
Abstract
Background:
The direct in-scope suction (DISS) involves a two-way adaptor mounted on a scope to aspirate and irrigate the pelvicalyceal system during flexible ureteroscopy. While integrated suction single-use scopes manage small dust particles effectively, they cannot remove particles >250 µm and are limited by single use.
Objectives:
To evaluate perioperative outcomes of the GLITZ system, a lightweight suction accessory for flexible ureteroscopes, facilitating laser lithotripsy with integrated aspiration.
Design:
Prospective, multicenter study.
Methods:
The GLITZ system, a 100 g trigger mounted on the ureteroscope handle, integrates with an irrigation and aspiration apparatus featuring a flow-regulating sensor. A finger-trigger activates suction, stopping irrigation until released, enhancing visibility and safety by automatically stopping irrigation if blockages occur. The study involved 29 patients (November 2023–April 2024). Procedures were performed using a disposable 7.5 Fr ureteroscope, ureteral access sheath, and thulium fiber or 100 W holmium:YAG laser. Surgeons evaluated ease of use and performance. Stone-free status was evaluated at a 30-day CT scan and classified as follows: Grade A: zero RF; Grade B: single RF not up 2 mm; Grade C: single RF 2.1–4 mm; and Grade D: single/multiple RFs > 4 mm. Data are reported as median and (interquartile range).
Results:
A total of 31.1% of patients were female. The median age was 54 years. Pain was the most common complaint, and 41.8% had multiple stones. GLITZ system showed satisfactory performance in 93.1% of cases, with complete dust aspiration achieved in 62.1%. Device dislodgement occurred in 24.1% of cases. Median operative time was 40 min, achieving postoperative CT at 30 days confirmed Grade A stone-free status in 75.9%. Fever was the most common complication (10.3%), with no sepsis case.
Conclusion:
The GLITZ system in DISS shows effectiveness with a 96.6% stone-free rate (Grade A + B) at 30 days, indicating strong potential for flexible ureteroscopy, though additional studies are needed to optimize flow rates and usability.
Introduction
The direct in-scope suction (DISS) concept was introduced in 2022 using a two-way adaptor mounted to a scope that used the in-scope single channel as a conduit to aspirate and irrigate the pelvicalyceal system (PCS) during flexible ureteroscopy (F-URS). 1 Since then, it has evolved with dedicated integrated suction flexible single-use scopes (SUS) which are now available for the same. These suction SUS are very effective and safe for DISS. 2 In an in vitro study, Madden et al. showed that integrated suction cleared 100% of dust <250 µm and real-time endoscopic clearance rates were significantly faster than just manual aspiration (3.01 g/min vs 0.41 g/min) for dust between 125 and 250 µm. 3 Yet, the limitation of such devices is the inability to remove particles larger than 250 µm. As suction technology, especially using the flexible and navigable suction ureteral access sheath (FANS-UAS), 4 is a proven game-changer compared with traditional UAS, 5 developing new suction techniques is poised to change the field of endourology and kidney stone disease in the future. 6 Indeed, the first clinical trial using the Pusen DISS 7.5 Fr ureteroscope (Zhuhai Pusen Medical Technology Co., Ltd., Zhuhai, Guangdong Province, China) demonstrated good visibility, maneuverability into the PCS, and suction aspiration quality, with excellent operative results. 2 One limitation is that this ureteroscope is single use; hence, the single channel is the inlet of suction and aspiration and is dependent on an external irrigation-aspiration system. Studies are needed to establish its cost-effectiveness. As several techniques develop, 7 it would be practical to have a unified DISS system that has its suction aspiration control and is compatible with any existing reusable or SUS.
This prospective study aims to describe the perioperative outcomes of performing DISS using a new system called the GLITZ system. This system is specifically designed as a lightweight accessory. The GLITZ system is easily mounted and integrated onto the handle of a flexible ureteroscope to facilitate suction and aspiration of dust when connected to its tabletop, portable suction-aspiration apparatus via the scope channel during laser lithotripsy (LL).
Methods
The GLITZ system
The novel GLITZ system (manufactured by Marflow AG, Islikon, Switzerland, and marketed by Biorad Medisys, Bengaluru, Karnataka, India) is a device specially designed for DISS (Figure 1). The GLITZ system has two parts. The lightweight trigger system weighing approximately 100 g (Figure 2) is mounted onto the scope handle, and secured onto the working channel by a locking screw. The trigger has two sets of tubing for irrigation and aspiration (Figure 3) which are, in turn, connected to the suction-aspiration apparatus. The latter has a sensor to regulate the flow rate (Figure 4). The laser fiber is inserted through a separate straight channel of the trigger handle directly into the flexible scope in the usual manner without additional modifications. A finger activation of the trigger (pulled down) initiates suction-aspiration (Figure 3) which cuts off irrigation and release of the same (neutral position) automatically resumes irrigation at the same user-predetermined flow rate (Figure 5 and Video 1). This alternate action is to ensure a safe and user-controlled dynamic mechanism during suction. If there is any blockage of the channel, the trigger mechanism does not work, and irrigation flow is automatically cut off. This in-built safety mechanism not only allows surgeons the opportunity to inspect the system for any malfunction but also to flush out any particles/debris that may get inadvertently lodged into the scope working channel. The tabletop design of the suction-aspiration apparatus specifically allows for easy portability as well as the integrated sand filter collects the filtered dust and fluid into the jar (Figure 6). This closed-loop system prevents water spillage, keeps the entire circuit watertight, and prevents air entry during the procedure to allow for an unobstructed calyceal view for surgeons, especially when the laser is activated. The trigger system should be activated only after LL to aspirate dust and not during LL to allow continuous irrigation of the PCS.
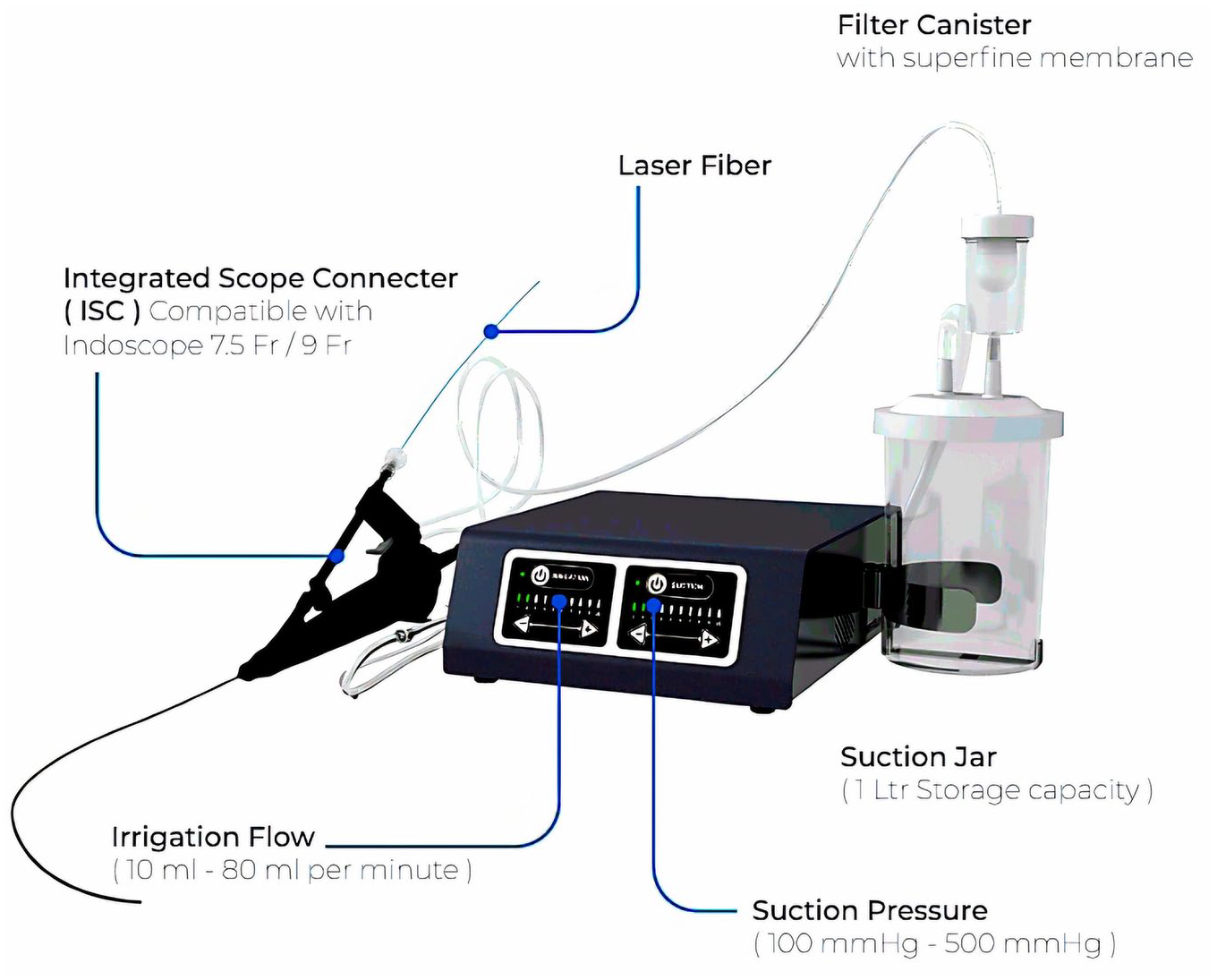
The GLITZ system.

The trigger system.

Tubes for irrigation and aspiration.

The suction-aspiration apparatus.

The peristaltic pump.
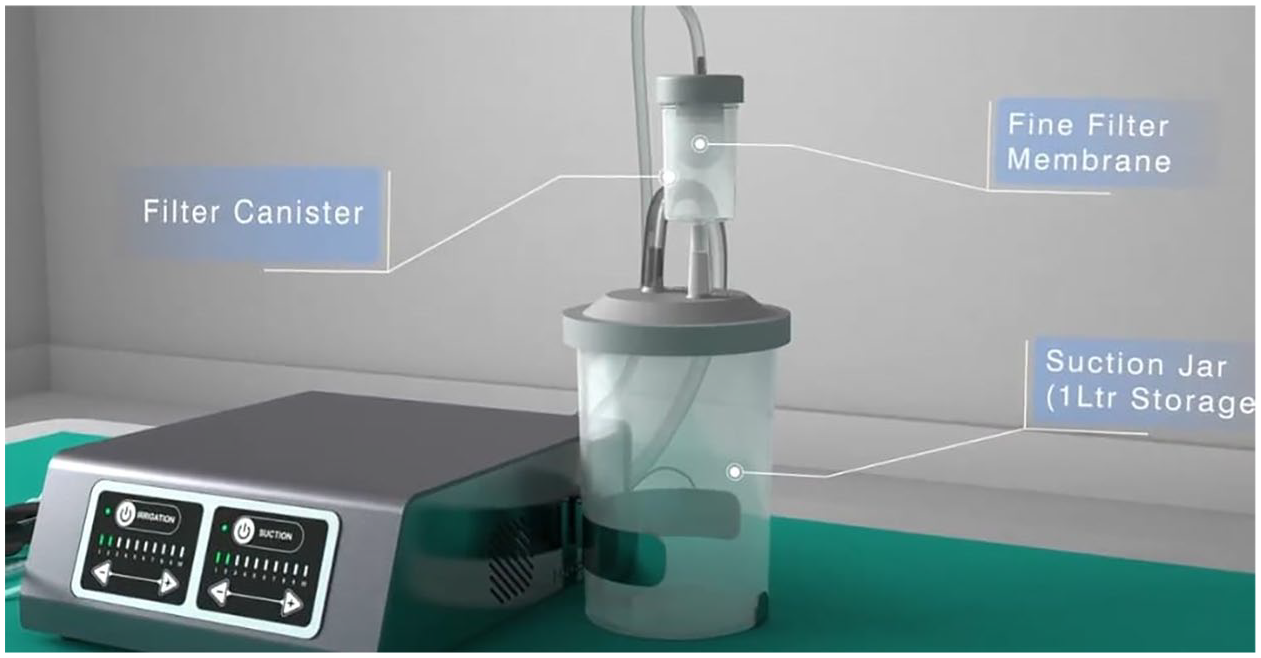
The filter membrane and suction jar.
Study design and patient population
Adult kidney stone patients with normal pelvicalyceal anatomy, capable of providing informed consent, fit for general anesthesia, and deemed suitable for F-URS underwent DISS using the GLITZ system between November 2023 and April 2024 in two centers (Asian Institute of Nephrology and Urology, and Muljibhai Patel Urological Hospital) after obtaining ethic board approval and registration (AINU-EC/28/2023 and FCI 1 017 12021). Exclusion criteria encompassed children/adolescents, ureteral stones, anomalous kidneys, bilateral procedures, and patients unfit for general anesthesia and unwilling to participate. Informed consent was obtained from all individual participants. This manuscript is written following the STROBE checklist (Supplemental Material). 8
Only two senior surgeons (DR and RS) performed all procedures as per the principal investigator and device developer (VG) instructions. All patients in whom the preoperative culture was positive were treated with antibiotics as per the antibiotic sensitivity profile. An extended 3-day antibiotic regimen was given by the surgeon’s personal decision and the patient’s recovery based on a multitude of factors such as preoperative positive culture, history of infection, prolonged surgical time, and suspicion of infected stone. The ureteroscope used for all cases was a disposable 7.5 Fr scope (Indoscope, Biorad Medisys, Bengaluru, Karnataka, India) and a UAS of the surgeon’s own choice. Pre-stenting was not mandatory. Either the thulium fiber laser (TFL) (Urolaser SP, IPG Photonics, Oxford, MA, USA) or a 100 W holmium:YAG laser (HL) (Cyber Ho, Quanta systems, Varese, Italy) was used for lithotripsy. A 200-micron reusable fiber was used with both lasers. Surgeons were asked to evaluate the GLITZ system after each case, scoring it as excellent, very good, good, average, or difficult. Operative time was defined as the time from the start of cystoscopy until the placement of a double J stent or ureteric catheter. Loin pain was assessed on postoperative day one in all patients and scored using the standard 10-point VAS, where 1 was the lowest score. 30-day postoperative complications were graded according to the Clavien-Dindo classification. All patients had a preoperative and a postoperative (24 h later) non-contrast low-dose CT scan (NCCT) using the bone window to assess stone parameters and residual fragments (RF) as well as to document any PCS injury or abnormal findings. On preoperative NCCT scan, the volume of the largest stone was calculated from the CT scan using the bone window and by measuring the stone diameter along three axes and applying the ellipsoid formula (length × width × depth × π × 0.167).
Stone-free status was classified as:
Grade A: 100% stone-free, indicating zero RF.
Grade B: Single RF not more than 2 mm in maximum diameter.
Grade C: Single RF 2.1–4 mm in maximum diameter.
Grade D: Single or multiple RFs > 4 mm in maximum diameter.
Only patients with Grades C and D that would possibly need surgical re-intervention had a 30-day NCCT scan to document RF status and plans for an ancillary procedure.
Statistical analysis
Continuous data are reported as median and (interquartile range). Categorical data are presented as absolute numbers and percentages. Statistical tests were conducted using the SPSS software package version 25.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 29 patients were included (Table 1). There were 9 (31.1%) females. Median age was 54.0 (20) years. A total of 17 (58.6%) patients were first-time stone formers. The main presenting symptom was pain (62.1%). Multiple stones were present in 12 (41.8%) patients. The most common stone location was the renal pelvis (58.7% of cases). The median volume of the largest stone was 2932 (2628) mm3. Eleven (37.9%) patients were pre-stented. Antibiotic prophylaxis was given in all patients as a single shot on the table in 41.3% of cases, while the remaining ones had extended prophylaxis up to 3 days. Table 2 shows intraoperative outcomes. 9.5/11.5 Fr size UAS (41.4%) was the most used. Calyceal inspection and stone localization were easy in all cases. Regarding the GLITZ device use, it was easily mounted and the trigger response for suction worked well in 27 cases (93.1%). There was a need to replace the trigger in one case (3.44%). Device dislodgement during use occurred in 7 (24.1%) cases. As per the Likert scale, surgeons’ objective evaluation of DISS demonstrated that it was very good in most cases (75.8%). Manipulation of DISS and laser together intraoperatively scored good and very good in 65.5% of cases. The contribution of DISS in dust aspiration was excellent in 27.6% of cases, while very good and good in 71.4% of cases. This helped in minimizing the snow globe effect. Median total surgical time was 40 (21) min. The most common dusting setting was 0.2 J/200 Hz for TFL and 0.3 J/50 Hz for Holmium laser. Contact bleeding encountered due to DISS usage was seen in 58.6% of cases. Bleeding requiring stopping surgery occurred in two (6.9%) cases. The use of an additional basket to remove fragments in the lower pole was necessary in two (6.9%) cases. Insertion of a double J stent at the end of the procedure was performed in 26 (89.7%) cases, while the remaining ones had an overnight ureteric catheter. On the table, Grade A stone-free status was 31.0% but dust remained in 65.5% of patients. Table 3 shows postoperative complications and stone-free rate (SFR). A total of 24-h CT scans showed no postoperative extravasation in all cases and Grade A SFR was 20.6% while Grade D was noted in 51.6% of cases. The most common complication was fever requiring antibiotics (Clavien grade 2; 10.3%). The sepsis rate was zero. Postoperative VAS score for loin pain was zero in 8 (27.9%) cases and graded 1–2 in 45.0% of cases. No patients had a VAS score more than 4 points. The median postoperative stay was 2 (1) days and no patient required readmission for any reason. Thirty-day CT scan was performed on 18 patients (Table 3). Overall, zero RF was seen in 75.86% 30 days after surgery and overall SFR was 96.5% with only two patients with RF on observation. No patient underwent ancillary procedures for RF.
Patient baseline characteristics.

Intraoperative outcomes.

More than one possible.
DISS, direct-in-scope suction; Fr, French; PCS, pelvis caliceal system; UAS, ureteral access sheath.
Postoperative outcomes.

CT, computed tomography; ICU, intensive care unit; SFR, stone-free rate.
Discussion
From a practical perspective, the GLITZ system is designed as an easy-to-use device, which needs a few seconds to integrate/mount the lightweight and has an ergonomic design factor of the trigger onto any scope, making this very practical and useful. This system shows much promise. It has irrigation tubing and tubes come in short and long lengths allowing the tabletop suction irrigation device to be placed ergonomically anywhere in the operating room, thus allowing for flexibility in maximizing space without interfering with other connections. It also obviates the need for additional suction and irrigation machines.
This system is the first in its class device objectively made to facilitate DISS that works effectively as an environmentally friendly, reusable (suction irrigation pump), and disposable (trigger and tubing) device system. This indeed benefits cost-conscious health systems without compromising on stability, sterility, and functionality. This is the main philosophy behind reusing disposable equipment.
In our study, we see that in 93.1% of cases the device was easily mounted, the trigger was responsive and suction worked well as this was always a new piece. In one case, a new trigger was used to complete the procedure and in the other case, this happened at the end of the procedure. Therefore, no additional strategy was deployed. We note that more improvement in its design function can prevent it from getting dismounted albeit occasionally. Yet, surgeons did not report any difficulty in ease of use or manipulation of laser with this system. In fact, the DISS procedure was successfully carried out in all patients with no need to abandon the same.
In the study by Nedbal et al., the quality parameters of the scope reached a mean Likert score of 4.5 for the DISS technique 2 and in our study as well the contribution of DISS in dust aspiration was excellent in 27.6% of cases, while very good and good in 71.4% cases. This efficiency helped in minimizing the snow globe effect given by dust and debris. The latter is one of the main reasons for poor vision during LL particularly with pulse-modulated lasers. This does affect SFR 9 and is also a reason for RFs post-conventional RIRS as was noted in the FLEXOR study. 10 We found that even though the snow globe effect is significantly mitigated, dust remained in some cases and PCS collapsed easily as irrigation was cut off. This will need to be carefully assessed in future studies to ascertain how to regulate and balance the correct irrigation inflow and aspiration to ensure all dust is removed without collapsing the PCS. In fact, the collapse of the PCS may inadvertently make the procedure slow due to the repeated need for refilling of PCS with irrigating fluid. Indeed, the use of suction as a potentially transformative tool in F-URS is now well established by numerous studies.1,11–13 In our study too, with a very short median total surgical time, 20.6% of patients had a zero RF just 24 h after surgery, and after a 30-day follow-up, the overall SFR was 96.5% with no reintervention.
The 24-h SFR using DISS is the first time being reported but is now being described in many suction-based studies for F-URS using FANS and suction access sheaths.11,14 Perhaps, it is an indicator of the elevated confidence level of surgeons being able to aspirate dust and fragments. While we performed the same only to have objective imaging to assess the true performance of the device, we think that a 30-day NCCT scan is probably adequate for assessment of RF and to objectively avoid unnecessary early re-intervention which is often reported. 15
It was observed that dust, currently defined as particles smaller than 250 µm, 16 was effectively aspirated by DISS using this device from all calyces on visual inspection in 62.06% of cases. The lower pole was indeed a challenge to aspirate dust in 10.3% of the cases. Often the dust would flush back into PCS. Even though irrigation and suction tubing to the trigger are different, the working channel is the same. Until we can create dust <250 µm, it is also possible that the particles will not be aspirated and hence for DISS using any technology this can be a potential limitation as was shown by Madden et al. 3 Moreover, there is a hypothesis that large particles can inadvertently block the working channel. 3 Yet, because our device has an automatic sensor to stop irrigation if such an occurrence happened, we did not encounter any events. The device safety mechanism ensures that any system malfunction does not affect the RIRS procedure or scope damage. Surgeons may continue to perform the procedure by simply detaching the device if they were to face any issues, making it versatile. Yet, DISS with GLITZ device mitigated infectious complications, and no sepsis was reported by absolving pyelovenous and pyelolymphatic backflow well recorded as an advantage of using suction.11–14
No additional device-related morbidity was seen apart from contact bleeding that occurred in more than half of the patients. This was multifactorial and related to the sudden collapse of the collecting system during aspiration, scope tip rubbing against the mucosa while aspirating the dust, or even due to scope manipulation in all parts of the collecting system with aspiration as irrigation gets cut off during surgery. Hence, surgeons must be aware that DISS, whilst feasible and safe, can also have operative problems of contact bleeding while performing suction and aspiration. This may not be a direct consequence of the device used but indeed much more information is needed on how to regulate the suction and irrigation parameters to avoid this phenomenon, especially as surgeons need to dust proactively with lasers and then aspirate the dust carefully during which irrigation gets cut off.
Our study aims were completed with no adverse events that compromised patient safety. No serious device malfunctions were reported, which is proof that this design concept of GLITZ delivers on its intended goals as a DISS-capable device. However, the GLTZ device has some limitations. First of all, ours is the first-ever clinical audit study for this new device and is thus used in conjunction with a UAS to ensure that patient safety is not compromised during the procedure. Second, its true suction-aspiration capabilities should be better ascertained when RIRS is performed without using a UAS. Third, we acknowledge that like any device there is always a training and learning curve involved and a phase II study comparing DISS using GLITZ vis a vis other suction aspiration techniques/devices is the best way to discern its utility in RIRS with suction. Notably, the 30-day SFR was very high which indicates that by using the device laser efficacy was not compromised. Perhaps aided by on-table aspiration, patients in all probability were eventually able to pass dust/debris and tiny fragments that could not be or were missed intraoperatively. Therefore, its true merit will be in using the device ad hoc without a UAS. Yet, until a safe way to monitor intrarenal pressure with DISS is established, it cannot be advocated. Finally, we acknowledge that the limitations of this study are its small sample size, the lack of a comparison group, no sample size calculation, the use of different laser techniques, different settings, different UAS sizes, the inclusion of some pre-stented patients, and that two experienced surgeons performed all procedures. Yet, this was the first proof of concept prospective audit for the design and functionality of the device, and we are honestly able to assess and disclose the merits and challenges needed to overcome. The GITZ device will need to be tested for its efficacy when used with other flexible ureteroscope handles for it to have a universal appeal.
Conclusion
DISS using the GLITZ system is easy and safe to perform with surgeons reporting good to very good scores for functionality. The single intervention 30-day grade A and B SFR was 96.6% including a zero RF status in 75.86% of patients with no patient needing repeat surgical intervention. These results indicate that DISS with this device is effective. Notably from our small sample study, the absence of sepsis and good peri and postoperative outcomes reiterates that DISS modality shows much promise if validated in larger studies. Indeed, the system may need improvements to overcome operator handling issues and dedicated studies to determine optimal irrigation flow rates when using this apparatus. As this study was done by experienced urologists and the number of patients is limited, it remains to be seen how the device performs in real-world practice. As this is a single-arm study only, future comparative studies preferably randomized can assess the performance of this device against other DISS techniques.
Supplemental Material
sj-docx-1-tau-10.1177_17562872251320807 – Supplemental material for Introducing a new device for direct in-scope suction technique during flexible ureteroscopy for kidney stone disease: an EAU Section of Endourology prospective multicenter audit using the GLITZ system
Supplemental material, sj-docx-1-tau-10.1177_17562872251320807 for Introducing a new device for direct in-scope suction technique during flexible ureteroscopy for kidney stone disease: an EAU Section of Endourology prospective multicenter audit using the GLITZ system by Vineet Gauhar, Olivier Traxer, Nanjappa Madappa Kandarthanda, Bhaskar K. Somani, Daniele Castellani, Ravindra B Sabnis and Deepak Ragoori in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.