ADHD than in symptomatic respondents (WPAI:GH Productivity Loss, 39.37 vs. 55.62, respectively; WPAI:GH Activity Impairment, 41.73 vs. 55.78, respectively; p < .001 for both). Respondents diagnosed with ADHD also had a significantly lower SDS total score (less impairment), higher self-rated health state based on the EQ-5D-5L, and higher RSES total score (better self esteem) than symptomatic respondents (Table 3).
Comparison of Outcomes Between Matched Respondents With Diagnosed ADHD and With Symptomatic ADHD (Adjusted Least-Square Means Model).
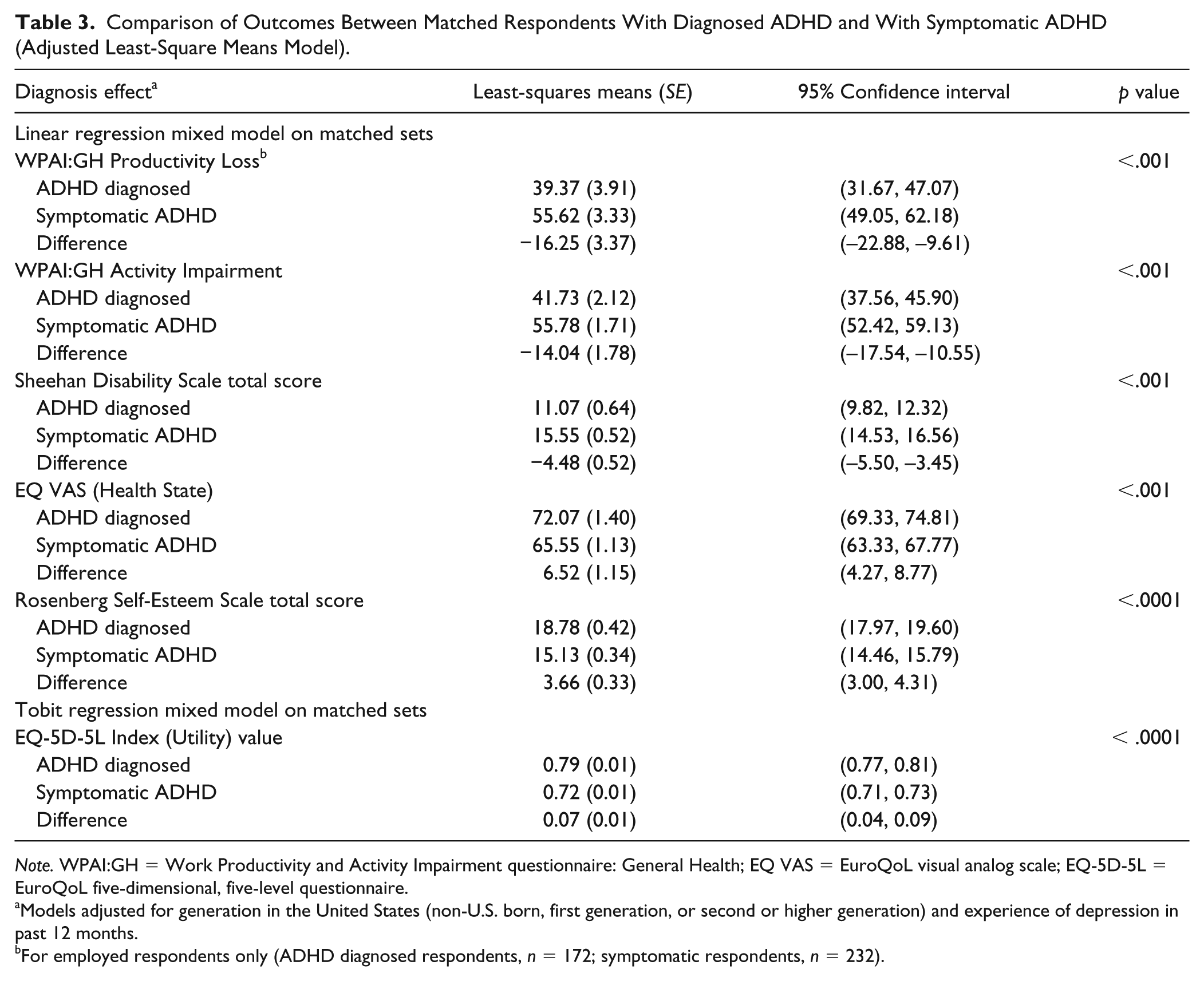
Note. WPAI:GH = Work Productivity and Activity Impairment questionnaire: General Health; EQ VAS = EuroQoL visual analog scale; EQ-5D-5L = EuroQoL five-dimensional, five-level questionnaire.
Models adjusted for generation in the United States (non-U.S. born, first generation, or second or higher generation) and experience of depression in past 12 months.
For employed respondents only (ADHD diagnosed respondents, n = 172; symptomatic respondents, n = 232).
Discussion
In this nationally representative sample of U.S. adults, we demonstrate that the burden of ADHD is greater in adults with symptomatic ADHD who have not been clinically diagnosed than in adults who have received a formal diagnosis of ADHD. Compared with symptomatic individuals, those with an ADHD diagnosis performed significantly better in measures of work productivity, quality of life, functioning, and self-esteem. These findings highlight the importance of an evaluation and diagnosis in adults with symptoms of ADHD, and hence access to the resources and treatment that may serve to improve outcomes.
Employed respondents with symptomatic ADHD reported significantly higher levels of absenteeism, presenteeism, and overall work productivity loss compared with those with a diagnosis of ADHD, as measured by the WPAI:GH. For both cohorts, presenteeism made a greater contribution to the loss in overall work productivity than absenteeism. Accordingly, any economic costs associated with individuals being less productive while at work may be greater than those due to individuals missing work because of their health problems.
Individuals with symptomatic ADHD showed significantly greater functional impairment than those with a diagnosis across all three items of the SDS (Social Life, Family Life/Home Responsibilities, and Work/School). In both cohorts, the highest SDS score (greatest impairment) was observed for the Social Life item, suggesting that individuals with symptoms of ADHD may have greater difficulty in negotiating the external social environment than the home environment, where adaptation and adjustment to impairments may be easier.
EQ-5D-5L is a generic HRQoL instrument that has been shown to be sensitive to ADHD in children (Bouwmans et al., 2014). Studies that have used the EQ-5D-5L instrument to assess the impact of ADHD on HRQoL in adults have recruited populations with a high rate of psychiatric comorbidities (Karlsdotter et al., 2016; Lensing, Zeiner, Sandvik, & Opjordsmoen, 2015). In the present study, adults with symptomatic ADHD reported a significantly lower HRQoL than respondents diagnosed with ADHD. Similarly, RSES scores indicated lower self-esteem in the symptomatic respondents compared with those reporting a previous diagnosis of ADHD.
Few data have been published on the impact of the lack of a diagnosis in adults exhibiting ADHD-like symptoms. A study by Able, Johnston, Adler, and Swindle (2007) compared adults with symptoms of ADHD but no formal diagnosis, individuals with an ADHD diagnosis and adults without ADHD (Able et al., 2007). Adults without symptoms of ADHD reported lower rates of a previous history of psychiatric disorders and current depression than both the diagnosed and undiagnosed adults with symptoms of ADHD. In contrast to the present study, Able et al. found no significant differences in impairment between diagnosed and undiagnosed adults with symptoms of ADHD using the SDS. Of note, baseline characteristics (including age, race, educational level, socioeconomic factors, and comorbidities) differed between these two studies. In particular, Able et al. found similar rates of current depression between the respondents diagnosed with ADHD and those with symptoms that were undiagnosed, whereas, in the present study, rates of depression in the past 12 months were higher in adults with symptomatic ADHD. Furthermore, the two studies differed in design. The Able et al. study involved a fully insured managed care population (Able et al., 2007), whereas 20% of participants in the VALIDATE study were uninsured and the remainder had a variety of insurance plans. Also, participants in the previous study were allocated to cohorts based on claims data (medical claims and drug use) and ADHD screen (Able et al., 2007); in the VALIDATE study, however, groups were designated according to self-reported data. Importantly, unlike the Able et al. study, the present study used matching and adjusting methodologies to reduce the risk of confounding and selection bias.
There are several possible reasons as to why adults experiencing symptomatic ADHD may not seek a formal evaluation, including lack of awareness, underrecognition of symptoms, development of coping mechanisms, and adoption of a lifestyle that compensates for ADHD-related impairments. Such symptoms may also overlap with those of depression or anxiety, leading to a misdiagnosis or a lack of formal diagnosis (Asherson et al., 2012). From a health care perspective, primary care physicians are often untrained in the use of diagnostic or assessment tools to evaluate adults with suspected ADHD, and may feel less comfortable managing the disorder in adults than in children (Culpepper & Mattingly, 2010). Primary care physicians have been shown to be significantly less likely than psychiatrists to make an initial diagnosis of ADHD in adults if no pediatric ADHD diagnosis had previously been made (Faraone, Spencer, Montano, & Biederman, 2004). The present data demonstrate that improving the rate of diagnosis of ADHD in adults could yield benefits both to the affected individuals and to society.
The strengths of this retrospective study include the recruitment of a large, real-world population of nationally representative adults and the breadth of the outcome measures analyzed. However, the data should be interpreted in the light of a number of caveats. First, ADHD diagnosis, symptoms, and comorbid conditions were self-reported and no further clinical confirmation was provided. Second, respondents were screened for symptoms of ADHD using the ASRS, a self-reported instrument that is based on only a partial list of DSM-IV-TR-based questions; additional DSM-IV-TR criteria for ADHD in adults, including symptoms before the age of 7 years, presence of some impairment from symptoms in two or more settings, evidence of impaired functioning, and symptoms that cannot be explained by other psychiatric disorders, were not applied in this study (APA, 1994). Indeed, in this study, significantly greater proportions of respondents in the symptomatic group had experienced depression, hypertension or insomnia in the past 12 months compared those with an ADHD diagnosis. Nevertheless, although it is not a substitute for clinical diagnosis, the ASRS can provide a useful screening tool to assess the occurrence and severity of symptoms that may warrant further in-depth evaluation (Able et al., 2007; Adamis et al., 2018). Third, the study was based on a self-selected sample, which may limit the generalizability of the results. Finally, as a cross-sectional study, any conclusions related to temporal or causal relationships should be made with caution.
Conclusion
These analyses of the VALIDATE study data compared the burden of ADHD in U.S. adults who reported having been diagnosed with the condition with that in symptomatic but undiagnosed adults. This comparison revealed that individuals who had been diagnosed with ADHD were more likely to experience better functioning, HRQoL, and self-esteem than those with symptomatic ADHD. This result appears to be robust, withstanding several levels of increasingly rigorous statistical adjustment. However, these findings should be confirmed by additional studies employing equally rigorous statistical methods.
Footnotes
Acknowledgements
Under the direction of the authors and funded by Shire International GmbH, Dr A. Jones DPhil, and Dr E. Gandhi, PhD, of Oxford PharmaGenesis, Oxford, UK, provided writing assistance for this publication. Editorial assistance in formatting, proofreading, copy-editing, and fact-checking was also provided by Oxford PharmaGenesis.
Authors’ Note
Manjiri Pawaskar and Regina Grebla were at Shire at the time the study was conducted.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M. Madhoo is an employee of Shire and owns stock or stock options. R. Grebla and M. Pawaskar were employees of Shire at the time the study was conducted. M. Fridman is an employee of AMF Consulting, Inc and a consultant to Shire.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shire Development LLC. Although employees of the Sponsor were involved in the design, collection, analysis, interpretation, fact checking of information, and coordination and collation of comments, the content of this manuscript, the interpretation of the data, and the decision to submit the manuscript for publication in the Journal of Attention Disorders was made by the authors independently.