
Abstract
Background:
Pelvic lipomatosis (PL) is a rare condition that is characterized by excessive growth of fat in the pelvic cavity. Studies have yet to systematically review surgical treatments for PL.
Objectives:
To provide a reference for selecting reasonable surgical treatments for PL patients according to previous literature on the surgical treatment of PL.
Design and methods:
We conducted this systematic review in accordance with the Preferred Reporting Items for a Systematic Review and Meta-Analysis (PRISMA) of Individual Participant Data guidelines. Literature on PL published from 1968 to 2022 was retrieved from the PubMed and EMBASE databases. Data were collected and analyzed independently by two independent investigators.
Results:
A total of 42 studies, involving 231 patients with PL, were included in the analysis. The surgical treatments included transurethral resection (TUR) (48.5%), ureteral stent placement (11.7%), percutaneous nephrostomy (1.3%), ureterocutaneostomy (1.3%), ureteral reimplantation (10.4%), ileal conduit (13%), and allograft kidney transplantation (0.4%). After excluding patients with unclear prognoses, 42.9% of patients showed improvement in lower urinary tract symptoms (LUTS) after TUR. Ureteral stent placement provided relief of hydronephrosis in 62.5% of PL patients. Percutaneous nephrostomy resulted in stable renal function in 33.3% of PL patients, while ureterocutaneostomy led to remission of postoperative hydronephrosis in 33.3% of PL patients. After ureteral reimplantation, 70.8% of patients experienced relief of hydronephrosis or had stable renal function. Ileal conduit led to remission of hydronephrosis, alleviation of symptoms, or maintenance of stable renal function in 83.3% of PL patients. One patient with PL had stable renal function after allograft renal transplantation.
Conclusion:
The surgical treatments for PL include TUR, ureteral stent placement, urinary diversion, and allograft renal transplantation. However, the choice of surgical method should be determined after comprehensive consideration of the patient’s condition.
Plain language summary
Pelvic lipomatosis (PL) is a rare condition that is characterized by excessive growth of fat in the pelvic cavity. Studies have yet to systematically review surgical treatments for PL. To provide a reference for selecting reasonable surgical treatments for PL patients according to previous literature on the surgical treatment of PL, we conducted this systematic review in accordance with the Preferred Reporting Items for a Systematic Review and Meta-Analysis of Individual Participant Data (PRISMA) guidelines. A total of 42 studies, involving 231 patients with PL, were included in the final analysis. Among 231 patients with PL, the surgical treatments included transurethral resection (TUR) (48.5%), ureteral stent placement (11.7%), percutaneous nephrostomy (1.3%), ureterocutaneostomy (1.3%), ureteral reimplantation (10.4%), ileal conduit (13%), and allograft kidney transplantation (0.4%). After excluding patients with unclear prognoses, 42.9% of patients showed improvement in lower urinary tract symptoms (LUTS) after TUR. Ureteral stent placement provided relief of hydronephrosis in 62.5% of PL patients. Percutaneous nephrostomy resulted in stable renal function in 33.3% of PL patients, while ureterocutaneostomy led to remission of postoperative hydronephrosis in 33.3% of PL patients. After ureteral reimplantation, 70.8% of patients experienced relief of hydronephrosis or had stable renal function. Ileal conduit led to remission of hydronephrosis, alleviation of symptoms, or maintenance of stable renal function in 83.3% of PL patients. One patient with PL had stable renal function after allograft renal transplantation. The surgical treatments for PL include TUR, ureteral stent placement, urinary diversion, and allograft renal transplantation. However, the choice of surgical method should be determined after comprehensive consideration of the patient’s condition.
Introduction
Pelvic lipomatosis (PL) is a rare condition that is characterized by excessive growth of fat in the pelvic cavity. This can cause compression of the bladder, ureter, rectum, and blood vessels, resulting in complications such as cystitis glandularis (CG), dysuria, hydronephrosis of the upper urinary tract, renal failure and constipation. While the incidence rate of PL is relatively low, at 0.6–1.7/100,000, 1 it is expected to increase due to advancements in medical detection technology and increasing awareness of the condition. The treatment of PL includes conservative treatment and surgical treatment. Conservative treatment mainly includes hormones, antibiotics, weight loss, and diet management, 2 but its efficacy is limited.3–5 Surgical treatments for PL include transurethral resection (TUR), ureteral stent placement, urinary diversion, and allograft kidney transplantation. To our knowledge, studies have yet to systematically review surgical treatments for PL. To better understand the surgical treatments available for PL and to assist in selecting a suitable treatment plan for PL patients, literature on the surgical treatment of PL was systematically reviewed.
Methods
This systematic review was performed according to the Preferred Reporting Items for a Systematic Review and Meta-Analysis (PRISMA) guidelines. PubMed and EMBASE databases were searched to identify eligible studies published from 1968 to 2022. The term used for the search were ‘pelvic lipomatosis’. Population, Intervention, Comparator, Outcome, and Study design criteria were applied. Studies that reported clinical data of patients of any age with a clinical diagnosis of PL (population) receiving surgical treatment (intervention) were included. Success of surgical treatment was defined as the alleviation of symptoms, remission of hydronephrosis, or maintenance of stable renal function (outcome). Observational studies written in English including case series or case-reports were eligible (study design). However, on the other hand, studies meeting the following criteria were excluded: (1) studies characterized as a review, without full text; (2) studies lacking data on surgical treatment; and (3) studies with overlapping populations. Data were extracted from the selected publications, including year of publication, source of publications, race, sex, age, body mass index (BMI), symptoms, presence of CG or hydronephrosis, type of surgical management, and outcomes. Two independent authors performed data extraction. Statistical analysis was conducted using the Statistical Package for Social Sciences, version 25.0 (SPSS, Chicago, IL, USA). Two independent investigators conducted a risk of bias assessment on studies included in the outcome analysis, utilizing the ORBIT (Outcome Reporting Bias In Trials) classification system. 6
Results
Literature search results and demographics
A total of 42 studies,1–3,7–45 including 231 patients with PL were finally included in this systemic review. The detailed literature search process is illustrated in Figure 1. The studies included in the review were published between 1968 and 2022. The majority of the studies (52.4%) were from Asia, followed by North America (33.3%), Europe (9.5%), Oceania (2.4%), and Africa (2.4%). Among the cohort of 231 PL patients, 6 (2.6%) were White, 45 (19.5%) were Black, and 170 (73.6%) were Asian. The median age of the PL patients was 43 years old [interquartile range (IQR): 37–52] and the median BMI was 25.5 (IQR: 24.5–26.1). CG was observed in 151 PL patients (65.4%), while hydronephrosis was found in 133 PL patients (57.6%). Furthermore, 31 PL patients (13.4%) experienced renal failure. The main clinical symptoms of PL were lower urinary tract symptoms (LUTS) (39.0%), hematuria (7.4%), flank pain (8.2%), and constipation (1.3%). Table 1 presents the characteristics of the patients.

PRISMA flow chart of literature screening.
Characteristics of the included literature and PL patients.

BMI, body mass index; IQR, interquartile range; LUTS, lower urinary tract symptoms; PL, Pelvic lipomatosis.
Surgical treatments
Surgical treatments for PL include TUR, ureteral stent placement, urinary diversion such as percutaneous nephrostomy, ureterocutaneostomy, ureteral reimplantation, ileal conduit, and kidney transplantation. Among the 231 patients with PL, TUR accounted for 48.5% of cases, ureteral stent placement for 11.7%, percutaneous nephrostomy for 1.3%, ureterocutaneostomy for 1.3%, ureteral reimplantation for 10.4%, ileal conduit for 13%, and allograft kidney transplantation for 0.4% (Table 2).
Surgical treatment of 231 patients with PL.
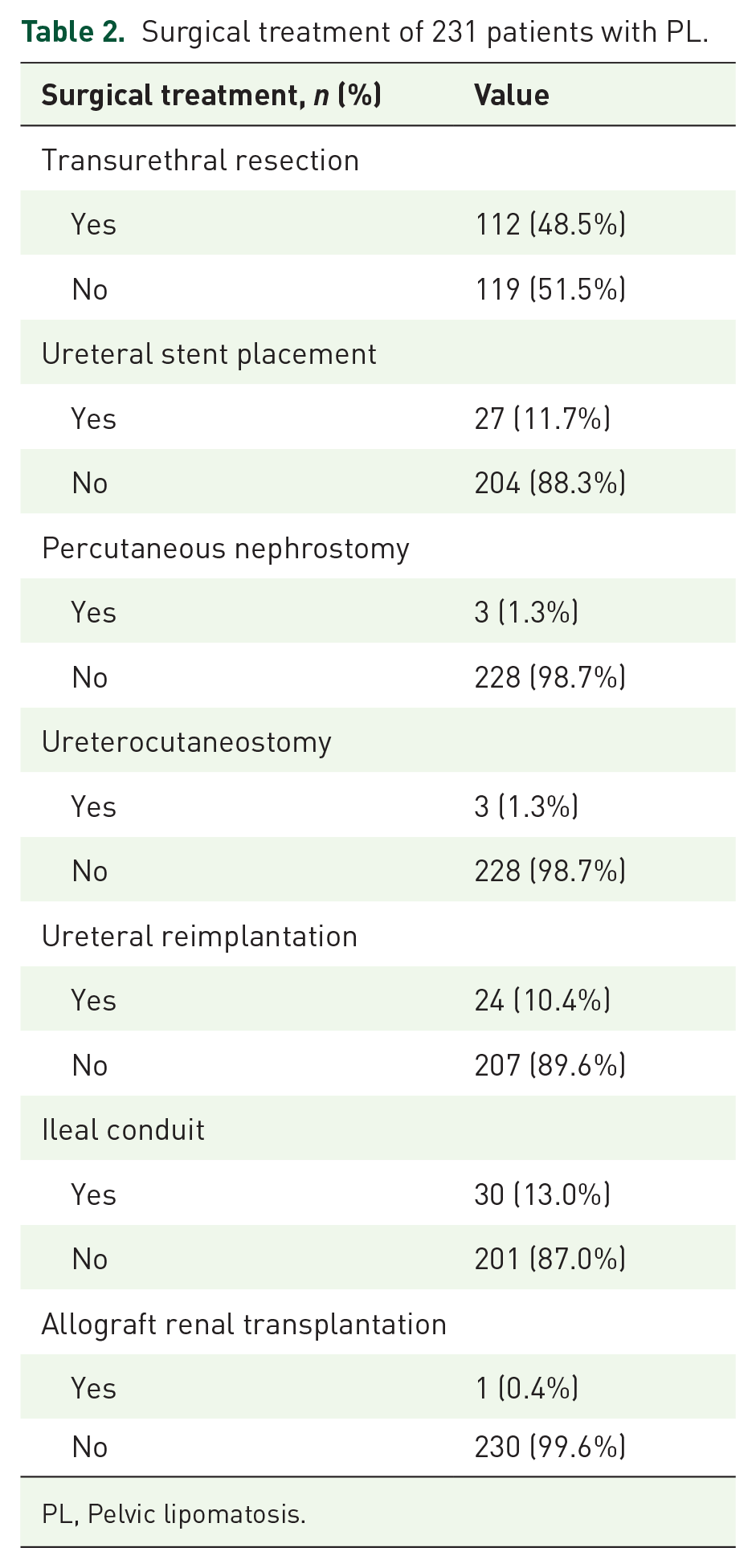
PL, Pelvic lipomatosis.
Treatment outcomes
After excluding patients without a clear prognosis, 42.9% of patients experienced improved LUTS after undergoing TUR. Ureteral stent placement provided relief of hydronephrosis in 62.5% of patients with PL. Percutaneous nephrostomy resulted in stable renal function in 33.3% of PL patients, while ureterocutaneostomy led to remission of postoperative hydronephrosis in 33.3% of PL patients. After ureteral reimplantation, 70.8% of PL patients experienced relief of hydronephrosis or maintenance of stable renal function. Ileal conduit resulted in remission of hydronephrosis, alleviation of symptoms, or maintenance of stable renal function in 83.3% of patients. One patient with PL had stable renal function after allograft renal transplantation. Supplemental Table 1 presents the results of the ORBIT classification of the studies included in the outcome analysis (Table 3).
Outcomes of different surgical treatment procedures for PL.

LUTS, lower urinary tract symptoms; PL, Pelvic lipomatosis.
Discussion
PL is a rare benign disease. At present, the surgical treatments for PL reported in the literature include TUR, ureteral stent placement, urinary diversion, and allograft kidney transplantation.
TUR is a commonly used method to treat bladder cancer and benign prostatic hyperplasia, and it can also be used for CG patients. TUR can treat CG by achieving diagnostic resection, alleviating dysuria, exposing the ureteral opening, or excising glandular hyperplasia tissue. 9 When TUR is used to treat CG in PL patients, attention should be given to avoiding excessive removal of glandular hyperplasia tissue, as excessive TUR may further exacerbate the inflammatory response of the bladder mucosa. As early as 1979, it was reported that TUR was suitable for PL patients with CG. 13 Hence, TUR is an alternative treatment option for most PL patients with CG. In our study, 42.9% of PL patients combined with CG experienced relief of LUTS after TUR. However, these patients still have the risk of CG recurrence or progression after TUR, and further research is warranted to determine which PL patients are susceptible to CG recurrence or progression, the risk factors for CG recurrence or progression, and the strategies to reduce the risk of CG recurrence or progression after TUR.
The ureteral stent can be used to treat various types of ureteral obstruction.46,47 It has the advantages of less trauma, a good drainage effect, fewer complications, and a high postoperative quality of life. 48 The ureteral stent can also be used for PL patients to alleviate hydronephrosis and protect renal function.7,9,49 As early as 1988, Demas et al. 19 reported the data of five patients with PL, and finally, two patients underwent ureteral stent placement to relieve the mechanical obstruction. For PL patients with hydronephrosis, ureteral stent placement is a feasible method.9,18 In this systematic review, ureteral stents alleviated hydronephrosis in 62.5% of PL patients, and 37.5% of PL patients did not show clear relief of hydronephrosis, which may be related to the obstruction of ureteral stents or the severe increase in bladder pressure resulting from the compression of the bladder by excess fat.
PL patients who experience persistent hydronephrosis after ureteral stent placement, severe changes in bladder morphology, severe damage to lower urinary tract function, or unsuccessful ureteral stent placement need to undergo urinary diversion. The urinary diversion methods include percutaneous nephrostomy, ureterocutaneostomy, ureteral reimplantation, and ileal conduit. Different operation methods have their advantages and disadvantages, which should be selected according to the specific conditions of the patients.
Ureterocutaneostomy and percutaneous nephrostomy can also be used for PL patients when they need urinary diversion. As early as 1976, Radinsky et al. 24 performed bilateral ureterocutaneostomy on a PL patient with severe hydronephrosis and serious changes in bladder morphology. In 1987, Allen and De Kock 22 reported on a case of PL with ureteral obstruction and vesicoureteral reflux, and these complications were finally relieved by percutaneous nephrostomy. Similar to ureteral stent placement, percutaneous nephrostomy is often used to temporarily alleviate the obstruction. Improper operation or ineffective nursing care may lead to risks such as bleeding, fistula prolapse, stones, urinary exosmosis, and urinary fistula. 50 In our study, 33.3% of PL patients had stable renal function or relieved hydronephrosis after percutaneous nephrostomy or ureterocutaneostomy. Due to the limited sample size and the lack of standardized reporting in the included case reports, it is possible that there may be variation between this finding and the actual value. In the realm of clinical practice, we believe that percutaneous nephrostomy and ureterocutaneostomy hold a greater likelihood of preserving stable renal function or alleviating hydronephrosis in PL patients. Additionally, opting for a renal fistula tube with a larger diameter will enhance the safeguarding of renal function.
Ureteral reimplantation can be used for various ureteral terminal obstruction and reflux diseases.51,52 In PL patients who need urinary diversion, ureteral reimplantation is often combined with fat removal.1,2 As early as 1977, Gerson et al. 30 reported for the first time the case of a PL patient undergoing ureteral reimplantation. Ureteral reimplantation is an effective treatment for PL patients. In our systematic review, 70.8% of patients experienced relief of hydronephrosis or stable renal function after ureteral reimplantation. However, PL patients still face the problem of recurrent ureteral stricture caused by continued growth of pelvic fat after ureteral reimplantation.2,19,29 On the one hand, the growing pelvic fat may compress the replanted ureter again, resulting in recurrent ureteral stricture. On the other hand, the growing pelvic fat may further increase the pressure in the bladder after pressing the bladder, resulting in poor urine drainage. At present, the limitations of relevant research on ureteral reimplantation for PL lie in the small sample size and short follow-up time, and studies with larger sample sizes and longer follow-up times are still needed to further verify the long-term effectiveness and safety of ureteral reimplantation for PL patients. Hence, ureteral reimplantation in the treatment of PL is still controversial. Although many studies have reported the application of ureteral reimplantation in PL patients, we believe that it is not suitable to protect the upper urinary tract and relieve hydronephrosis in PL patients. First, since the pelvic fat of PL patients is hard and tightly adhered to the ureter, it is difficult to separate the ureter and adipose tissue during the operation, which is a great risk. In addition, after ureteral reimplantation, fat that continues to grow may continue to compress the ureter-bladder anastomosis, thus causing recurrent ureteral stricture. Therefore, we do not recommend ureteral reimplantation for PL patients.
The ileal conduit is suitable for PL patients with persistent hydronephrosis after ureteral stent placement, severe changes in bladder morphology, severe damage to lower urinary tract function, or unsuccessful ureteral stent placement. PL patients with failure of ureteral reimplantation can also receive ileal conduits2,19,29 to protect the upper urinary tract and relieve hydronephrosis. As early as 1968, it was reported that ileal conduits were used to treat PL. 38 The risk of complications still exists after ileal conduit, including early complications such as urine leakage, intestinal obstruction, intestinal fistula, and urinary tract infection, and late complications such as skin fistula retraction and stenosis, ureteral anastomotic stenosis, and nephroureteral calculi.53–55 Yang et al. 56 reported the case of a PL patient with recurrent ureteral stricture after ileal conduit. Thus, traditional ileal conduit surgery is still associated with a risk of recurrent ureteral stricture due to the continued pressure of growing fat on the ureteral-ileal anastomosis site, as the ureteral-ileal anastomosis site is close to the pelvic cavity. Modified ileal conduit surgery with ureteral-ileal anastomosis at the lower pole level of both kidneys may be a new trend for urinary diversion in PL treatment in the future. Ileal conduit surgery is a major urologic operation that requires a high level of physical and mental cooperation from patients. In addition, it has a great impact on patients’ physiology and daily life. Hence, in the selection of this surgery, the patients’ conditions need to be comprehensively considered. In our systematic review, 83.3% of PL patients experienced remission of hydronephrosis, alleviation of symptoms, or maintained stable renal function after ileal conduit.
Allograft renal transplantation is one of the most effective methods used to treat end-stage renal disease.57,58 Due to the extrusion of hyperplastic fat, PL patients may gradually develop obstructive urinary tract diseases, and the conditions of 40% of them will deteriorate into renal failure after an average of 5 years.27,36,59 When PL patients suffer end-stage renal disease, allograft renal transplantation can be selected to improve their renal function. 21 Therefore, when allograft renal transplantation is performed in PL patients, attention should be given to the selection of appropriate sites of renal transplantation and methods of urinary diversion.
To our knowledge, this study provides a systematic review of surgical treatment for PL for the first time. This study has limitations. Due to the rarity of PL, the majority of the literature included in this study consists of a small number of cases, and these reports lack standardized formatting, which can make it necessary to interpret the conclusions drawn from our study with caution. It is crucial to consider the context of clinical practice when evaluating these findings. In addition, some clinical features or data may be omitted from previous literature, which can lead to some potential biases. However, these biases will not prevent us from further understanding this disease. In our clinical practice, we will comprehensively consider previous literature and specific clinical practice to choose the most suitable treatment plan for PL patients.
Surgical treatments for PL include TUR, ureteral stent placement, urinary diversion, and allograft renal transplantation. It is necessary to comprehensively consider the patients’ conditions to determine the most appropriate surgical treatment method. The published studies related to PL have limitations such as a small sample size, lack of standardization, short follow-up time, or even no follow-up. In the future, studies with larger samples, higher evidence levels, and longer-term follow-up are needed to further confirm the effectiveness and safety of these surgical treatment methods for PL.
Supplemental Material
sj-xlsx-1-tau-10.1177_17562872231217842 – Supplemental material for Surgical treatment of pelvic lipomatosis: a systematic review of 231 cases
Supplemental material, sj-xlsx-1-tau-10.1177_17562872231217842 for Surgical treatment of pelvic lipomatosis: a systematic review of 231 cases by Mancheng Xia, Shengwei Xiong, Zhihua Li, Shubo Fan, Yuke Chen, Liqun Zhou, Kai Zhang and Xuesong Li in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.