
Abstract
Objective
Laparoscopic ports have been used in many surgical procedures. Trocar-site hernias are a unique complication in laparoscopic surgeries. Closing the trocar-site defect could be an essential part of trocar-site closure for preventing trocar-site hernia formation. We report a new, simple, and safe-to-perform technique to close port-site wounds. This easy-to-manipulate tool only requires a balloon catheter and involves a safe procedure.
Methods
In this retrospective study, 55 port-site closure cases (54 cases of laparoscopic inguinal hernias and 1 case of appendicitis) were enrolled from January 2022 to July 2024 in the Department of Hernia Surgery at the First Affiliated Hospital of Yangtze University. An inflatable balloon catheter was used in the upward direction to lift the peritoneum fascia after the skin and subcutaneous tissue were retracted with a right-angled retractor. The trocar site was closed under direct vision, and no complications were reported.
Results
The trocar-site closure technique was used in 55 port sites among 54 patients, and no adverse events occurred. Only a balloon catheter was required, and no additional tissue trauma was reported. This technique is easy to learn and manipulate. No trocar-site hernia or abdominal organ injury was reported at the median follow-up of 15 months.
Conclusions
The trocar-site closure technique is a simple-to-manipulate, safe, and cost-effective approach.
Keywords
Introduction
Laparoscopic surgery has become a common treatment approach for various hernias worldwide. The small incision size required for laparoscopic surgery and the associated rapid recovery period have been accepted by all surgical specialties. However, the potential complications of laparoscopic surgery have received considerable attention. Among them, trocar-site hernia (TSH) is a complication that should be avoided. The first case of TSH was reported by Fear in 1968 in patients who had undergone gynecologic laparoscopies. 1 The intestine or omentum protruded out of the abdomen through the trocar-site defect. This herniation developed though the defect of the trocar site at the peritoneum fascia. Port-site hernia and TSH are often reported in the literature. 2 The incidence of TSH was 0.104% in a retrospective review of 18,533 patients after 23 months of laparoscopic surgery. 3 Karampinis et al. detected an abdominal wall defect rate of 34.5% following bariatric surgery at a mean follow-up duration of 36.4 months. 4 The incidence of TSH varies between 0.15% and 34% in the literature.2,3 The incidence could reach 37% for TSH complications. The estimated incidence of TSHs varies between 1% and 6% following laparoscopic surgery, as reported by Antoniou et al. in 2016. 5 The 5-mm TSH rates were 0.003% following gynecologic procedures and 0.0005% following general surgical procedures. 5 Pereira et al. reported that 86.3% of the 850 TSHs were >10 mm in size. 6 The notable factors of TSHs depend on the characteristics of patients and the surgical technique used by surgeons for trocar-site closure. TSH formation is associated with wound infections, obesity, nutritional status, anemia, and diabetes. 7 Several techniques of trocar-site closure have been employed by surgeons, including endoscopic suturing and specialized devices. 7 However, these methods are complex or expensive. Herein, we present our technique of trocar incision closure with a balloon catheter, especially in challenging cases. The aim of our study was to introduce our trocar-site closure technique and simplify this novel tool based on the reported literature.
Technique description
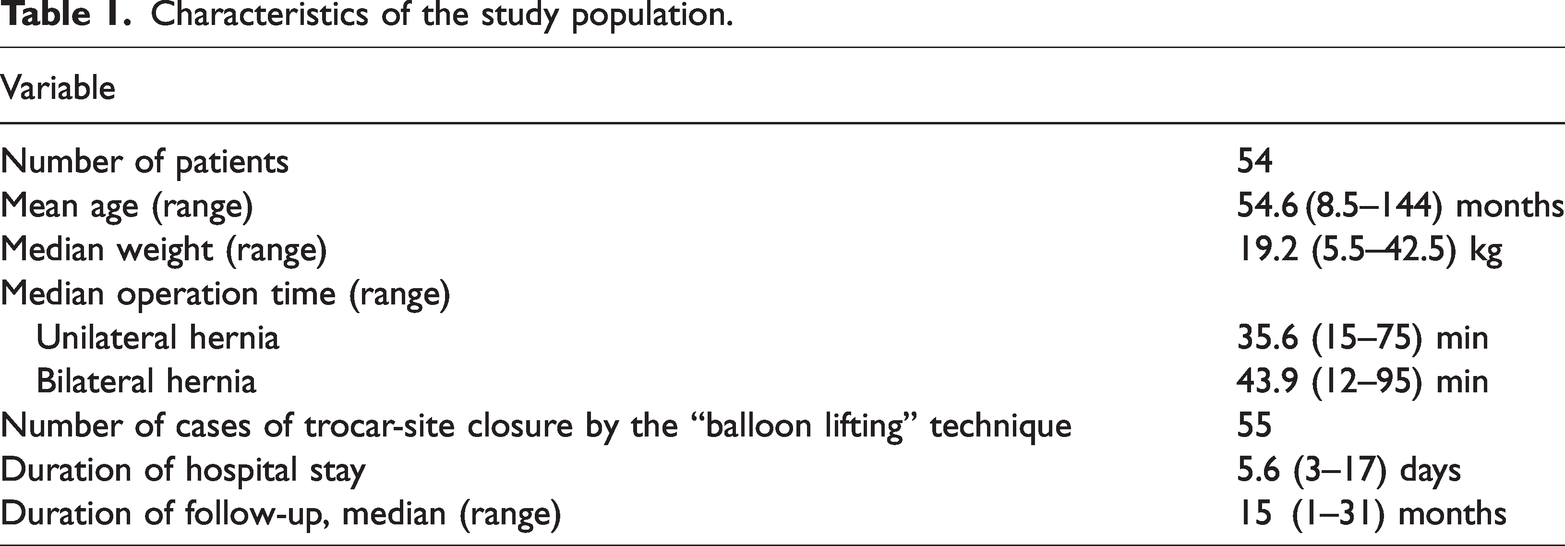
A retrospective study of patients with inguinal hernias or appendicitis was performed by two expert surgeons at the Department of Hernia Surgery of the First Affiliated Hospital of Yangtze University between January 2022 and July 2024. This study was approved by the Ethics Committee of the Hospital (No. 2023HC95). Written informed consent was obtained from all study participants. The research conformed to the principles of the Declaration of Helsinki. We de-identified all patient details. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 8 The patients were selected consecutively (Table 1). Standard surgery equipment was required. All procedures were performed under standardized general anesthesia. A specifically designed 14-Fr ureteral balloon catheter (Double lumen catheter standard version, Model: 4.7 mm(14-Fr), 30 mL) was utilized. Before deflating the pneumoperitoneum, the catheter was inserted into the peritoneal cavity under direct laparoscopic visualization (Figure 1). Under laparoscopic monitoring, a surgeon slowly injected exactly 30 mL of air using a calibrated syringe to achieve spherical balloon expansion (Figure 2). Critically, the balloon volume was titrated until visible tension was observed on the peritoneal surface (range: 30 mL). After retracting the skin and subcutaneous tissue with a standard right-angled retractor, the inflated balloon catheter was gently retracted in the upward direction (direction: 90° toward the patient’s body) to elevate the peritoneal fascia (Figure 3). The mobilized peritoneal edge was secured using atraumatic tissue forceps immediately superior to the balloon (Figure 4). The contralateral peritoneal edge was grasped in a similar manner. The trocar-site defect was closed with 2–3 interrupted sutures of 3-0 absorbable monofilament placed at 5-mm intervals, incorporating the full-thickness peritoneal edge and fascia (Figure 5). The trocar site was closed under direct vision, and no complications were reported.
Characteristics of the study population.

Insertion of a balloon catheter into the peritoneal cavity before deflating the pneumoperitoneum.

Injection of 20–30 mL of air by the surgeon into the ureteral balloon and observation of its spherical expansion under laparoscopic monitoring.

The peritoneal tissue wounded by tissue forceps above the inflatable balloon catheter.

The peritoneal tissue wounded by tissue forceps after removing the inflatable balloon catheter.

Use of 2–3 interrupted absorbable sutures for closing the trocar-site defect.
Results
The inflatable balloon catheter technique was used for closure of 55 trocar sites in 54 patients. The mean body mass index and weight were 15.5 kg/m2 and 19.2 kg, respectively. We did not observe TSH in our patients at the median follow-up of 15 months. Our standard follow-up protocol mandated scheduled clinical assessments, including a thorough physical examination specifically focused on detecting TSH signs and symptoms at defined intervals (e.g. 1 month, 3 months, 6 months, and 12 months after the operation). No clinically evident TSH was detected during the follow-up period (minimum 12 months) based on scheduled clinical assessments, including thorough physical examinations. Targeted imaging (ultrasound or computed tomography (CT)) was performed selectively based on clinical suspicion, and no such suspicion arose in any patient. Currently, we routinely close trocar-site defects using the inflatable balloon catheter technique.
Discussion
TSHs are acknowledged universally as a complication of laparoscopic surgery. The most common contents of TSHs are the intestine or omentum; in rare cases, the appendix, ovaries, or fallopian tubes can be found in TSHs following laparoscopic procedures.9,10 The majority of TSHs occurred within 6 months of laparoscopy surgery. The pathogenesis of TSHs depends on both technical factors and patient-related factors. The major reason for TSH formation is forgotten or inadequate closure of fascial defects. Nonclosure or the absence of tight closure of trocar-site fascial defects as well as some patient-related risk factors such as diabetes, coughing, poor nutrition, immunosuppression, chronic steroid use, older age, and frailty can accelerate TSH formation. 11 The 5-mm TSHs are formed more frequently when bladed trocars are used in surgery compared with when nonbladed trocars are used. 12 Bladed trocars cause a larger defect size than nonbladed trocars. 13 TSHs develop more easily in patients with pre-existing fascial defects. 14
Factors involved in the development of TSHs include trocar location, trocar type and size, manipulation time of operation, and the size of fascial defects. Extensive or prolonged manipulation of the 5-mm trocar port site during surgery is associated with TSH development. 14 Trocar-site fascial closure is affected by factors such as patients’ obesity and surgeons’ skill level. The limited visual field of the trocar site is the key technical difficulty, especially in obese patients with a thick abdominal wall. Researchers recommend that all trocar incisions, including peritoneum fascia incisions, should be closed. Our “balloon lifting” technique makes the peritoneum fascia layer easier to suture. No trocar-site herniation was found in our patients at the 6-month follow-up.
TSHs can cause pain, nausea, and abdominal discomfort in early appearance stages. The size, shape, and location of the trocar are important factors for TSH development. The umbilicus was the most common site of TSHs because it is commonly used as a camera location. 15 Trocars placed along the midline seem to increase the likelihood of TSH formation, even when the linea alba incision is closed. Regarding 5-, 10-, or 12-mm trocar, TSHs were more likely to occur while using bladed trocars than while using nonbladed trocars. 5 Trocars ≥10 mm in adults and ≥5 mm in children should be closed for reducing the risk of hernia.16,17 Hata et al. believed that suturing all layers of the abdominal wall is necessary for preventing TSHs, especially in obese patients. 18 Ota et al. reported that inserting nonbladed 12-mm trocars into the abdominal cavity of pigs at a 45° angle resulted in smaller fascial defects. 9 TSHs also occurred in the 8-mm trocar site after robot-assisted surgery. 19 TSHs formed more easily when the trocar was located in the midline than off the midline. Trocars placed in the linea alba of the abdominal wall, which lacks muscle layers, are more susceptible to TSH formation. 20 TSH is associated with age, duration of surgery, obesity, incision enlargement, wound infection, and diabetes mellitus; thus, peritoneum fascial closure is essential in these patients. Tonouchi et al. classified TSHs into three types: early type, late type, and special type. 21 Early-type hernia usually arises from the dehiscence of three parts of the tissue: anterior fascia, posterior fascia, and parietal peritoneum fascia. Late-type hernia usually develops because of disconnection of the posterior and anterior fascial plane. The special type represents the dehiscence of the entire abdominal wall. 6 In a previous study, closure of the trocar-site defect reduced the incidence of TSH by two-thirds after laparoscopic surgery. 22 The treatment methods for TSHs include fascial closure and omental or partial intestine resection. It is recommended to close trocars <10 mm routinely, especially when risk factors exist. 23 The CT device and EZ port-site closure device are widely used for port-site closure. Kim et al. mentioned these devices took less time for port-site suturing and caused the least complications. 24 The cutanplast plug is used in port-site closure; 25 however, it is challenging to learn. The Versa OneTM fascial closure system (VFCS; Medtronic Japan) offers consistent suture placement for laparoscopic port closure. The VFCS device was complicated and designed to suture the port site using a single suture. 26 However, its consumer price is high and the method is not preferred by our patients. No port-site closure techniques have been adopted in daily surgical practice. The dual-hemostat technique for port closure is an appropriate option in laparoscopy. 27 The advantage of the Chennai port-site closure technique lies in the ability to perform prefabricated sutures without the need for other suturing after removing the port. The port placement should be in the middle point of the prefabricated loop of suture. 28 Lasheen’s port-site closure technique involves tying the thread out of the peritoneal cavity by using the percutaneous transabdominal approach with two looped needles. 29 The heat-induced trocar-site closure technique, which causes shrinkage and collagen denaturation of the fascial and muscle defect, may prevent herniation of the trocar site. 30 A surgical plug and transplanted autologous fat are used as adjuncts for closing the trocar hole. 31 Moreno-Egea described a mini-IPOM with a lightweight mesh, fixed with glue for closing the trocar hole. 32 The IPOM-mesh is then introduced through the trocar on the forceps until the abdominal cavity is reached, where the internal layer opens freely like an umbrella. Fascial closure devices are more expensive and time-consuming and involve complicated methods; moreover, they are associated with a risk of bowel injury during suturing. In fact, surgeons customarily leave the fascia defect unclosed. Trocar-site closure techniques play a key role in preventing trocar-site defect related complications. According to Shaher, 33 there are three categories of trocar-site closure techniques: (a) techniques that require two ports (suturing the pneumoperitoneum defect from inside the abdomen); (b) techniques that require one port (suturing the pneumoperitoneum defect with additional extracorporeal assistance); and (c) techniques that require no port (suturing the pneumoperitoneum defect with or without direct visualization). Some special closure devices are recommended for closing the trocar-site defect, including spinal needle, double-tip needle, tip hole needle, and Carter–Thomason needle. Once the peritoneum is hooked by the Graham’s nerve hook, it facilitates better visualization for the surgeon while closing the trocar-site defect. 34 Our technique is easily performed under direct visualization, and the inflatable balloon catheter is lifted to perform pneumoperitoneum defect suturing under direct visualization. Our technical approach is cheaper and more practical. The inflatable balloon catheter may reduce the risk of bowel injury when the suturing needle penetrates the fascia above the balloon. For obese patients, we should not make the incision longer for closing the fascial defect; instead, we must only lift the balloon straight upward to visualize the peritoneum incision. Our “balloon lifting” technique may be suitable for any trocar-site closure. There are certain limitations in our study. First, 54 patients with hernia and appendicitis were studied; we plan to further study the correlation of the inflatable balloon catheter technique with the incidence of TSHs in a larger patient cohort in the future. Second, our study was a descriptive case series focused on assessing the feasibility of the surgical technique and observational clinical parameters, without hypothesis testing. More inferential statistics will be used in future studies.
Conclusion
With an increase in the use of laparoscopic surgery, TSHs have received increasing attention as a potential complication. This observational study suggests that the inflatable balloon catheter technique for trocar-site closure may offer a simple, safe, and cost-effective approach. Based on our experience, this technique warrants further investigation for broader application in laparoscopic surgeries.
Footnotes
Acknowledgements
Our research was written and conducted by human authors without the use of AI.
Author contributions
Conceptualization: Chuanchang Yin
Data curation: Yu Wang
Formal analysis: Xiaoyan Wang
Methodology: Xiaoyan Wang
Writing—original draft: Chuanchang Yin
Writing—review & editing: Xiaoyan Wang
Consent
Informed consent was obtained from the parents of the participants included in the study.
Data availability
All data generated or analyzed during this study are included in this published article.
De-identified participant data, surgical videos, and analysis protocols are available from the corresponding author (
Declaration of conflicting interests
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or nonfinancial interest in the subject matter or materials discussed in this manuscript.
Ethics approval
Approval was obtained from the Institutional Review Board of the First Affiliated Hospital of Yangtze University. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Funding
No funding was received for conducting this study.