
Abstract
Percutaneous nephrolithotomy is the preferred treatment for large renal calculi; however, postoperative hemorrhage is a dangerous complication. The three main causes of hemorrhage after percutaneous nephrolithotomy are pseudoaneurysms, arteriovenous fistulas, and arterial lacerations. The preferred treatment for acute hemorrhage is superselective angioembolization. However, in a few cases, angiography reveals no abnormal findings pertaining to hemorrhage. We herein present a clinical case of a 48-year-old man who presented with multiple complex right renal calculi and was managed with percutaneous nephrolithotomy in the prone position. Massive hemorrhage occurred 6 days postoperatively, and renal angiography was immediately performed. However, while the bleeding was still occurring, no extravasation was observed on renal angiography. We performed retroperitoneal laparoscopic renorrhaphy, which successfully stopped the bleeding and consequently preserved the kidney. We suggest that retroperitoneal laparoscopic renorrhaphy can be effective in patients who have undergone failed renal arterial embolization or are reluctant to undergo renal arterial embolization.
Introduction
Percutaneous nephrolithotomy (PCNL) is now the first-line surgical procedure for treating large, complex upper urinary tract stones.1,2 However, serious postoperative complications such as hemorrhage still occur in some cases. 3 Postoperative hemorrhage occurs in approximately 14% to 24% of patients, and 0.8% of these patients require angiographic embolization or open surgery. 4 Superselective renal arterial embolization (SRAE) is an effective and well-tolerated method for post-PCNL hemorrhage and has a success rate exceeding 80%. 5 However, the initial SRAE for severe post-PCNL hemorrhage fails in some patients, necessitating further surgical treatment. 6 We herein report a case of severe post-PCNL hemorrhage treated with retroperitoneal laparoscopic renorrhaphy following failed initial SRAE. We also discuss the causes of hemorrhage and various management options. This case report informs clinicians that retroperitoneal laparoscopic renorrhaphy can be used in patients who have undergone failed SRAE or are reluctant to undergo SRAE.
Case report
The reporting of this study conforms to the CARE guidelines. 7 A 48-year-old man presented with multiple right renal calculi in the middle and inferior calyces. The calculi had a maximum size of approximately 2.5 cm and maximum computed tomography (CT) Hounsfield units of 1336 (Figure 1). They were managed with PCNL in the prone position using a middle calyceal puncture approach. Target papillary access was achieved using an 18-Fr dilator under ultrasound guidance. The puncture and dilation procedures were uneventful, and a holmium laser was used for lithotripsy. Approximately 20 minutes after lithotripsy, the color of the abdominal drainage fluid became red. The surgery was suspended, and a 16-Fr Foley catheter was inserted as a nephrostomy tube to suppress potential hemorrhage of the renal parenchyma or damaged veins. The nephrostomy tube was clipped and opened after 6 hours. The color of the fluid in the nephrostomy tube and urinary catheter became clear after 3 days. On postoperative day 5, the patient was able to get out of bed, and a CT scan was performed. The CT scan showed that the right nephrostomy tube was in a good position with no blood clots around the kidney or renal pelvis, but some residual stones were present (Figure 2(a)). Four hours after the CT scan, the fluid in the nephrostomy tube and urinary catheter gradually turned red. Eight hours after the CT scan, the patient suddenly felt pain in the lower abdomen, and ultrasound examination showed a bladder hematoma measuring 8 cm. The patient’s hemoglobin concentration was 4.5 g/dL lower than that before PCNL. The bladder hematoma was immediately cleared under general anesthesia using a cystoscope. The patient also received a transfusion of 4 units of blood, and renal angiography was immediately performed. However, no extravasation was observed on renal angiography (Figure 3). The color of the fluid in the right nephrostomy tube and urinary catheter and the progressive reduction in the hemoglobin concentration suggested persistent bleeding. In addition, the hemoglobin monitoring results suggested a progressive decline in the patient’s clinical condition and hemodynamic instability. However, the patient was reluctant to undergo repeat renal angiography.
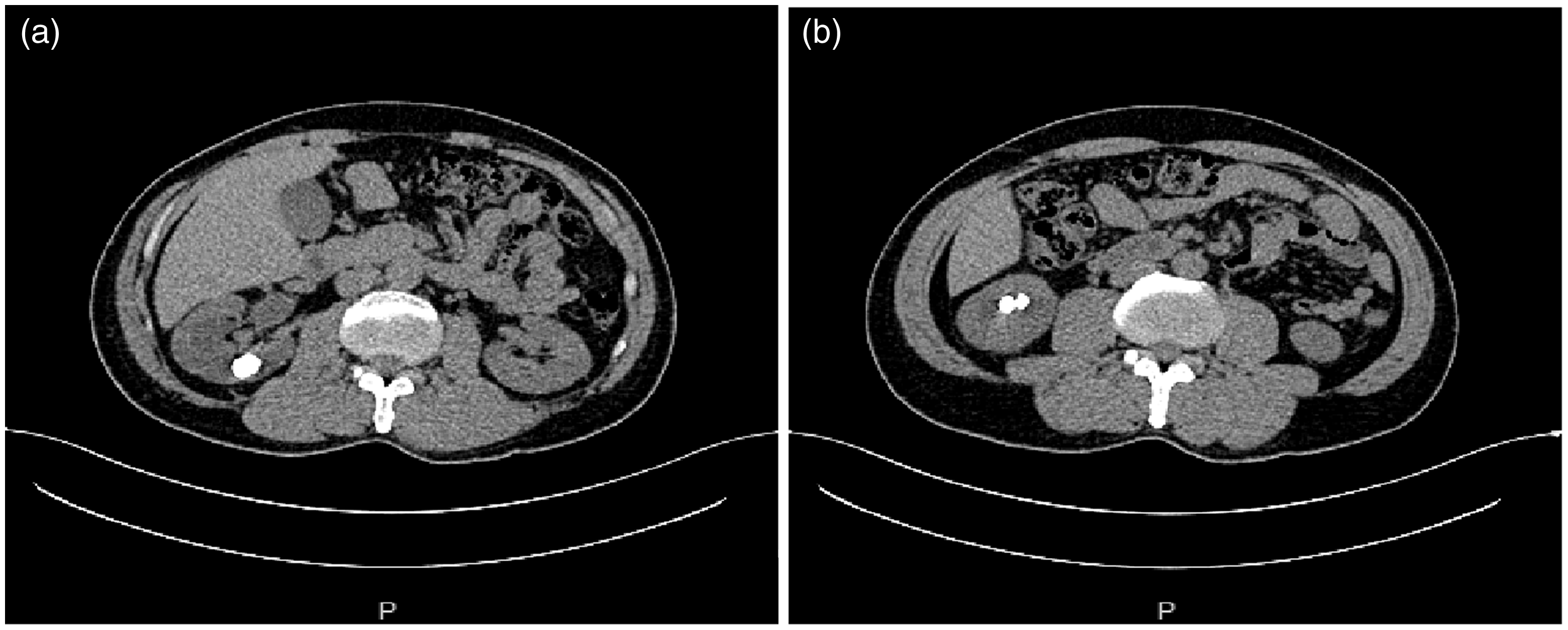
Computed tomography scans showing specific information regarding the calculi. (a) Stones in the middle calyx of the right kidney. Maximum diameter, 2.5 cm; Hounsfield units, 1336 and (b) Multiple stones in the lower calyx of the right kidney.

Computed tomography scans showing the nephrostomy tube and postoperative status of retroperitoneal laparoscopic renorrhaphy. (a) The right nephrostomy tube was in a good position; no hematoma was present, but a residual stone was observed in the renal calyx and (b) Normal kidney morphology after retroperitoneal laparoscopic renorrhaphy.

Right renal angiography. No bleeding spots were found.
After obtaining written consent from the patient, we performed retroperitoneal laparoscopic renorrhaphy to control the bleeding. During this procedure, the patient was placed in the lateral decubitus position under general anesthesia. The retroperitoneal cavity was established using the direct puncture tunnel method. 8 First, we dissected the renal artery to control the bleeding on an emergency basis (Figure 4(a)). The kidney was completely mobilized, and the perirenal hematoma was cleared. The puncture access site was found (Figure 4(b)), the hematoma in the renal pelvis was debrided, and residual stones were also removed (Figure 4(c)). The puncture site was sutured in one full-thickness layer using a 2-0 barbed suture (Figure 4(d)). During suturing, the renal artery was not clamped because of the slow rate of bleeding. The urinary catheter was observed for 10 minutes to check for any significant intrarenal hemorrhage. Finally, a 20-Fr catheter was placed in the retroperitoneum for external drainage, and the retroperitoneal puncture tunnels were closed. During the recovery phase, the patient remained on complete bed rest for 4 days and was closely monitored for any recurrence of bleeding. CT showed good healing (Figure 2(b)), and the patient was discharged after 1 week.

Process of retroperitoneal laparoscopic renorrhaphy. (a) The right renal artery was dissected and suspended by a blue vascular band. (b) The kidney was completely mobilized, and the site of puncture access was found. (c) Calyceal residual stones were found and removed and (d) The puncture access was sutured through a full-thickness monolayer using a 2-0 barbed suture.
Discussion
Severe post-PCNL hemorrhage is a life-threatening complication. 9 Major causes of severe hemorrhage are pseudoaneurysm, arteriovenous fistula, and arterial laceration. 10 Venous bleeding can be controlled using conservative measures. Although the incidence of arterial hemorrhage is low, it can easily lead to hemodynamic instability, necessitating immediate intervention. Huber et al. 11 examined 19 patients with massive hemorrhage requiring SRAE and found that the initial SRAE procedure was successful in 12 patients and unsuccessful in 7 [initial success rate of 63% (12/19)]. Repeat SRAE was performed in six of the seven patients whose initial procedure failed, and of these, SRAE was successful in three patients and nephrectomy was required in three. Zeng et al. 6 reported an initial SRAE success rate of 89.7% and initial failure rate of 10.3%. Among the 11 patients in the failure group, 10 underwent repeat SRAE and 1 underwent nephrectomy.
There are many reasons for failure of the initial SRAE. Zeng et al. 6 reported three risk factors that could lead to failure of the initial SRAE: multiple percutaneous access sites, more than two bleeding sites identified on renal angiography, and use of a gelatin sponge alone as the embolic material. Mao et al. 12 reported that the percutaneous tract size, number of bleeding sites, and vascular aberration/tortuosity were significant predictors of initial treatment failure. They suggested that a repeat SRAE was preferred for patients who experienced initial treatment failure with recurring hemorrhage following PCNL. 12 Some specific types of bleeding also require careful examination, such as subcostal artery bleeding and bleeding in two lumbar arteries after PCNL.13,14 In the present case, there was no obvious arterial hemorrhage on angiography; thus, we considered the possibility of venous bleeding or missed arterial bleeding due to the radiologist’s inexperience. SRAE may fail even if the bleeding sites are found on renal artery angiography. Zhaohui et al. 15 reported that 7 of 37 patients requiring repeat renal arteriography had missed pseudoaneurysms, 7 had recanalization of embolized vessels, and 22 had new renal vascular lesions. Their new findings included pseudoaneurysm, arteriovenous fistula, combination of new pseudoaneurysm and arteriovenous fistula, and no identifiable abnormalities. They believed that the main reason for the failure of SRAE was arterial spasm; progressive deterioration of the injured vessel integrity was another possibility.
Failure of the initial SRAE or unavailability of angioembolization could be devastating for both the patient and surgeon. In failed cases, repeat SRAE may be an option. However, in certain situations, a delay in treatment occurs because angioembolization is prevented by a lack of tools or the patient’s poor condition, such as hemodynamic instability. In addition, the cost of angioembolization may be considered a limiting factor in some hospitals. Surgery is the only option for all patients who have undergone failed SRAE or failed conservative management of bleeding. In this emergency, preserving the kidney is especially important for patients with poor renal function, particularly those with a solitary kidney.
In the current report, we have described the detailed role of retroperitoneal laparoscopic renorrhaphy in such a challenging situation. To the best of our knowledge, this is the first reported case of retroperitoneal laparoscopic renorrhaphy after failed embolization. Aminsharifi et al. 16 reported eight cases of massive hemorrhage after PCNL, and angioembolization either failed or was not feasible. In their cases, partial nephrectomy or renorrhaphy was performed with open surgery, during which the warm ischemia time ranged from 24 to 42 minutes. The renal artery was dissected but not clamped, and the kidney was virtually at zero ischemia during suturing. We believe that the reduction in bleeding may be related to the pneumoperitoneum pressure, and zero ischemia may be an advantage of laparoscopic renorrhaphy over open renorrhaphy. Zero ischemia is vital for preserving renal function, especially in solitary kidneys. In addition, retroperitoneal laparoscopy has the following advantages: a shorter postoperative hospitalization period, less analgesic use, and earlier return to activities of daily life. With respect to the suture method, because the percutaneous renal puncture channel is relatively neat, we believe that it is sufficient to suture the wound in one layer. Aminsharifi et al. 16 used circumferential sutures with chromic 2-0 running sutures in open partial nephrectomy or renorrhaphy. We believe that the hemostatic effect of intraoperative sutures can be determined by observing the color of the fluid in the urinary catheter. In accordance with the principles of kidney injury treatment, postoperative bed rest is also important.
Conclusion
Retroperitoneal laparoscopy is an available option for preserving the kidneys in patients who have undergone failed SRAE or are reluctant to undergo SRAE.
Footnotes
Author contributions
All authors whose names appear on the submission have contributed sufficiently to the scientific work and therefore share collective responsibility and accountability for the results. J.L.: Project development, data collection, and manuscript writing/editing. G.H., S.C., W.Z., and H.Y.: Data collection.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statement
The procedure performed in this study was in accordance with the ethical standards of the institution and with the 1964 Helsinki declaration and its later amendments. The study protocol was approved by the ethics committee of Guang'an People’s Hospital. The patient provided written informed consent for publication of this case report.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fund of the High Quality Development of Guang'an People’s Hospital (grant no. 21FZ013) and the Youth Innovation Project of Sichuan Medical Association (grant no. Q21042).