
Abstract
Background:
Previous reviews evaluating biofeedback (BF)-assisted pelvic floor muscle (PFM) training (PFMT) with or without electrical stimulation (ES) for women with stress urinary incontinence (SUI) have reported conflicting results, and no consensus has been reached on the optimal parameters for this intervention.
Objectives:
To (1) evaluate the effectiveness of non-invasive and invasive BF-assisted PFMT with or without ES for SUI in women and (2) investigate whether study design characteristics and intervention parameters affect treatment effects.
Design:
Systematic review with meta-analysis and meta-regression.
Data sources and methods:
Seven English and two Chinese databases were searched from inception to May 2025. Outcomes were synthesized as standardized mean differences (SMDs) or odds ratios (ORs) with 95% confidence intervals. Meta-regression was employed to investigate the impact of study design characteristics and intervention parameters on outcomes.
Results:
This review included 21 studies involving 2373 participants. Meta-analyses revealed significant effects of invasive BF-assisted PFMT on PFM strength (SMD 0.71 (0.29, 1.14), p = 0.001), urinary incontinence (UI) symptom severity (SMD −0.33 (−0.63, −0.03), p = 0.032), quality of life (QoL; SMD −1.10 (−1.78, −0.41), p = 0.002), and improvement/cure rate (OR 2.02 (1.25, 3.26), p = 0.004). Meta-analyses also revealed significant effects of both invasive (SMD −1.23 (−1.93, −0.52), p = 0.001) and non-invasive (SMD −1.23 (−1.77, −0.68), p < 0.001) BF-assisted PFMT on urine loss severity. Meta-regression analysis revealed higher improvement/cure rates when BF-assisted PFMT involved mildly challenging exercises, tailoring to patients’ abilities, therapist supervision, sessions of <10 min, durations of >1 h/week for ⩾8 weeks, and ⩾80%–95% adherence.
Conclusion:
Invasive BF-assisted PFMT can improve PFM strength, reduce urine loss and UI symptom severity, enhance QoL, and increase the improvement/cure rate. Non-invasive BF-assisted PFMT can reduce urine loss severity. However, these results must be interpreted cautiously due to methodological flaws, risks of bias, and substantial heterogeneity across the included studies. Further high-quality studies are warranted to confirm the effectiveness of invasive or non-invasive BF-assisted PFMT with or without ES for treating SUI in women. The recommended parameters may optimize treatment effects.
Trial registration:
PROSPERO (CRD42023473798).
Keywords
Introduction
The International Continence Society defines urinary incontinence (UI) as any involuntary loss of urine. 1 The prevalence of UI varies greatly, ranging from 25% to 45% globally, 2 20% to 52% in Hong Kong, 3 and 8.7% to 69.8% in Chinese women. 4 However, most studies suggest that the prevalence of any UI falls between 4% and 35% among adult women. 5 Despite its high prevalence, only a small percentage of women experiencing UI seek medical care and receive treatment due to low expectations of treatment efficacy, embarrassment, and social stigma.6,7
UI is categorized into stress UI (SUI), urge UI, and mixed UI (MUI), which has both stress-predominant and urge-predominant forms. 8 SUI is the most common type in women. It is characterized by the complaint of any involuntary loss of urine when intra-abdominal pressure increases during effort or physical exertion, or when sneezing or coughing. 9 In women, SUI often occurs due to weak pelvic floor muscles (PFMs) or vaginal connective tissue, leading to the insufficient urethral and bladder neck closure during increased intra-abdominal pressure, which is especially common after pregnancy and vaginal delivery.10,11 In recent decades, there has also been an increasing number of women suffering from SUI due to aging.5,12 SUI is associated with a heavy economic burden on individuals and healthcare systems and affects social relationships, emotional and physical health, and quality of life (QoL). 13 SUI also reportedly affects work function, sexual activity, and personal relationships in daily life and increases the risk of depression and anxiety in women. 14
Women with mild or moderate SUI usually undergo conservative treatments rather than surgical interventions. 15 Due to its non-invasiveness and lack of associated risks, PFM training (PFMT) is the first-line conservative treatment for SUI. 16 It reduces the impact of SUI by improving PFM strength. 17 However, the success of PFMT alone, without adjunct therapies, is often limited by the lack of training adherence due to an inability to isolate PFM contractions and poor motivation to perform the exercises. 18 Therefore, PFMT is often combined with non-invasive (e.g., a surface electrode) or invasive (e.g., a vaginal probe) biofeedback (BF) alone or in combination with electrical stimulation (ES) to facilitate accurate PFMs contraction, optimize the contraction, and retain motivation for PFMT among women with SUI. 18 However, the effectiveness of BF-assisted PFMT with or without ES remains uncertain, and studies have reported conflicting results. Previous reviews of BF-assisted PFMT with or without ES for SUI indicate that BF-assisted PFMT improves cure and improvement rates, QoL, and PFM strength.19–21 In contrast, a review in 2019 reported that BF-assisted PFMT does not offer therapeutic benefits over alternative interventions in terms of QoL, PFM strength, and amount of urine loss. 22 However, no systematic reviews have evaluated the effectiveness of non-invasive BF-assisted PFMT for treating women with SUI. Additionally, none of the previous systematic reviews performed meta-regression to explore the impact of study design characteristics and intervention parameters (e.g., sample size, intervention week, and Physiotherapy Evidence Database Scale (PEDro) score) on treatment effects. Thus, there is a need to conduct a systematic review, meta-analysis, and meta-regression to allow more robust conclusions.
Therefore, this study aimed to (1) evaluate the effectiveness of invasive and non-invasive BF-assisted PFMT with or without ES in terms of QoL, PFM strength, severity of urine loss, improvement/cure rate, and severity of UI symptoms among women with SUI, and (2) investigate whether study design characteristics and intervention parameters impact treatment effects.
Materials and methods
This meta-analytic review was developed and reported in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. 23 The PRISMA checklist is provided in Supplemental Appendix 1. This review was conducted in accordance with a protocol prospectively registered in the PROSPERO database (CRD42023473798).
Search strategy
Seven English databases (Cochrane Library, Embase, PubMed, CINAHL, PEDro, Web of Science, and Scopus) and two Chinese databases (Wanfang and CNKI) were initially searched for relevant articles from their inception to October 2023, with the searches updated in May 2025. The search strategy included a comprehensive list of medical subject headings or keywords relating to the target population (women with SUI or stress-predominant MUI), interventions (invasive or non-invasive BF-assisted PFMT with or without ES), outcome measures (severity of UI symptoms, severity of urine loss, QoL, PFM strength, and improvement/cure rate), and study design (randomized controlled trials (RCTs)). A detailed list of the search terms is provided in Supplemental Appendix 2. The reference lists of the identified articles were also manually searched to identify other relevant systematic reviews and studies.
Inclusion and exclusion criteria
Studies were included in this systematic review if they (1) were RCTs, pilot RCTs, or randomized cluster or cross-over studies; (2) included women aged over 18 years with SUI or stress-predominant MUI; (3) compared the intervention to no treatment, usual care, standard care, placebo, PFMT alone, or sham control; (4) utilized invasive or non-invasive BF-assisted PFMT with or without ES; and (5) evaluated PFM strength, QoL, improvement/cure rate, severity of urine loss, and severity of UI symptoms. Studies were excluded if they (1) were not published in English or Chinese; (2) included women with urge-predominant MUI, overactive bladder, or UI resulting from other diseases (e.g., spinal cord injury or multiple sclerosis), or included men or children with SUI; (3) were case series, case studies, single group studies, or quasi-experimental studies; (4) involved interventions such as Pilates, BF combined with behavioral therapy, Chinese herbal medications, extracorporeal magnetic stimulation, surgery or traditional Chinese medicine; or (5) were conference proceedings.
Records retrieved from the searches were imported into EndNote (version 21) for organization and management. After removing duplicate records, two authors (LZ and MUA) independently selected studies according to the selection criteria. The titles and abstracts of the retrieved references were initially screened for eligibility, followed by their full texts. Any disagreements between reviewers were resolved through discussion, and a third author (PK) was consulted when they could not be resolved through discussion.
Data extraction
Two authors (LZ and MUA) independently extracted the following data: (1) first author, country, publication year, and sample size; (2) participant characteristics (e.g., mean age); (3) intervention and control conditions; and (4) the mean and standard deviation or the number of women in the results reported at baseline (pre-intervention) and last available assessment (post-intervention).
Quality assessment
The methodological quality and risk of bias (RoB) of all included studies were evaluated using the PEDro scale and the Cochrane RoB 2 tool, respectively. The PEDro scores for the included studies were retrieved from the PEDro website (https://search.pedro.org.au/advanced-search). Two authors (LZ and MUA) independently scored the studies using the PEDro scale if they were not available in the PEDro database, and also evaluated the studies using the RoB 2 tool. The PEDro scores were categorized as follows: <4 = poor, 4–5 = fair, 6–8 = good, and 9–10 = excellent. 24
The level of evidence was evaluated using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach with the GRADEpro software (https://www.gradepro.org/). The GRADE classification was downgraded for RoB by one level if fewer than half of the studies included in the pooled analyses had a high RoB, and by two levels if at least half of the studies had a high RoB. 25 The level of evidence was downgraded for inconsistency by one level when visual or statistical heterogeneity (I2 > 50%) was present, and by two levels when both forms of heterogeneity were present. 26 The GRADE classification was downgraded for indirectness by one level if there was a single or minor difference across studies in populations, interventions, comparators, or outcomes, and by two levels if there were more than two or major differences. 26 The level of evidence was downgraded for imprecision by one level if the 95% confidence interval (CI) did not include a clinically important effect or if the total sample size across the studies was smaller than the estimated optimal information size (OIS) criterion, and by two levels if both were present. 25 The OIS was calculated for a two-arm, parallel-group design based on data from a previous study on BF-assisted PFMT, assuming an α of 0.05 and power of 80% (β = 0.2). 27 If the total sample size of the studies included in the meta-analysis was smaller than the estimated OIS, the studies providing evidence for that intervention were considered small. 28 The level of evidence was downgraded for publication bias if studies were industry-funded, appeared to be sponsored by individuals who could benefit from the results, or if there were study protocols in a trial registry, but no subsequent publications. 28 The overall level of evidence was evaluated as high, moderate, low, or very low. 29 Two authors (LZ and MUA) independently completed the GRADE assessment for all included studies. Any disagreements were resolved through discussion, and a third author (PK) was consulted when they could not be resolved through discussion.
Data analysis
Meta-analyses were conducted using the Comprehensive Meta-Analysis software (version 3, Biostat, Inc., Englewood, NJ, USA). Studies examining similar interventions (e.g., BF-assisted PFMT with ES and BF-assisted PFMT without ES) and outcome measures were synthesized. Subgroup analyses were performed by BF type (non-invasive or invasive). Effect sizes were calculated for continuous outcomes as standardized mean differences (SMDs) with 95% CIs, and for dichotomous outcomes as odds ratios (ORs) with 95% CIs. The I2 statistic was used to evaluate heterogeneity among the studies, with an I2 of >50% indicating potential heterogeneity. 30 A random effects model was implemented when I2 was >50%, and a fixed effects model was adopted otherwise. 30 Publication bias was assessed using Begg’s funnel plot and Egger’s regression asymmetry test. 31 A p < 0.05 was considered statistically significant.
Meta-regression analyses were performed to determine the impact of study design characteristics (e.g., sample size and PEDro score) and intervention parameters (e.g., intervention duration and adherence) on treatment effects. They were only performed when at least 10 studies reported data on the same variable. 32 The degree of challenge was determined based on the exercise position: a supine or lithotomy position was considered mildly challenging, a standing or upright position was considered moderately challenging, and the use of two or more positions was considered highly challenging. Between-study heterogeneity was quantified using the I² statistic, with a value of >50% indicating substantial heterogeneity. A p < 0.05 was considered statistically significant, and a regression coefficient (RC) between 0 and 1 was considered significant 33 ; a larger standardized RC indicates a stronger effect size. 34
Results
Study selection
The searches identified 5094 potentially relevant studies. After the manual and automatic removal of duplicates, 3887 studies were eligible for inclusion in this review. After title and abstract screening, 3789 studies were excluded, and the full texts of the remaining 98 studies were further evaluated for eligibility. Of these 98 studies, 21 met the eligibility criteria and were included in this systematic review and meta-analysis, of which 12 were included in the meta-regression analysis. The study search and selection process is illustrated in a PRISMA flowchart (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of studies through the review.
Study and patient characteristics
The characteristics of the 21 included studies are summarized in Table 1. Of the 21 included studies, 19 were prospective RCTs27,35–52 and two were pilot RCTs.53,54 Six were conducted in Asia,27,38,43,44,52,54 two in the Middle East,41,47 seven in Europe,36,37,39,40,48,50,53 and six in the Americas.35,42,45,46,49,51 Their sample sizes ranged from 21 to 600, comprising a total of 2373 participants (1154 in the experimental group and 1219 in the control group). The mean age of the participants ranged from 42.11 to 59.3 years.
Characteristics of included studies (n = 21).

Median ± standard deviation.
Number of women.
Median (First Quartile–Third Quartile).
Median (95% confidence interval).
Mean (95% confidence interval).
Mean difference (95% confidence interval).
Mean (min–max).
BF, biofeedback; Con, control group; ES, electrical stimulation; Exp, experimental group; ICIQ-SF, International Consultation on Incontinence Questionnaire-Short Form; ICIQ-UI-SF, International Consultation on Incontinence Questionnaire-Urinary Incontinence-Short Form; IIQ-7, Incontinence Impact Questionnaire, Short Form; I-QOL, Incontinence Quality of Life Questionnaire; KHQ, King’s Health Questionnaire; min(s), minute(s); MOS, Modified Oxford Scale; NR, not reported; PEDro, Physiotherapy Evidence Database; PFM, pelvic floor muscle; PFMT, pelvic floor muscle training; s, second.
The examined interventions included invasive BF-assisted PFMT (n = 18),27,35–37,39–49,51,53,54 invasive BF-assisted PFMT with ES (n = 3),38,50,52 and non-invasive BF-assisted PFMT (n = 2).47,54 The control condition was PFMT alone in all included studies (n = 21).27,35–54 Of the 21 included studies, eight assessed QoL,27,42,44,45,47,49,51,52 of which three utilized the Incontinence Quality of Life Questionnaire (I-QOL),27,44,52 two utilized the International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF),45,49 two utilized the Incontinence Impact Questionnaire, short form (IIQ-7),47,51 and one utilized the King’s Health Questionnaire (KHQ). 42 Thirteen studies assessed PFM strength using the Modified Oxford Scale (MOS) or perineometry.27,38–44,46–49,54 Thirteen studies reported the number of women who reported improvement/cure of incontinence.35–37,39–41,43,44,46–48,51,52 Ten studies assessed the severity of urine loss using a pad test.36,37,40,41,43,46,47,50,53,54 Five studies assessed the severity of UI symptoms using the International Consultation on Incontinence Questionnaire-Urinary Incontinence-Short Form (ICIQ-UI-SF).27,43,48,52,54
Quality assessment
The RoB of the included studies is summarized in Figure 2. Thirteen studies failed to clearly report their concealed allocation procedure, resulting in an unclear or high risk rating of the randomization process.27,35,38,39,42–44,47,50–54 Ten studies were found to have an unclear or high RoB in the outcome measurement due to a lack of assessor blinding.38,39,41,43,45,46,49–52 Sixteen studies presented unclear RoB of the selective reporting bias.27,35–39,41–44,46,47,49,50,52,53 Overall, of the 21 included studies, 2 had a low RoB,40,48 12 had a moderate RoB,27,36,37,42–44,47,50–54 and 7 had a high RoB.35,38,39,41,45,46,49

Summary of findings (Cochrane RoB 2).
The PEDro scores of the included studies are presented in Table 1, and the PEDro assessment of the included studies is reported in Supplemental Appendix 3. The mean PEDro score of the 21 included studies was 5.71 out of 10. Among the 21 included studies, 12 lacked assessor blinding,37–39,41,43,45,46,49–53 13 did not report allocation concealment,27,35,38,39,42–44,47,50–54 11 lacked intention-to-treat analysis,27,35,37–39,41,42,45,47,50,52 and 7 reported inadequate follow-up.38,39,41,43,46,48,49
The evidence profiles for each outcome measure generated by the GRADEpro Guideline Development Tool (GDT) are summarized in Table 2. The OIS was estimated at 400 participants. The overall GRADE level of evidence for the 21 studies included in the meta-analyses ranged from very low to moderate. For QoL, the GRADE quality was very low for the studies that used the ICIQ-SF. For PFM strength, the GRADE quality was very low for the studies that utilized the MOS and low for those that utilized perineometry. For the severity of UI symptoms, the GRADE quality was moderate for the studies that utilized the ICIQ-UI-SF. For the improvement/cure rate, the GRADE quality was low for the studies that reported the number of women who reported improvement/cure of incontinence. For the severity of urine loss, the GRADE quality ranged from low to very low for the studies that utilized the pad test. Serious RoB and inconsistency were the main factors leading to the downgraded level of evidence. Regarding the ORs, the visual inspection of funnel plots and Egger’s test (p = 0.27) provided no evidence of significant publication bias across the included studies (Supplemental Appendix 4).
Summary of findings (GRADE).
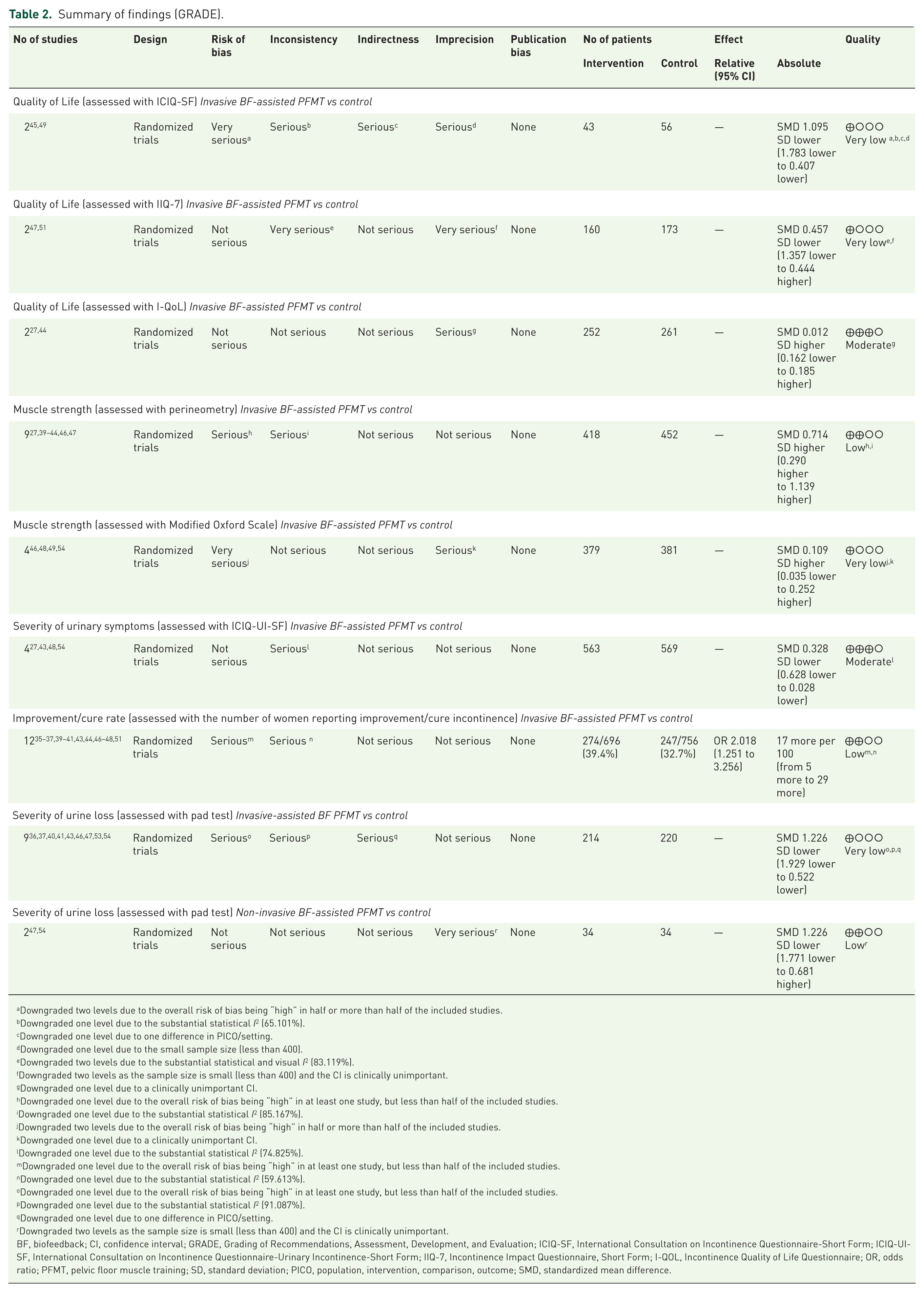
Downgraded two levels due to the overall risk of bias being “high” in half or more than half of the included studies.
Downgraded one level due to the substantial statistical I2 (65.101%).
Downgraded one level due to one difference in PICO/setting.
Downgraded one level due to the small sample size (less than 400).
Downgraded two levels due to the substantial statistical and visual I2 (83.119%).
Downgraded two levels as the sample size is small (less than 400) and the CI is clinically unimportant.
Downgraded one level due to a clinically unimportant CI.
Downgraded one level due to the overall risk of bias being “high” in at least one study, but less than half of the included studies.
Downgraded one level due to the substantial statistical I2 (85.167%).
Downgraded two levels due to the overall risk of bias being “high” in half or more than half of the included studies.
Downgraded one level due to a clinically unimportant CI.
Downgraded one level due to the substantial statistical I2 (74.825%).
Downgraded one level due to the overall risk of bias being “high” in at least one study, but less than half of the included studies.
Downgraded one level due to the substantial statistical I2 (59.613%).
Downgraded one level due to the overall risk of bias being “high” in at least one study, but less than half of the included studies.
Downgraded one level due to the substantial statistical I2 (91.087%).
Downgraded one level due to one difference in PICO/setting.
Downgraded two levels as the sample size is small (less than 400) and the CI is clinically unimportant.
BF, biofeedback; CI, confidence interval; GRADE, Grading of Recommendations, Assessment, Development, and Evaluation; ICIQ-SF, International Consultation on Incontinence Questionnaire-Short Form; ICIQ-UI-SF, International Consultation on Incontinence Questionnaire-Urinary Incontinence-Short Form; IIQ-7, Incontinence Impact Questionnaire, Short Form; I-QOL, Incontinence Quality of Life Questionnaire; OR, odds ratio; PFMT, pelvic floor muscle training; SD, standard deviation; PICO, population, intervention, comparison, outcome; SMD, standardized mean difference.
Effectiveness of interventions
Quality of life
The pooled analysis of data from two studies45,49 of good methodological quality, very low GRADE quality, and a high RoB revealed a significant effect of invasive BF-assisted PFMT compared to the control condition on QoL measured using the ICIQ-SF (SMD −1.10, 95% CI (−1.78, −0.41), p = 0.002, n = 99; Figure 3(a)). Meta-analysis of data from two studies47,51 of good methodological quality, very low GRADE quality, and moderate RoB revealed a nonsignificant effect of invasive BF-assisted PFMT compared to the control condition on QoL measured using the IIQ-7 (SMD −0.46, 95% CI (−1.36, 0.44), p = 0.32, n = 350; Figure A in Supplemental Appendix 5). Meta-analysis of data from two studies27,44 of good methodological quality, moderate GRADE quality, and moderate RoB also showed a nonsignificant effect on invasive BF-assisted PFMT compared to the control condition on QoL measured using the I-QoL (SMD 0.01, 95% CI (−0.16, 0.19), p = 0.893, n = 513; Figure B in Supplemental Appendix 5).

(a) Effect of invasive BF-assisted PFMT compared to control conditions on QoL using ICIQ-SF. (b) Effect of invasive BF-assisted PFMT compared to control conditions on MS using perineometry. (c) Effect of invasive BF-assisted PFMT compared to control conditions on the severity of UI symptoms using ICIQ-UI-SF. (d) Effect of invasive BF-assisted PFMT compared to control conditions on the improvement/cure rate. (e). Effect of invasive BF-assisted PFMT compared to control conditions on the severity of urine loss using the pad test. (f) Effect of non-invasive BF-assisted PFMT compared to control conditions on the severity of urine loss using the pad test.
PFM strength
Meta-analysis of data from nine studies27,39–44,46,47 of fair-to-good methodological quality, low GRADE quality, and low-to-high RoB showed a significant effect of BF-assisted PFMT to a control condition on PFM strength measured using perineometry (SMD 0.74, 95% CI (0.33, 1.14), p < 0.001, n = 887; Figure C in Supplemental Appendix 5). A subgroup analysis of these nine studies revealed a significant effect of invasive BF-assisted PFMT compared to the control condition on PFM strength (SMD 0.71, 95% CI (0.29, 1.14), p = 0.001, n = 887; Figure 3(b)).
Meta-analysis of data from four studies46,48,49,54 of good methodological quality, very low GRADE quality, and low-to-high RoB revealed a significant effect of BF-assisted PFMT compared to the control condition on PFM strength (SMD 0.14, 95% CI (0.001, 0.282), p = 0.049, n = 827; Figure D in Supplemental Appendix 5). These studies used the MOS grading to assess abnormalities in PFM strength, with a MOS grade of III or below considered a weak or absent contraction. 55 A subgroup analysis of these four studies revealed a nonsignificant effect of invasive BF-assisted PFMT compared to the control condition on PFM strength, as measured using the MOS (SMD 0.11, 95% CI (−0.04, 0.25), p = 0.138, n = 810; Figure E in Supplemental Appendix 5).
Severity of UI symptoms
Meta-analysis of data from four studies27,43,48,54 of fair-to-good methodological quality, moderate GRADE quality, and low-to-moderate RoB revealed a significant effect of BF-assisted PFMT compared to the control condition on the severity of UI symptoms, as measured using the ICIQ-UI-SF (SMD −0.52, 95% CI (−0.89, −0.15), p = 0.006, n = 1149; Figure F in Supplemental Appendix 5). A Subgroup analysis of these four studies revealed a significant effect of invasive BF-assisted PFMT compared to the control condition on the severity of UI symptoms, as measured using the ICIQ-UI-SF (SMD −0.33, 95% CI (−0.63, −0.03), p = 0.032, n = 1132; Figure 3(c)).
Improvement/cure rate
Meta-analysis of data from 12 studies35–37,39–41,43,44,46–48,51 of fair-to-good methodological quality, low GRADE quality, and low-to-high RoB revealed a significantly greater number of women reporting improvement/cure of incontinence in the BF-assisted PFMT group than in the control group (OR 2.12, 95% CI (1.33, 3.38), p = 0.002, n = 1510; Figure G in Supplemental Appendix 5). A subgroup analysis of these studies revealed a significant effect of invasive BF-assisted PFMT compared to the control condition on the improvement/cure rate (OR 2.02, 95% CI (1.25, 3.26), p = 0.004, n = 1476; Figure 3(c)).
Severity of urine loss
Meta-analysis of data from nine studies36,37,40,41,43,46,47,53,54 of fair-to-good methodological quality, very low GRADE quality, and low-to-high RoB revealed a significant effect of BF-assisted PFMT compared to the control condition on the severity of urine loss, as measured using the pad test (SMD −1.27, 95% CI (−1.92, −0.63), p < 0.001, n = 468; Figure H in Supplemental Appendix 5). A subgroup analysis of these studies revealed a significant effect of invasive BF-assisted PFMT compared to the control condition on the severity of urine loss, as measured using the pad test (SMD −1.23, 95% CI (−1.93, −0.52), p = 0.001, n = 434; Figure 3(e)). The subgroup analysis also revealed that two studies47,54 with good methodological quality, low GRADE quality, and moderate RoB also revealed a significant effect of non-invasive BF-assisted PFMT compared to the control condition on the severity of urine loss, as measured using the pad test (SMD −1.23, 95% CI (−1.77, −0.68), p < 0.001, n = 68; Figure 3(f)).
Analysis of data for 51 participants from a single study 47 evaluating the effect of non-invasive BF-assisted PFMT compared to a control condition revealed significant beneficial effects of the intervention on QoL, as measured using the IIQ-7 (SMD −0.90, 95% CI (−1.61, −0.20), p = 0.012); PFM strength, as measured using perineometry (SMD 0.98, 95% CI (0.27, 1.70), p = 0.007); and improvement/cure rate (OR 5.53, 95% CI (1.09, 25.21), p = 0.038). Analysis of data for 51 participants from a single study 54 evaluating the effect of non-invasive BF-assisted PFMT compared to a control condition revealed significant beneficial effects of the intervention on PFM strength, as measured using the MOS (SMD 0.94, 95% CI (0.23, 1.65), p = 0.009), and severity of UI symptoms, as measured using the ICIQ-UI-SF (SMD −1.64, 95% CI (−2.41, −0.86), p < 0.001). Analysis of data for 110 participants from a single study 52 evaluating the effect of invasive BF-assisted PFMT with ES revealed significant beneficial effects on the severity of UI symptoms, as measured using the ICIQ-UI-SF (SMD −1.25, 95% CI (−1.66, −0.84), p < 0.001); QoL, as measured using the I-QoL (SMD 2.34, 95% CI (1.85, 2.82), p < 0.001); and improvement/cure rate (SMD 7.11, 95% CI (1.94, 26.12), p = 0.003). Analysis of data for 60 participants from a single study 38 evaluating the effect of invasive BF-assisted PFMT with ES compared to a control condition revealed a significant beneficial effect on PFM strength, as measured using perineometry (SMD 0.58, 95% CI (0.06, 1.09), p = 0.029). Analysis of data for 40 participants from a single study 50 evaluating the effect of invasive BF-assisted PFMT with ES compared to a control condition revealed a significant beneficial effect on the severity of urine loss, as measured using the pad test (SMD −1.98, 95% CI (−2.73, −1.22), p < 0.001). Analysis of data for 21 participants from a single study 42 evaluating the effect of invasive BF-assisted PFMT compared to a control condition revealed a nonsignificant beneficial effect on QoL, as measured using the KHQ (SMD −0.32, 95% CI (−1.18, 0.54), p = 0.465). A detailed summary of the descriptive data is provided in Supplemental Appendix 6.
Meta-regression analysis
The meta-regression analyses included 12 studies (Table 3). They revealed that the effects of BF-assisted PFMT on the improvement/cure rate were greater when the intervention was provided for more than 1 h per week (RC 0.88, 95% CI (0.35, 1.40), p = 0.001, I2 = 61%) and for at least 8 weeks (RC 0.70, 95% CI (0.15, 1.23), p = 0.01, I2 = 66.23%). They also revealed that the intervention led to greater improvements in the improvement/cure rate when exercise adherence was at least 80%–95% (RC 0.58, 95% CI (0.02, 1.50), p = 0.04, I2 = 3.09%), sessions lasted less than 10 min (RC 0.40, 95% CI (0.006, 0.793), p = 0.047, I2 = 1.50%), and the exercises were mildly challenging (RC 0.83, 95% CI (0.06, 1.60), p = 0.04, I2 = 75.37%). Moreover, they revealed that the intervention led to greater improvements in the improvement/cure rate when BF-assisted PFMT was performed with a therapist (RC 0.76, 95% CI (0.28, 1.23), p = 0.002, I2 = 61%) and tailored to the participant’s ability (RC 0.85, 95% CI (0.36, 1.35), p = 0.001, I2 = 61%).
Results of meta-regression explore the effect of study-level characteristics on the improvement/cure rate.

BF, biofeedback; CI, confidence interval; h, hour; N, number; PEDro, Physiotherapy Evidence Database; PFMT, pelvic floor muscle training; RC, regression coefficient; SUI, stress urinary incontinence.
Bold indicates P < 0.05, which is statistically significant.
Discussion
The database searches identified 5094 potentially relevant records, of which 21 met the eligibility criteria and were included in this systematic review and meta-analysis. Of these 21 studies, 15 (71%) were of good methodological quality based on the PEDro quality assessment scale.27,35–37,40,42,44–49,51,53,54 Regarding RoB, 2 (9.5%) studies had a low RoB,40,48 12 (57.1%) had a moderate RoB,27,36,37,42–44,47,50–54 and 7 (33.4%) had a high RoB.35,38,39,41,45,46,49 The GRADE quality of the outcome measures varied from very low to moderate. Our findings suggest that invasive BF-assisted PFMT may be advantageous in enhancing QoL and the improvement/cure rate, strengthening PFM, reducing the severity of urine loss, and alleviating UI symptoms in women with SUI compared to control conditions. They also indicate that non-invasive BF-assisted PFMT may be beneficial for reducing the severity of urine loss. Based on the results of meta-regression analyses, the following parameters are recommended for BF-assisted PFMT for women with SUI: mildly challenging exercises tailored to the patient’s ability and performed under therapist supervision, sessions lasting less than 10 min, more than 1 h per week for at least 8 weeks, and at least 80%–95% adherence.
Promisingly, invasive BF-assisted PFMT appeared to improve PFM strength, reduce the severity of urine loss, and increase the improvement/cure rate. The effect size was large for the severity of urine loss (SMD −1.23) and medium to large for PFM strength (SMD 0.71). The likelihood of reporting improvement/cure was high (OR 2.02). Despite the large effect sizes and high OR, these findings are limited by the very-low-to-low GRADE quality of the included studies. Additionally, nearly all pooled data exhibited substantial heterogeneity across the included studies, likely due to variability in the diagnostic criteria for SUI or in the devices used for BF. Therefore, the true magnitude and potentially the direction of these effects remain uncertain. 56 Moreover, invasive BF-assisted PFMT appeared to enhance QoL45,49 and reduce the severity of UI symptoms.27,43,48,54 The effect size was large for QoL (SMD −1.10) and small to medium for the severity of urinary symptoms (SMD −0.33). However, these results should be treated with caution because either the meta-analysis was based on a small number of studies or the mean estimate of the effect was not large. Additionally, the results for this intervention were based on studies associated with moderate-to-high RoB, particularly in domains such as outcome measurement and allocation concealment. These limitations may have introduced systematic errors and compromised the reliability of the pooled results. Overall, the evidence for invasive BF-assisted PFMT in women with SUI remains inconclusive. Additional adequately powered and high-quality studies are warranted to confirm its effectiveness for women with SUI.
Analysis of data from the included studies revealed significant effects of invasive BF-assisted PFMT with ES on the improvement/cure rate, the severity of urine loss, QoL, PFM strength, and the severity of urine symptoms. However, these results were based on data from single studies with low-to-moderate GRADE quality. Therefore, they require replication in additional studies before conclusions can be drawn. In the studies providing evidence for the effect of BF-assisted PFMT with ES, invasive BF with ES was provided via an intravaginal probe. A Cochrane review reported that intravaginal probes caused adverse effects, including pain or discomfort and reactions to the lubricant used with the device. 57 In addition, intravaginal probes are contraindicated for women with menopause-related vaginal dryness or atrophic vagina. 58 Five of the included studies27,43,49,51,54 reported that invasive BF caused adverse reactions such as yeast infection, undefined pain and discomfort, bacterial vaginosis, vaginal irritation, and skin lacerations. Given the reported adverse events associated with intravaginal probes and their suitability for menopausal women with SUI, the clinical benefit and acceptability of this approach remain uncertain. This review found limited evidence in the included studies for the effectiveness of non-invasive BF for treating SUI in women. Therefore, we recommend that more studies evaluate the effects of non-invasive BF to further explore its potential benefits for women with SUI and its potential as an alternative to invasive BF via intravaginal probes.
Our meta-analyses revealed that non-invasive BF-assisted PFMT had superior benefits compared to the control condition in reducing the severity of urine loss, as measured using the pad test. However, these results were based on two studies47,54 of moderate RoB and low GRADE quality, which exhibited substantial heterogeneity. Therefore, this finding should be considered cautiously. Future studies with high methodological rigor are required to confirm the effectiveness of non-invasive BF-assisted PFMT for reducing the severity of urine loss in women with SUI. Nonetheless, the effect size was large (SMD –1.23), and given the safety of non-invasive devices,47,54 non-invasive BF-assisted PFMT may be considered in the clinical management of SUI in women.
Our findings are consistent with a recent systematic review and meta-analysis by Wu et al., which evaluated BF for treating SUI in women. 19 Their meta-analysis included 21 studies and revealed significant effects of BF-assisted PFMT on the improvement/cure rate, with a large effect size (OR 4.82). 59 Similarly, our meta-analysis revealed a large effect (OR 2.12) for this intervention on the improvement/cure rate. Wu et al. 19 also reported significant effects for BF-assisted PFMT on QoL, as measured using the I-QOL, whereas our meta-analysis revealed a nonsignificant effect on this outcome. These differences likely reflect the number of studies included in each meta-analysis for each outcome.
Current systematic reviews and meta-analyses on this topic have failed to reach a consensus on the most effective exercise parameters for BF-assisted PFMT. 22 The treatment parameters, such as the type of contraction (fast, slow, maximum, or sustained), number of repetitions per session, frequency of sessions per week, total duration of treatment sessions, exercise position, and BF equipment utilized, varied considerably among the included studies, limiting the general applicability of our findings to clinical settings. In our study, meta-regression analyses were conducted to investigate how study design characteristics and intervention parameters impact treatment effects. Significant RCs were observed for exercise duration, treatment adherence, and exercise position in improving treatment effects, from which optimal parameters could be derived. The lack of significance for the other variables might be due to the small number of participants in the included studies, the different parameters or methods used in the BF treatment, or the failure of investigators to adhere to standard instruction guidelines for BF-assisted PFMT. Therefore, additional studies are needed to explore and standardize the optimal parameters and treatment processes for BF-assisted PFMT with or without ES.
Our study had several strengths. First, it is the first to employ meta-regression to determine the effective treatment parameters for improving the improvement/cure rate among women with SUI. Second, it employed a comprehensive search strategy that used relevant terms to identify RCTs that evaluated the effectiveness of BF-assisted PFMT with or without ES on SUI in women. Third, it employed a robust and systematic methodology to evaluate the included studies. Finally, the included studies had been conducted in numerous countries worldwide, including both middle- and high-income countries, providing widespread representation.
However, our study also had some limitations. First, the evidence level of most of the included studies, as assessed using the GRADE approach, was low, and their RoB, as assessed using the Cochrane RoB 2 tool, was moderate to high. Second, the degree of UI, differences in body mass index, menopausal status, and parity of the enrolled patients may have affected the homogeneity of the included studies. Third, the low methodological quality, high heterogeneity, and variation in the implementation of intervention protocols and BF modalities across the included studies may have affected the overall estimation of the effect, limiting the generalizability of the conclusions. Finally, only studies published in English and Chinese were considered for inclusion, which may have introduced language bias.
Conclusion
Invasive BF-assisted PFMT is beneficial for improving PFM strength, enhancing QoL, reducing the severity of urine loss and UI symptoms, and increasing the improvement/cure rate in women with SUI. However, our findings must be interpreted cautiously due to substantial heterogeneity across the included studies, as well as their fair-to-good methodological quality, very-low-to-moderate GRADE quality, and low-to-high RoB. Future, adequately powered, high-quality studies are needed to confirm the effectiveness of invasive BF-assisted PFMT for treating SUI in women, as supported by this systematic review and meta-analysis. Our findings support the beneficial effects of invasive BF-assisted PFMT with ES on PFM strength, QoL, the severity of urine loss, the improvement/cure rate, and the severity of UI symptoms. However, since these findings were based on data from single studies, they require replication in other large studies. Our findings also support the beneficial effects of non-invasive BF-assisted PFMT on the severity of urine loss in women with SUI. However, since these findings were based on a small number of studies (n = 2) with substantial heterogeneity, they must be considered cautiously. Analyses of data from single studies support the beneficial effects of non-invasive BF-assisted PFMT on QoL, PFM strength, the severity of UI symptoms, and the improvement/cure rate in women with SUI. Importantly, the evidence for the effectiveness of non-invasive BF-assisted PFMT was derived from studies with good methodological quality, low-to-moderate GRADE quality, and moderate RoB. However, more rigorous, high-quality studies that adhere to the Consolidated Standards of Reporting Trials (CONSORT) guidelines are required to provide a definitive answer on the effectiveness of non-invasive BF-assisted PFMT for SUI in women. Based on our findings, BF-assisted PFMT for women with SUI should involve mildly challenging exercises tailored to the patient’s abilities, performed under the supervision of a therapist during sessions lasting less than 10 min, for more than 1 h/week for at least 8 weeks, with a minimum of 80%–95% adherence.
Supplemental Material
sj-docx-1-tau-10.1177_17562872251406946 – Supplemental material for The effectiveness of invasive and non-invasive biofeedback-assisted pelvic floor muscle training with or without electrical stimulation for the treatment of stress urinary incontinence in women: a systematic review with meta-analysis and meta-regression of randomized controlled trials
Supplemental material, sj-docx-1-tau-10.1177_17562872251406946 for The effectiveness of invasive and non-invasive biofeedback-assisted pelvic floor muscle training with or without electrical stimulation for the treatment of stress urinary incontinence in women: a systematic review with meta-analysis and meta-regression of randomized controlled trials by Shirley Zhaoxue Liu, Mohammed Usman Ali, Mohammad Jobair Khan, Gladys Cheing and Priya Kannan in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.