
Abstract
Mayer–Rokitansky–Küster–Hauser syndrome (MRKH) is a congenital abnormality of sexual development characterized by agenesis of the uterus and vagina. It may be confined to the genital tract (MRKH type I) or be accompanied by abnormalities of the urinary or skeletal systems (MRKH type II). We report a case of an 8-year-old girl who was admitted to the hospital because of a “reducible mass in the left groin.” Upon examination, a mass of about 3 × 2 × 2 cm3 in size was found in the left inguinal region on increasing abdominal pressure, and a left inguinal oblique hernia was diagnosed. The vulva developed normally, and the vaginal vestibule had only a urethral opening but no vaginal opening; abdominal ultrasound revealed that the right kidney was absent, and the left kidney seemed to be fused by two renal cavities; ultrasound of the uterine appendages showed no uterus, and the left and right ovaries were normal; thus, the patient was diagnosed with MRKH type II syndrome. Laparoscopic examination verified the above findings, and it was also found that no obvious fallopian tubes were found around both ovaries. High ligation of the left inguinal hernia was performed to treat the inguinal oblique hernia. When a patient with MRKH syndrome presents with an unexplained inguinal mass, an ovarian or uterine inguinal hernia should be suspected. Early detection of this anomaly will aid in reproductive outcome management and appropriate surgical management.
Plain language summary
This report describes a rare medical case in an 8-year-old girl who was born without a uterus and vagina, a condition known as Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome. She came to the hospital because of a soft, moveable lump in her left groin. Doctors found it was caused by a hernia, where tissue pushes through a weak spot in the belly muscles. Further examinations showed that while her outer genital area looked normal, she did not have a vaginal opening. Imaging tests also showed she had no uterus, her right kidney was missing, and her left kidney appeared unusual—likely formed by two kidney parts fused together. Her ovaries were normal, but doctors could not find her fallopian tubes. She was diagnosed with MRKH type II, which not only affects the reproductive system but also includes kidney and sometimes skeletal problems. Surgery was done to fix her hernia, and her condition will need long-term follow-up, especially as she grows older. This case shows how important it is to carefully check for reproductive and kidney issues in young girls with unusual groin masses or genital differences. Early diagnosis can help with treatment planning and support for future fertility and emotional well-being.
Keywords
Introduction
Mayer–Rokitansky–Küster–Hauser (MRKH) syndrome refers to a syndrome of genital malformation with normal development of female external genitalia but abnormal development of the Müllerian duct, 1 characterized by congenital dysplasia of the uterus and upper part of the vagina (2/3), but normal development of secondary sexual characteristics and normal 46,XX karyotype. 2 There are two types of MRKH syndrome: Type I (simple form), characterized by congenital absence or underdevelopment of the uterus and vagina, and Type II (complex form), which is also associated with abnormalities in the urinary and skeletal systems in addition to uterine and vaginal anomalies. 3 It is estimated that MRKH syndrome occurs in 1 in 5000 female newborns.4,5
Recent studies have identified defects in genes involved in the development of the mesoderm and its derived structures as the genetic cause of MRKH syndrome. 6 MRKH syndrome was previously considered a sporadic malformation, but the increase in the number of familial cases and the association with chromosomal rearrangements suggest that genetic factors may play a key role in the syndrome. 7 Numerous researchers have detected promising genetic variants associated with MRKH syndrome, including deletions at 17q12 (LHX1, HNF1B) and 16p11.2 (TBX6) and sequence variants in GREB1L and PAX8.8–10 Inguinal hernia is the most common hernia, but it is uncommon in women. 11 The inguinal hernia sac usually contains the omentum, appendix, and bladder. 12 In ovarian hernia, congenital genitourinary malformations of the fallopian tubes and uterus should be considered, such as MRKH syndrome and Müllerian duct malformation. 12
In this study, we reported an extremely rare case of simultaneous presentation of MRKH syndrome, left inguinal hernia, and left renal fusion with malrotation, and reported our experience in the diagnosis and treatment of such conditions.
Case presentation
The patient was an 8-year-old 2-month-old girl who was admitted to the hospital because of “discovery of a reducible mass in the left groin.” The parents were not consanguineous and had no history of genetic diseases. Four years ago, the child had a mass in the left groin area. The mass appeared intermittently and was soft in texture. The mass disappeared on its own after sleep and rest. Since then, the mass has recurred repeatedly and become more obvious during exercising or increased intra-abdominal pressure. The patient denied a history of incarcerated hernia. The outpatient clinic suspected “left inguinal oblique hernia” and recommended hospitalization for treatment (Supplemental Material).
After physical examination, a mass was found in the left groin area when abdominal pressure was increased. The mass was soft in texture, with clear boundaries, no tenderness, and could be retracted into the abdominal cavity with light pressure. Abdominal ultrasound revealed a left ovarian hernia; the left ovary was probed at the inner ring opening, showing a size of about 2.6 × 1.4 × 1.3 cm3, with no obvious abnormality in shape, clear boundaries, and no abnormality in the right ovary (Figure 1). No abnormalities were found in the right groin area. The patient’s vulva developed normally, the vaginal vestibule only had a urethral opening but no vaginal opening, and no abnormalities were found in the anus. The patient’s chromosome karyotype was 46,XX (Figure 2). The urinary system involvement was then examined. Abdominal ultrasound revealed that the right kidney was absent; the size of the left kidney was about 9.2 × 3.0 cm, the renal membrane was intact, and it seemed that two renal cavities were fused, with the renal hilum facing upward (Figure 3). This indicated that the left kidney was fused and rotated poorly. Ultrasound of the uterine appendages revealed that the bladder was well filled, the mucosa was continuous and smooth, and the uterus was not seen behind the bladder (Figure 4). Therefore, it was diagnosed as MRKH type II syndrome. To treat the inguinal hernia, we performed laparoscopic surgery. Laparoscopic-assisted exploration showed that the left inguinal canal was not closed, the left ovary was located in the left inguinal canal, and it could be retracted into the abdominal cavity after traction. No uterus was found in the pelvic cavity (Figure 5(a)). The right ovary was located in the right paracolic groove, the right inguinal canal was closed, and no obvious fallopian tubes were seen around both ovaries (Figure 5(b)). The left ovary was dragged out to the abdominal cavity, and a high ligation of the left inguinal hernia was performed. During the 1-year follow-up, the child had no recurrence of inguinal hernia and no complications.

Abdominal ultrasound revealed a left ovarian hernia, and the horizontal line was the transverse diameter of the internal ring opening.
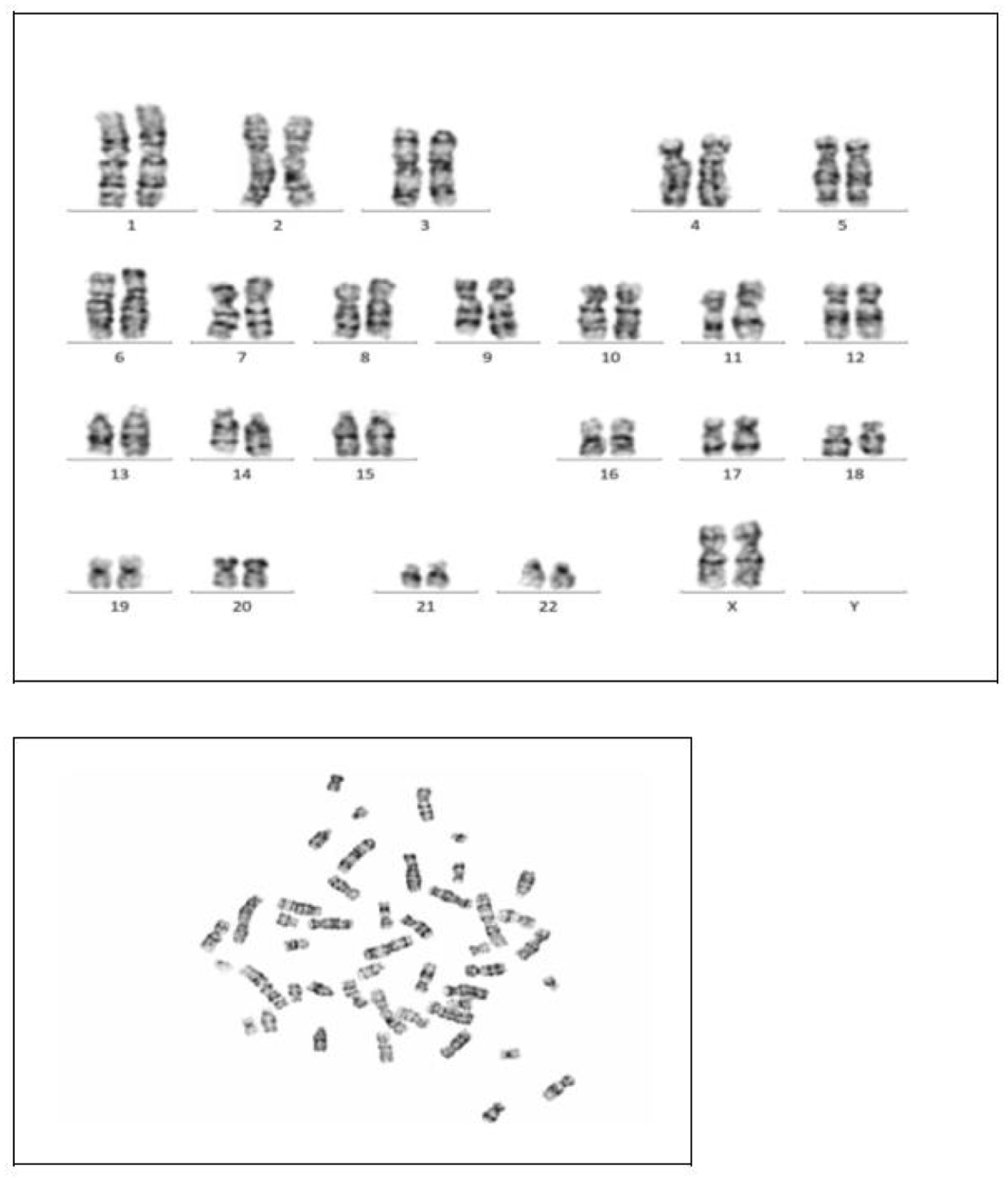
Chromosomes of the patient.

Abdominal ultrasound. Left: the arrow points to the renal hilum, where the renal blood vessels enter and exit the kidney, toward the upper and outer sides. Right: the arrow points to the fused renal notch.

Uterine appendages ultrasound. No uterus was found behind the bladder. Left: transverse section of bladder and Right: longitudinal section of bladder.

Laparoscopic surgical findings. (a) The left ovary has no oviduct and fimbriae of the uterine tube, and herniates into the left inguinal canal, dragging it out of the left inguinal canal and (b) the right ovary, without the oviduct and fimbriae of the uterine tube.
Discussion
As renal fusion with malrotation is usually asymptomatic, its diagnosis remains difficult without the use of imaging techniques. Rather than being diagnosed incidentally, MRKH syndrome is most often identified in adolescence following clinical evaluation for primary amenorrhea, which is usually the first noticeable symptom. Inguinal hernias are rare in females and are commonly seen in children with congenital developmental abnormalities. In this study, we reported an extremely rare case presenting with MRKH syndrome, inguinal hernia, left renal fusion, and malrotation. We aimed to highlight the rarity of this disease and share our experience in its diagnosis and treatment.
The primary diagnostic tool for MRKH is imaging, with abdominal ultrasound as the initial test and magnetic resonance imaging (MRI) of the abdomen and pelvis providing more detailed information. 13 However, in general, ultrasound is less adept at observing detail and observing the location of ectopic ovaries when diagnosing MRKH.14,15 Several other diagnoses have been shown to mimic MRKH syndrome. Vaginal agenesis is occasionally misinterpreted as an imperforate hymen or transverse vaginal septum, with ultrasound demonstrating a proximal vaginal cavity and possible hematocolpos. This misinterpretation can have unfortunate iatrogenic consequences. 16 The diagnosis is often made during adolescence, a time of sensitive physical/emotional development and vulnerability, which further heightens the provider’s concern and awareness of the patient’s emotions, reactions, and coping strategies. 17 Healthcare providers can influence young women’s understanding of MRKH syndrome by using inclusive language and emphasizing all aspects of normal functioning. 18 Early diagnosis of MRKH syndrome may aid psychological support and treatment planning, but can also cause emotional stress in adolescents. It should be approached with consideration of the patient’s maturity and individual needs. 19 In this study, we performed abdominal ultrasound and uterine adnexal ultrasound on the patient and finally diagnosed her with MRKH syndrome. Preoperative imaging and meticulous surgical technique are essential to avoid misdiagnosis, missed diagnosis, or the need for repeat surgery.
MRKH type II syndrome is characterized by abnormal development of the vagina, uterus, and, along with kidney, skeletal, and cardiac malformations.14,20 Associated upper urinary tract malformations were found in approximately 40% of MRKH syndrome cases. 21 The main ones include unilateral renal agenesis (23%–28%), unilateral or bilateral renal ectopia (17%), renal dysgenesis (4%), horseshoe kidney, and hydronephrosis.3,22 In addition, a case of bilateral renal agenesis associated with uterine and fallopian tube absence has been reported in a fetus aborted by medical means, 23 reinforcing the idea that Müllerian agenesis may be an additional manifestation of inherited renal agenesis in some cases. 24 Genetic case studies have found that 17q12 deletions appear to be associated with a subset of MRKH syndrome patients with or without renal disease. 25 Other promising genetic variants associated with MRKH syndrome include deletions and variants at 16p11.2 (TBX6), 26 1q21.1 (RBM8A), 27 2q13q14.1 (PAX8), 28 and GREB1L, 29 indicating that the causes of MRKH syndrome are diverse and involve multiple genes. Only conventional karyotype analysis was performed in this case, and no abnormalities were detected. As chromosomal microarray analysis was not conducted, the presence of copy number variations (e.g., 17q12 microdeletions) cannot be excluded, which represents a limitation of this study. In this context, our patient presented with uterine and vaginal agenesis and left renal fusion with malrotation, which is a typical example associated with MRKH type II syndrome.
Hernia is one of the common surgical diseases, which can be divided into abdominal wall hernia and inguinal hernia. The incidence of inguinal hernia in children is relatively high, and most of them are oblique hernias. 30 The present case represents a rare co-occurrence of MRKH syndrome and ovarian hernia. While inguinal hernias involving pelvic reproductive organs are uncommon in MRKH patients, they have been documented. Most reported cases involve herniation of rudimentary uteri,31,32 whereas our case uniquely features herniation of the ovary. Previous studies have suggested that genital hernia structures may be related to incomplete fusion or abnormal fixation of the Müllerian duct. 33 In addition, weak or abnormal development of ovarian ligaments may partly explain the presence of inguinal hernias.34,35 Another theory suggested that weakness of the broad or ovarian ligament and increased intra-abdominal pressure lead to herniation of the ovary into the inguinal canal. 36 Increased intra-abdominal pressure, such as from heavy lifting or chronic straining, may act as an aggravating factor. This case reinforces the importance of considering genital hernia in MRKH patients presenting with groin swelling or pain. Early diagnosis and surgical intervention are essential to preserve ovarian function and avoid complications such as torsion or infarction. Compared to previously reported uterine inguinal hernias, 31 this case adds to the phenotypic spectrum of MRKH-associated inguinal hernias and underscores the need for individualized evaluation and management.
Surgery is an effective method for treating inguinal hernia in children. 37 The traditional surgical method is high ligation of the hernia sac under a small incision, which is very harmful to children and is gradually replaced by new surgical procedures, such as laparoscopic minimally invasive high ligation of the hernia sac. Thanks to its visualization characteristics, the operation site is changed from intra-abdominal to extraperitoneal, which reduces the surgical risk and is more conducive to intraoperative operation. In addition, laparoscopic technology can be used to explore the uterine appendages, which have an auxiliary role in the diagnosis of MRKH.
Conclusion
MRKH type II syndrome should be considered in patients presenting with genital tract hypoplasia and associated anomalies of the extragenital system. Although several candidate genes and chromosomal deletions have been implicated, the genetic basis of MRKH syndrome remains incompletely understood. Early recognition through imaging and laparoscopy remains the cornerstone of diagnosis and is essential for guiding multidisciplinary management, providing psychological support, and preserving organ function in complex cases such as those involving coexisting inguinal hernias.
Supplemental Material
sj-pdf-1-tau-10.1177_17562872251398912 – Supplemental material for Mayer–Rokitansky–Küster–Hauser syndrome with inguinal hernia, left renal fusion, and malrotation: a rare case
Supplemental material, sj-pdf-1-tau-10.1177_17562872251398912 for Mayer–Rokitansky–Küster–Hauser syndrome with inguinal hernia, left renal fusion, and malrotation: a rare case by Chuanxin Li, Hang Yang, Han Xiao and Jianhong Yan in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.