
Abstract
Background:
The clinical utility of preoperative mid-stream urine culture (MSUC) in predicting fever and urinary tract infections (UTIs) after suction-assisted mini-percutaneous nephrolithotomy (SM-PCNL) remains debated.
Objectives:
This study aims to evaluate the correlation of postoperative fever and UTIs following SM-PCNL in patients with a positive preoperative MSUC versus those with a negative culture.
Design:
This was a retrospective analysis of a prospectively collected registry including 693 patients from the international STUMPS registry (30 centers and 21 countries).
Methods:
Patients were stratified by preoperative MSUC results. All positive cultures were treated with targeted antibiotics for ⩾5 days as per the antibiogram; repeated negative cultures before surgery were not mandatory. Intraoperative parameters, 30-day postoperative complications, and stone-free rates (SFR) were evaluated. Multivariable logistic regression was performed to assess independent predictors of infectious complications.
Results:
Clavien-Dindo grade 1 postoperative fever occurred in 10.6% of patients with positive MSUC versus 4.6% in those with negative cultures. Clavien-Dindo grade 2 infections were more frequent in MSUC-positive patients (4.9% vs 1.2%). Sepsis requiring intensive care occurred in one patient per group. There was no difference in stone compositions and equivalent distribution of infectious stones in both. Intraoperative pelvic urine cultures were more frequently positive in patients with positive MSUC (5.7% vs 0.9%, p < 0.001). No differences were observed in major complications or SFR at 30 days. A positive preoperative MSUC was the only independent predictor of postoperative infection (OR 3.04; 95% CI 1.48–6.12; p = 0.01).
Conclusion:
Positive preoperative MSUC is independently associated with a higher risk of postoperative fever and UTIs, particularly Clavien-Dindo grade 1 and 2 events, following SM-PCNL. Furthermore, these patients are more likely to have a positive intraoperative urine culture. Therefore, a preoperative MSUC should always be obtained, and a targeted antibiotic therapy should be administered irrespective of stone composition to reduce postoperative infectious risk.
Plain language summary
Kidney stones can cause pain and infections. A common treatment for large kidney stones is a procedure called suction-assisted mini-percutaneous nephrolithotomy (SM-PCNL), which removes stones through a small incision in the back. Even though it is less invasive, some patients develop infections after the surgery. Doctors often check a patient’s urine before surgery to see if there are bacteria that could cause infection. This test is called a mid-stream urine culture (MSUC). If the test is positive, antibiotics are given before surgery. However, it’s not always clear whether a positive test still means a patient is more likely to get an infection after surgery. In this study, we looked at 693 patients from 30 centers worldwide who had SM-PCNL. We compared those with positive urine cultures before surgery to those with negative cultures. We found that infections after surgery were more common in patients with a positive urine culture—even if they were given the right antibiotics ahead of time. These patients were also more likely to have bacteria in their kidneys during the procedure. Still, the overall success of the surgery in removing the stones was similar for both groups. This study shows that testing the urine before surgery is very important. Even with antibiotic treatment, patients with a positive result are more likely to develop infections. This information can help doctors identify patients who need extra care to reduce the risk of complications after kidney stone surgery.
Introduction
The integration of suction technology in mini-percutaneous nephrolithotomy (SM-PCNL) decreases intrarenal pressure while facilitating better stone removal. 1 Despite its minimally invasive nature, postoperative infectious complications such as systemic inflammatory response syndrome (SIRS) and sepsis occur in up to 10% of cases.2,3 Recurrent urinary tract infections (UTIs), especially in the presence of renal calculi, are a well-recognized risk factor for such complications, 4 presenting a chicken-and-egg situation to urologists. 5 Kidney stones may harbor bacteria within their matrix, releasing pathogens during lithotripsy that may lead to transient bacteremia and infectious complications. 6
Current international guidelines recommend obtaining a mid-stream urine culture (MSUC) and treating any identified infection before surgical intervention for kidney stones.7–9 However, infectious complications can occur even in patients with negative preoperative cultures.10,11 The need to obtain a negative preoperative urine culture is refuted by recent evidence by Zheng et al., who suggest that achieving a negative MSUC before standard PCNL is unnecessary if appropriate targeted antibiotic therapy is administered. 12 Moreover, the value of repeating MSUC after targeted antibiotics is still uncertain, as continued antibiotic use may mask bacteriuria and delay surgery. However, a 7-day targeted treatment is typically sufficient to prevent serious post-surgical infections. 13
Adding suction to PCNL minimizes infection-related complications by reducing intrarenal pressure and accelerating fluid evacuation, which limits pyelovenous and pyelolymphatic backflow, bacteremia, and consequently lowers the incidence of infectious complications.1,14 To the best of our knowledge, data explicitly assessing the role of preoperative MSUC in SM-PCNL in real-world practice are lacking. This study aims to evaluate the incidence of postoperative fever and UTIs in patients undergoing SM-PCNL, with positive preoperative MSUC versus those with a negative culture. The secondary aims were intra- and perioperative outcomes and stone-free rate (SFR).
Materials and methods
The full protocol of the Suction Technology Utility in Mini-PCNL Study (STUMPS) registry has been previously published. 15 The study prospectively enrolled adult patients (⩾18 years) with renal calculi undergoing suction mini-PCNL performed utilizing either a single-use or reusable suction-access nephrostomy sheath (ranging from 14 to 22 Fr), in combination with any lithotripsy energy modality between March and November 2024. Inclusion criteria were age ⩾ 18 years, kidney stone(s) only, suction sheath 14–22 Fr, normal kidney anatomy, a preoperative MSUC, an intraoperative urine culture and a 2 mm slice unenhanced computed tomography (CT) scan using a bone window and with 2 mm slice thickness within 6–8 weeks before surgery and 30 days after the procedure to assess pre-stone burden and post SFR. Patients under 18 years, concurrent ureteral stones, ongoing use of antiplatelet or anticoagulant therapy without suspension, inability to provide informed consent, and patients with missing data were excluded. Thirty centers across 21 countries were involved. The STUMPS registry was approved by the ethical board of the Asian Institute of Nephrology and Urology (protocol number #01/2024), and other centers obtained approval from their institutional review board. All patients signed an informed consent to allow for data collection for the STUMPS registry.
Collected data included patient demographics, stone characteristics, operative details, lithotripsy modalities, surgical duration, complications, presence of residual fragments (RFs), and need for reoperation. A preoperative MSUC was obtained in all patients, and infections were treated with targeted antibiotics based on antibiogram results for at least 5 days. Positive MSUC was defined as bacterial growth ⩾105 colony-forming units per milliliter. Specimens showing mixed flora or polymicrobial growth were considered likely contamination and were not treated with antimicrobial therapy unless accompanied by compelling clinical signs of active urinary tract infection. A repeated negative urine culture was not mandatory before surgery. For patients with single or multiple stones, the largest stone diameter was recorded. The volume of the largest stone (solitary or in multiple stones) was calculated using the ellipsoid formula: length × width × depth × π × 0.167. The Guy’s stone score was also assessed. 16 Antibiotic prophylaxis was administered according to the antibiogram or followed local practices in case of a negative MSUC. Antiplatelet and anticoagulant therapies were discontinued at least 3 days prior to surgery and resumed postoperatively at the discretion of the attending physician. A renal pelvic urine was collected for culture once lithotripsy commenced. The selection of energy source, patient positioning, puncture technique, tract dilation method, sheath size, and exit strategy was determined by the operating surgeon based on their expertise and available resources. Complications occurring within 30 days post-surgery were classified according to the Clavien-Dindo system validated for PCNL. 17 Stone-free status (SFS) was assessed at 30 days by a 2 mm slice thickness, low-dose NCCT scan using a bone window, and categorized as follows:
- Grade A: no RF (100% stone-free; zero residual fragments (ZRF))
- Grade B: a single RF ⩽ 4 mm (relatively stone-free)
- Grade C: a single RF > 4 mm or RFs of any size
For this study, a retrospective analysis of a prospectively collected registry was performed only on patients with the availability of stone composition. Patients were divided into two groups according to the results of preoperative urine culture. Group 1 included patients who had a negative culture, while Group 2 included those who had a positive culture.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 18 The STROBE checklist is available as Supplemental Material.
Statistical analysis
Continuous variables are reported using median and interquartile range, while categorical variables are described using absolute numbers and percentages. To compare both study arms, patient demographics, peri-operative parameters, and 30-day outcomes were compared between the groups using the Fisher exact test or χ2 test for categorical parameters and the Mann–Whitney U test for continuous variables. A multivariable logistic regression analysis was performed to evaluate factors associated with any postoperative infectious complication, with an a priori selection of variables that have been suggested in previous literature to impact postoperative fever and UTIs after PCNL. 19 Predictors are described using odds ratio (OR), 95% confidence interval (CI), and p-values. All statistical tests were performed using R Statistical language, version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was set at a two-tailed p-value < 0.05.
Results
The STUMPS registry enrolled 1707 patients. A total of 693 patients had data on stone composition and only these were included in this analysis, with 570 in Group 1 and 123 in Group 2. Table 1 shows patients’ baseline characteristics. The median age was similar between groups (47 (38–58) years in group 1 vs 48 (37–60) years in group 2, p = 0.39). The proportion of male patients was significantly higher in group 2 patients (49.6% vs 38.8%, p = 0.03). Demographically, groups were well-balanced for proportion of first-time stone formers, diabetic and chronic kidney disease patients, anticoagulant/antiplatelet use, largest stone volume, stone laterality, Guy’s score, Hounsfield units, and previous PCNL. There was a significant difference in body mass index, American Society of Anesthesiologists score, and stone location. Group 1 patients had a significantly lower proportion of patients with congenital anomalous kidneys (4.7% vs 24.4%, p < 0.001). Table 2 shows pathogens isolated at MSUC. Escherichia coli was the most common isolated pathogen (31.7%).
Patient’s baseline characteristics.
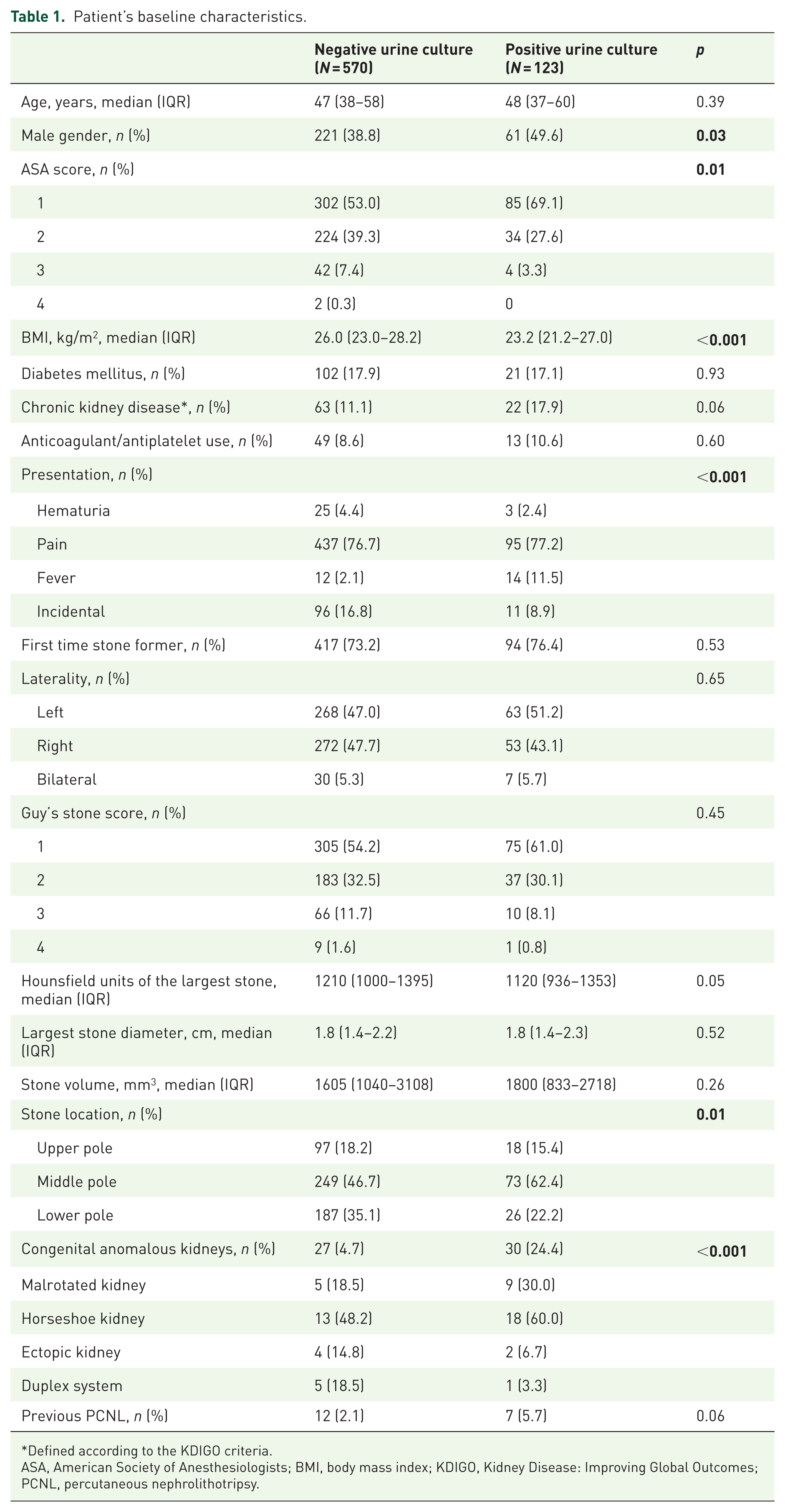
Defined according to the KDIGO criteria.
ASA, American Society of Anesthesiologists; BMI, body mass index; KDIGO, Kidney Disease: Improving Global Outcomes; PCNL, percutaneous nephrolithotripsy.
Isolated pathogens in preoperative mid-stream urine culture.
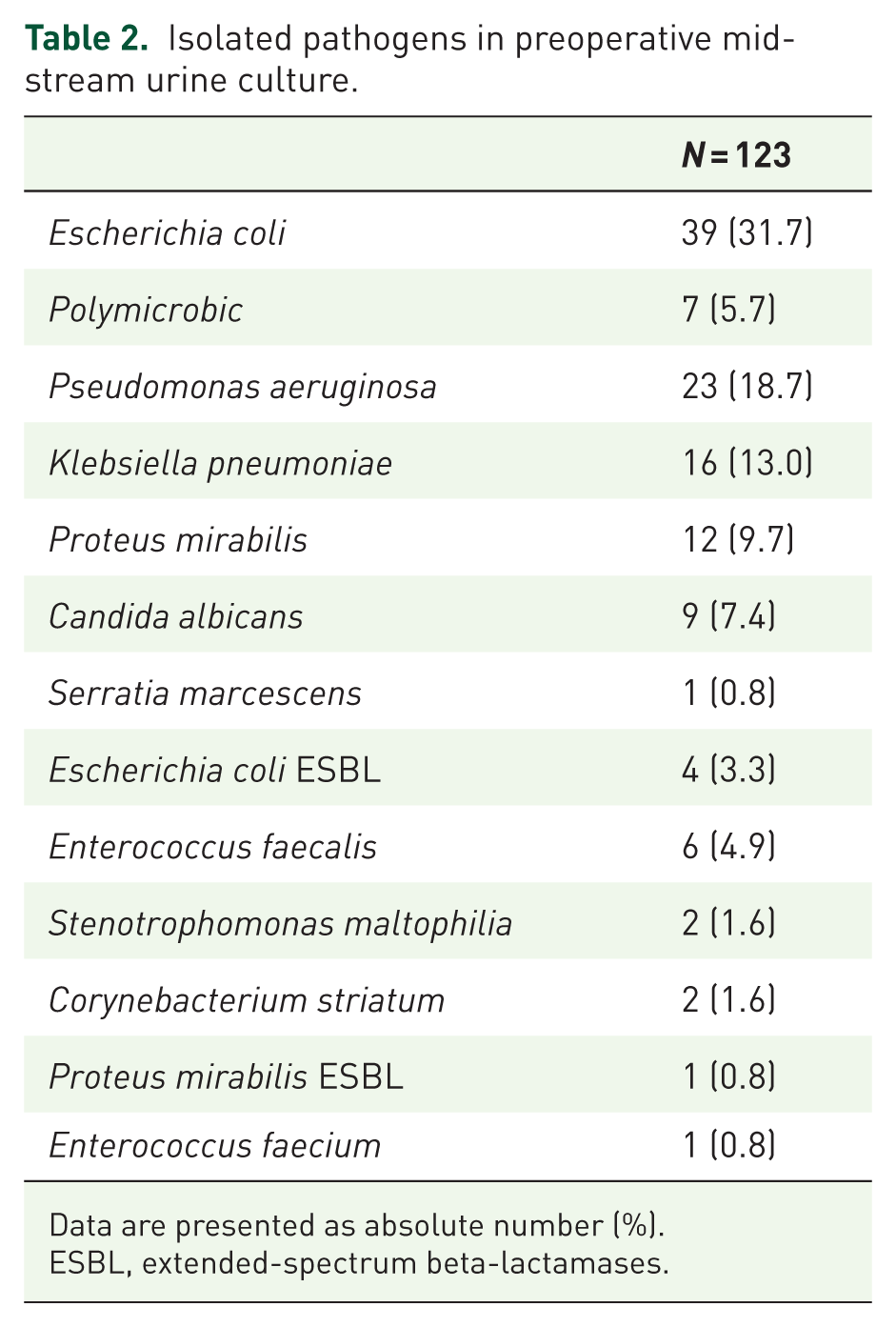
Data are presented as absolute number (%).
ESBL, extended-spectrum beta-lactamases.
Table 3 shows procedural characteristics. A significantly higher proportion of patients in group 2 had surgery under spinal anesthesia (78.0% vs 47.2%, p < 0.001). There was no difference in patient positioning, number of tracts, sheath size, lithotripsy, and stone fragmentation modalities. Significant differences in access technique were noted with higher fluoroscopy-only access to the pelvicalyceal system in 84.6% of cases in group 1 versus 76.4% in group 2. Most patients in both groups had a single access tract (95.6% in group 1 vs 94.3% in group 2) with a similar trend for a supracostal approach (27.7% in group 1 vs 27.6% in group 2, p > 0.99). A significant difference in tract dilation mode was seen with serial dilatation with metal dilators, the preferred modality in group 2 (63.4%), while single-step dilatation was more common in group 1 (41.2%). A ureteral stent was the most common exit strategy in group 1 (45.6%), while the use of a nephrostomy tube and ureteral stent was higher in group 2 (44.6%). A totally tubeless procedure was performed in 1.2% and 0.8% of cases in groups 1 and 2, respectively. Zero fragment intraoperative stone-free status by fluoroscopy and/or visual inspection was seen in 91.0% of cases in group 2 and 86.1% in group 1. Total operation time was significantly shorter in group 2 patients (29 (20–40) min vs 40 (29–70) min, p < 0.001).
Procedural characteristics.

By surgeon confirmed using fluoroscopy or visual inspection.
Table 4 shows intraoperative and postoperative outcomes. The incidence of a positive intraoperative pelvic urine culture was significantly higher in group 2 patients (5.7% vs 0.9%, p < 0.001). The incidence of all complications Clavien 1 and 2 was lower in group1 (9.8% in group 1 vs 14.6% in group 2, p = 0.16) with a similar rate of major complications (i.e., Clavien grade ⩾ 3). The incidence of fever and UTIs was significantly higher in group 2 patients, with only 1 case of sepsis with multiple organ failure needing intensive care management reported (Clavien grade 4b) in each group. No 30-day mortality was reported.
Intraoperative and postoperative outcomes.

CT, computed tomography; RF, residual fragment.
Figure 1 shows the stone composition. The most common stone type was mixed composition in both groups (group 1: 39.0%; group 2: 66.0%), and there was no significant difference in the incidence of struvite stones between the groups (8.4% in group 1 vs 13.8% in group 2, p = 0.09). At 30-day CT scan evaluation, overall stone-free status was similar, and grade ZRF status was reached in 84.7% and 90.2% of cases in groups 1 and 2, respectively.

Proportion of types of stones in the negative and positive urine culture groups.
Multivariable logistic regression analysis shows that a positive preoperative urine culture (OR 3.04 95% CI 1.48–6.12, p value 0.01) was the only factor associated with higher odds of having postoperative fever/UTIs (Table 5).
Multivariable logistic regression analysis of factors associated with postoperative fever and UTIs.

UTI, urinary tract infection.
Discussion
To our knowledge, this is the first multicenter global prospective registry evaluating outcomes in patients with positive pre-op MSUC versus those with negative culture in the setting of SM-PCNL Our findings suggest that a positive preoperative MSUC, even when treated with targeted antibiotics, is independently associated with a higher risk of postoperative fever and UTIs following surgery irrespective of stone composition and independent of the status of the renal pelvic urine culture. Patients with positive MSUC indeed experienced more frequent febrile episodes and UTIs than those with negative MSUC, despite similar stone characteristics. Indeed, the number of anomalous anatomies was higher in these patients, but the Guy’s score distribution was similar.
The most common infectious complication was fever with body temperature greater than 38 degrees (Clavien-Dindo grade 1), which occurred in 4.6% of patients with negative MSUC and 10.6% with positive MSUC. Also, febrile episodes requiring antibiotic therapy (Clavien-Dindo grade 2) were more frequent in the MSUC-positive group (4.9% vs 1.2%). These data suggest that even targeted antibiotic therapy provides incomplete protection, confirming that while antibiotic prophylaxis reduces the infection risk in stone surgery, it does not eliminate it. 20 Furthermore, even the addition of suction cannot entirely mitigate the risk of bacteremia. In fact, it is possible that uncontrolled inflow irrigation fluid may worsen the risk of bacteremia if the outflow is not adequately balanced by adequate suction. Clavien Grade 1 cases likely involve short-lasting systemic inflammatory responses due to stone manipulation,6,21 which antipyretics can effectively manage, yet result in prolonged monitoring, delayed discharge, and increased patient discomfort.22,23 The reasons behind more infectious complications in group 2 patients are multifactorial and likely involve the presence of microbial biofilms, difficult to eradicate by standard antibiotic therapy, or the presence of undetected resistant pathogens within the stone or pelvic urine. 24 Our observed fever/UTI rate in patients with negative and positive MSUC was 4.7% and 11.4%, respectively, slightly lower than those reported in the CROES study (8.8% and 18.2% in the Gutierrez et al. 2 The variability in reported rates may be attributed to differences in patient populations, stone characteristics, operative techniques, and definition of UTI used across studies, but might also be associated with the use of suction in our study.
In our study, the incidence of anomalous anatomy, serial dilators being used for access, postoperative use of a nephrostomy tube, and stenting was higher, and these are well-established risk factors for post-op fever and even sepsis. This can account for the fever despite the shorter surgical time and higher intraoperative zero RF status, which mitigates the risk of postoperative fever. Notably, Group 2 patients had more febrile episodes and a higher risk of sepsis, consistent with CROES findings for standard PCNL patients. 2 However, with SM-PCNL in our cohort, CD2 complication rates were much lower (4.9% vs 1%) than in standard PCNL, where post-op fever is notably higher, especially for those with positive urine cultures preoperatively (18.2% vs 8.8%). 2
Notably, sepsis occurred in one patient in each group. Despite the rarity of this outcome, its occurrence in both groups reinforces the idea that preoperative MSUC alone is an insufficient predictor of severe infectious events.25,26 Prior studies have similarly shown poor concordance between MSUC and pathogens found in stone or bloodstream cultures.27–29
It is worth mentioning that, in the present study, patients with positive preoperative MSCU had a significantly higher rate of positive intraoperative pelvic urine cultures than those with a negative preoperative MSUC (5.7% vs 0.9%, p < 0.001), confirming that pathogens can still harbor in the collecting system despite appropriate preoperative antibiotics therapy as stones have bacteria in their matrix that get released in blood stream on lithotripsy. Such findings support the added value of intraoperative cultures, which are important in selecting the right antibiotic in case of postoperative infections.9,25 Indeed, Silvani et al. 30 demonstrated that bacteremia and microbial dissemination into irrigation fluid are detectable during PCNL even in patients with negative preoperative UC. Blood cultures were positive in 16.4% of cases and stone cultures in 37.7%, with 80% concordance between the two cultures, suggesting that pathogens originating from the stone may colonize the irrigation fluid and the bloodstream. Accordingly, the study recommends routine intraoperative cultures from stones and pelvic urine to better assess infection risk and tailor postoperative antibiotic therapy. 30 Two recent meta-analyses also support the notion that both stone and pelvic urine cultures outperform MSUC in anticipating systemic inflammatory events such as sepsis or SIRS following PCNL.31,32 In addition, Yang et al., 33 focusing on patients undergoing tubeless mini-PCNL, reported that a positive intraoperative SC was associated with a 5.09-fold increased risk of postoperative septic shock (OR: 5.09; 95% CI: 1.22–21.16; p = 0.025). Therefore, the pelvic urine culture could be a viable alternative to stone culture when the latter is not feasible. We were also limited by the lack of stone cultures to make any further analysis.
Given the relevance of preoperative MSUC, questions remain whether patients with preoperative positive MSUC should repeat a preoperative MSUC after having received appropriate antibiotic treatment. Such “traditional” policy 34 has recently been challenged by Zheng et al. 12 who showed that as much as 90% of patients with positive preoperative MSUC had negative MSUC 3 days after treatment initiation, thus making it safe to proceed with PCNL 5–7 days after treatment initiation. This said, 10% of patients remained positive, with 57% presenting bacterial variation. Again, positive stone culture was found to be an independent predictor of fever and UTIs. In the present study, we used the Zheng policy, but unfortunately did not check for 3-day MSUC after treatment initiation or before surgery. Nor did we check the emerging systemic inflammatory biomarkers, such as the neutrophil-to-lymphocyte ratio (NLR) or lymphocyte-to-monocyte ratio (LMR), platelet-to-lymphocyte ratio (PLR), or the systemic immune-inflammatory index (SII). Elevated preoperative systemic inflammatory biomarkers have been identified as an independent predictor of SIRS and urosepsis following PCNL, suggesting that integrating them with microbiological and clinical data could enhance perioperative decision-making.35,36 These biomarkers reflect the balance between inflammatory and immune responses, helping predict procedural outcomes. Elevated ratios typically indicate increased systemic inflammation, which correlates with higher complication rates and prolonged operative times of PCNL.
This approach deserves attention, particularly in patients with chronic bacteriuria, namely those in whom a course of antibiotics did not result in urine sterilization. These are indeed expensive tests and perhaps need to be further validated in large-scale studies before they can be part of routine clinical use.
Several limitations of our study should be acknowledged. First, no repeated MSUC was available immediately before surgery, limiting the ability to confirm bacterial clearance/persistence after antibiotic therapy. Second, although renal pelvic urine and stone fragments were sometimes collected for culture, these data were not systematically analyzed, and no subgroup analyses were performed. This represents a missed opportunity to explore microbiological concordance among MSUC, pelvic urine, and stone cultures, and future studies should look at the specific bacterial subtypes and their influence on culture-positive infections in suction mini-PCNL. Similarly, no blood culture data were available, preventing us from evaluating the correlation between bloodstream, urinary, and pelvic infections. Third, although multivariable analysis was conducted, residual confounding due to unmeasured variables, such as operative irrigation parameters or surgeons’ skills, cannot be excluded entirely. A lack of irrigation and aspiration parameters and IRP monitoring is also noted. In addition, even though treatment therapy was initiated as per antibiograms, patient adherence to preoperative antibiotic therapy was not verified, and criteria for postoperative antibiotic administration were not standardized across centers. Moreover, microbiological endpoints were defined based on clinical documentation and intraoperative pelvic cultures, but no antibiotic resistance data were captured. The interval between the end of antibiotic therapy and surgery was not recorded and standardized, which could influence recolonization risk. In addition, the anatomical differences as an independent factor cannot be best assessed due to fewer numbers, but Guy’s score was similar. Interestingly, both groups had similar distributions for sheath sizes, lithotripsy modality, and stone size, and hence these had no bearing on MVA. Notably, while the STUMPS registry’s strength lies in its large, international, multicenter dataset, this could also introduce potential bias. Variations in hospital resources, perioperative protocols, surgical instrumentation, surgeon experience, and patient management strategies across centers can have affected procedure duration and outcomes for different stone complexities and account for unexpected results in this study. Yet, postoperative fever in PCNL, even with SM-PCNL, should not be taken lightly, as this added morbidity can prolong hospital stay, as was seen in our study, and even though we did not assess quality of life, it will definitely negatively impact the same. We also recognize that excluding over 50% of patients from the registry significantly limits the external validity of our results and may introduce selection bias. Finally, the absence of standardized postoperative antibiotic protocols across centers is another limitation that impacts the generalizability of our results, but all centers treated the cultures as per appropriate antibiogram recommendations.
Conclusion
The present study found that a positive preoperative MSUC is independently associated with a higher risk of postoperative fever and UTIs, particularly Clavien-Dindo grade 1 and 2 events after SM-PCNL, even with targeted antibiotic therapy. In addition, patients with a positive preoperative MSUC were more likely to have a positive intraoperative urine culture. Therefore, a preoperative MSUC should always be obtained, and targeted antibiotic therapy should be administered regardless of stone composition to reduce the risk of significant infectious morbidity. Finally, the development of composite scoring systems incorporating these biomarkers with traditional factors (stone burden, anatomy, comorbidities) could create more sophisticated predictive models for personalized PCNL planning and improve overall patient outcomes.
Supplemental Material
sj-pdf-1-tau-10.1177_17562872251400125 – Supplemental material for Positive preoperative urine culture is a predictor of urinary tract infections and fever following suction mini-PCNL: results from a large, multicenter series from the Endourology section of the European Association of Urology and the STUMPS collaborative group
Supplemental material, sj-pdf-1-tau-10.1177_17562872251400125 for Positive preoperative urine culture is a predictor of urinary tract infections and fever following suction mini-PCNL: results from a large, multicenter series from the Endourology section of the European Association of Urology and the STUMPS collaborative group by Angelo Cormio, Daniele Castellani, Bhaskar K. Somani, Khi Yung Fong, Nitesh Kumar, Rajiv H. Kalbit, Ivan Gorgotsky, Sundaram Palaniappan, Yiloren Tanidir, Zelimkhan Tokhtiyev, Lazaros Tzelves, Andreas Skolarikos, Esteban Acuña, Leonardo Gomes Lopes, Dmitriy Gorelov, Jaisukh Kalathia, Amish Mehta, Karl Tan, Pankaj Dholaria, Arun Chawla, Edgar Beltrán-Suárez, Zhu Wei, Thomas R. W. Herrmann, Steffi Kar-Kei Yuen and Vineet Gauhar in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.