
Abstract
Introduction:
Transperineal laser ablation (TPLA) of the prostate is a new, minimally invasive technique for benign prostatic hyperplasia (BPH) with promising effectiveness and safety outcomes. This systematic review aims to provide an update of existing literature.
Methods:
A literature review was performed in Pubmed/MEDLINE, Embase, Cochrane Library, and clinicaltrials.gov from January 2000 up to April 2023. Data extraction and risk of bias were performed independently by three authors.
Results:
A total of 11 studies were included, among which 9 were observational, 1 randomized controlled trial, 1 animal study, while 2 of them were comparative (1 with prostatic artery embolization and 1 with transurethral resection of the prostate). Functional outcomes were improved in the majority of studies both for objective (maximum flow rate and post-void residual) and subjective outcomes (improvement of International Prostate Symptom Score and quality of life). Complication rates ranged between 1.9% and 2.3% for hematuria, 3.7% and 36.3% for dysuria, 1.9% and 19% for acute urinary retention, 0.6% and 9.1% for orchitis/urinary tract infections, and 0.6% and 4.8% for prostatic abscess formation. Regarding sexual function, >95% of patients retained their ejaculation while erectile function was maintained or improved.
Conclusion:
TPLA of the prostate is an innovative, minimally invasive technique for managing patients with BPH. Existing studies indicate an effective technique in reducing International Prostate Symptom Score and quality of life scores, post-void residual reduction, and increase in Qmax, albeit the measured improvements in terms of Qmax are not equal to transurethral resection of the prostate. Although sexual function is maintained, the mean catheterization time is 7 days, and no long-term data are available for most patients.
Introduction
Benign prostatic hyperplasia (BPH) is a very common clinical condition with a progressive natural history in men aged over 45–50 years. The reported prevalence among men aged over 60 years is up to 40%. 1 Lower urinary tract symptoms (LUTS) and coexisting erectile dysfunction in up to 50–60% are the main symptoms while patients may also encounter serious complications such as recurrent infections, bleeding, or renal failure.1,2 Treatment algorithm entails a stepwise approach with conservative management for mild symptoms, monotherapy, or combined pharmacotherapy for moderate symptoms (α-blockers, 5-α-reductase inhibitors, β3-adrenergic agonists, anticholinergics, Phosphodiesterase-5 (PDE5)-inhibitors) and surgical management for severe symptoms, recurrent disease, or in case of complications. 1
Transurethral resection of the prostate (TURP) has been the gold-standard treatment for many and has withstood the test of time, but nowadays enucleation techniques using several energy types (holmium: YAG-HoLEP, thulium laser – ThuLEP, bipolar energy – bipoLEP) are proved to be at least as effective as resection, while a recent network meta-analysis indicates that they may be even superior to TURP.3,4 TURP is a technique indicated for prostates sized up to 80–100 ml, is accompanied by excellent functional outcomes, but is also associated with side effects such as bleeding, urethral strictures, infections, bladder neck contracture and, importantly, permanent sexual dysfunction, mainly in the form of retrograde ejaculation in more than 60% of the patients. 5 Since quality of life (QoL) is greatly affected by sexual function, especially in younger men, TURP sustainable effectiveness is often hindered by these side effects. Enucleation techniques with laser/bipolar energy are also commonly accompanied by sexual dysfunction. 1
In the last 10 years, a number of minimally invasive surgical therapies (MIST) for BPH have emerged: Aquablation therapy, convective water vapor therapy (Rezum), temporary implantable nitinol device (iTIND), Urolift, and prostatic artery embolization (PAE). 1 Although these techniques offer inferior clinical outcomes compared to TURP and enucleation techniques, it is the preservation of sexual function and ability to perform them in an outpatient setting, which have rendered them a quite popular option among the male population. One of the newest MIST is transperineal laser ablation (TPLA) of the prostate, which is still not incorporated in the European Association of Urology Guidelines, but accumulating evidence indicate that it is an effective and safe method. In this systematic review of the literature, we aim to provide an updated summary of the existing evidence on TPLA.
Methods
Search strategy
This systematic review was conducted according to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement. 6 A literature search was performed using Pubmed/MEDLINE, Embase, Cochrane Library for Clinical Trials, and clinicaltrails.gov for studies focusing on TPLA and published in the English language between January 2000 and April 2023. Reference lists of all included studies were screened as well. The following key terms were used in combination: benign prostatic enlargement, BPH, bladder outlet obstruction, BPE, BPH, BOO, LUTS, and TPLA. Duplicates were removed using a citation manager tool (Clarivate Analytics, version 20).
Selection of studies, assessment of risk of bias, and data extraction
Two authors (LT and SN) performed an independent screen of the literature by title and abstract, to identify eligible studies. After initial screening, a full-text evaluation followed to decide the studies to be included. All disagreements were dissolved upon consensus with a third author (AP). Eligible studies were observational, either prospective or retrospective, single arm or comparative, and randomized controlled trials (RCTs). Animal studies, case reports, conference abstracts, trial protocols with no reported outcomes, editorial comments, non-English studies, and those with a sample size less than 10 patients were excluded.
Data extraction was performed independently by three authors (LT, SN, and AP) using a predefined Excel spreadsheet, which included baseline study characteristics (author name, year of publication, country, study design, inclusion and exclusion criteria, description of technique, sample size, and follow-up) and patient characteristics [age, prostate volume (PV), International Prostate Symptom Score (IPSS) at baseline and postoperatively, post-void residual (PVR) at baseline and postoperatively, maximum flow rate (Qmax) at baseline and postoperatively, questionnaire responses and scores, complication rates, length of catheterization, and hospital stay]. Any disagreements were resolved upon consensus among the three authors after carefully revising the eligible studies.
Risk of bias (RoB) was assessed independently by three authors (LT, SN, and AP) using the Cochrane tools for non-randomized studies (Risk Of Bias in Non-randomised Studies of Interventions - I (ROBINS)). 7 For RCTs, the updated version of the Cochrane risk-of-bias tool for randomized trials (RoB 2) was used. 8 The quality of this systematic review has been evaluated using the updated AMSTAR 2. 9
Results
Study selection
The literature search revealed a total of 102 studies among the four databases. After the removal of 3 duplicates, 99 records were screened by title and abstract. After excluding 74 records (65 due to irrelevant subjects, 3 conference abstracts, and 6 protocols with no published outcomes), 25 full texts were screened for eligibility. Finally, after excluding 3 reviews and 11 studies not on BPH or transperineal route of therapy, 11 studies were deemed eligible for inclusion: 1 RCT, 10 1 animal study, 11 and 9 observational studies,12–20 from which one was comparative. 12 Since only two comparative studies were found, one of which was an RCT and they compared TPLA with either PAE or TURP, no meta-analysis was performed. PRISMA flow diagram is shown in Figure 1. Baseline study characteristics are depicted in Table 1. RoB for selected studies is shown in Supplemental Tables 1–3. A MeaSurement Tool to Assess systematic Reviews 2 scale is shown in Supplemental Files.

Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flowchart of the included studies.
Baseline study characteristics.

BPH, benign prostatic hyperplasia; IPSS, International Prostate Symptom Score; LUTS, lower urinary tract symptoms; PSA, Prostate Specific Antigen; PV, prostate volume; PVR, post-void residual; Qmax, maximum urinary flow rate; RCT, randomized controlled trial; TPLA, Transperineal Laser Ablation; TRUS, transrectal ultrasound; TURP, transurethral resection of the prostate; US, ultrasound.
Technical aspects
The available studies demonstrated heterogeneity in the type of equipment that was used. While differences existed among the applied techniques. The main principles were similar and are summarized below.
Position and preparation: The procedure was performed in a lithotomy position with the testes and penis lifted and fixed to expose the perineum. An 18Fr three-way catheter was placed, while continuous normal saline irrigation for urethral cooling to prevent urethral wall injury was applied.13,16 The procedure was performed under transrectal ultrasound (TRUS) guidance with a biplanar 4–13 Hz probe. 13 Furthermore, the use of a multi-channel needle applicator with a dedicated software display grid overlapping the ultrasound images could also aid the procedure. 16
Anesthesia: The perineum was disinfected with wipes and the procedure was performed under local anesthesia only,13,17 or conscious sedation and local anesthesia.15,16,18,19 Lidocaine 2% was administered to the perineum and the periprostatic region for local anesthesia.13,15
Equipment and settings: The SoracteLite EchoLaser, Elesta laser ablation system was used. A dedicated planning tool (Echolaser Smart Interface, Elesta S.p.A, Calenzano, Italy) with simulation software allowed the user to plan the treatment and to place applicators in the prostate in a safe manner.13,15–18 A 21G trocar needle was used to accommodate the 300-μm flat-tip optical fiber and a continuous mode with a wavelength of 1064 nm was employed. At this wavelength, the penetration of light in the infrared spectrum was optimal. 13 The energy setting was 1800 J per fiber and illumination at a fixed power of 3 W,13,15,18,19 or 4.5–5 W reduced to 3–3.5 W after 1–2 min.16,17,20
Details of the procedure: The initial planning is conducted on the biplanar TRUS, to ensure adequate margins of safety. The ellipsoid area of coagulative necrosis extends to 22.5 mm longitudinally (of which two-thirds are localized beyond the tip of the fiber and one-third behind the tip) and 16 mm transversely. 16 Hence, the needle tip must be at least 15 mm from the base of the bladder and 8–10 mm from the urethra and prostate capsule to ensure a safe procedure. A 21G Chiba needle was inserted percutaneously in the perineum, under ultrasound guidance, and the energy delivered through the laser fiber was transferred through the needle. The needle was inserted as parallel to the longitudinal axis of the prostate as possible. The laser fiber protrudes 5–10 mm outside of the tip of the needle.13,14,16 Additional fibers may be used, depending on the size of the prostate. Generally, one fiber was needed for each lobe of the prostate. However, for gland sizes more than 45–60 ml,15,17 additional fibers may be required. Also, additional fibers are needed in case a median lobe exists. Whenever additional fibers are used, the distance between them must be 10–15 mm to comply with the created ellipsoid area of coagulative necrosis, as discussed above. Also, if the prostate gland has an increased volume profile longitudinally, a ‘pull-back’ maneuver to ensure adequate ablation may be used. 16 The treatment ablation lasted between 400 and 600 s 17 or was concluded when the maximum energy of 1800 J per fiber was reached.15,18,19 The ablation range evaluation was performed by contrast-enhanced ultrasound in three studies,13,18,19 and MRI in one study. 17
A graphical illustration of the technique is shown in Figure 2, while Figures 3 and 4 show the intraoperative setting and use of the equipment.

Graphical illustration of TPLA.

(a) Intraoperative setting, (b) laser setting screen, (c) transrectal application of ultrasound transducer, and (d) appearance of the prostate using the transrectal ultrasound probe.
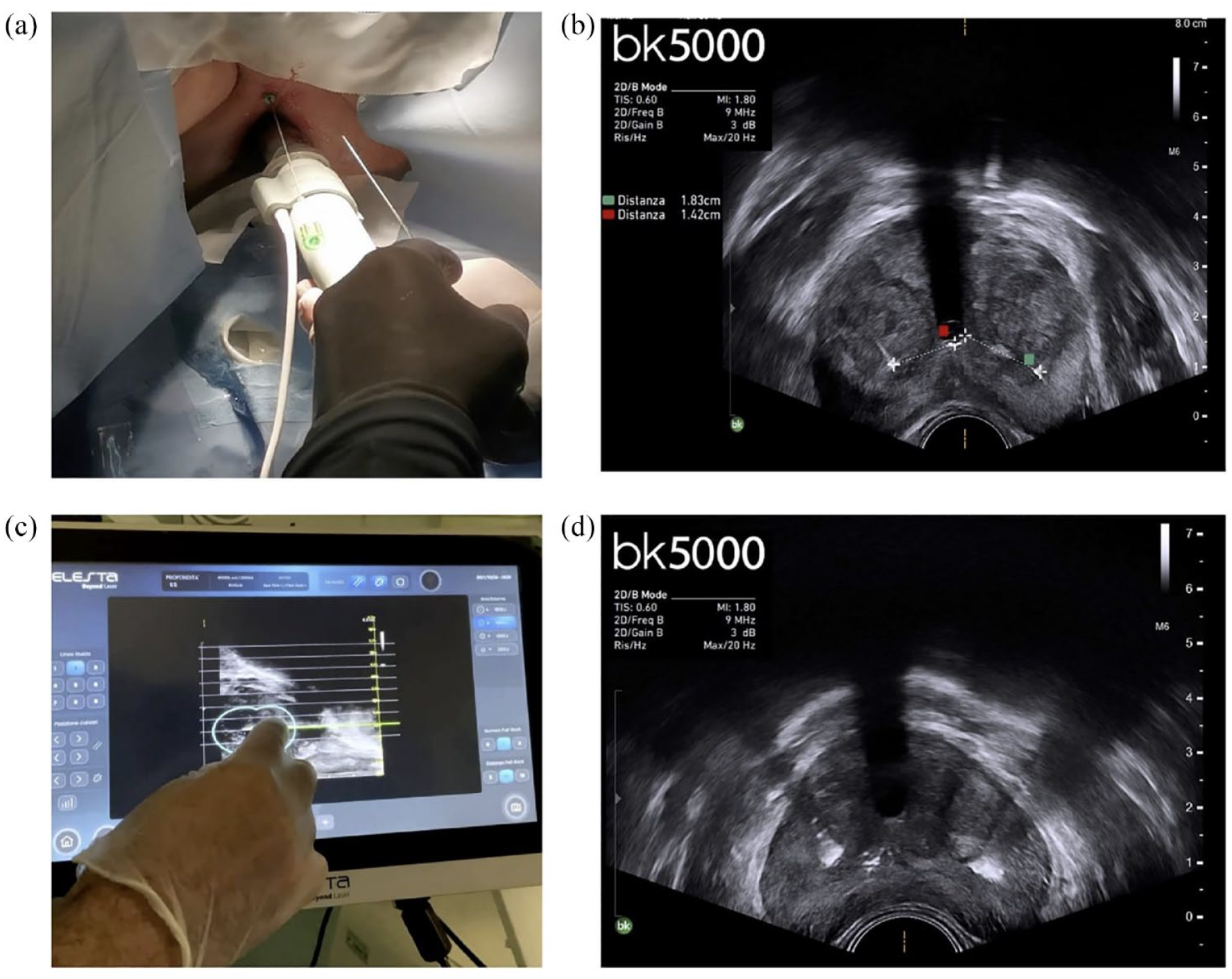
(a) Insertion of needles using the transrectal probe, (b) measurement of distance between needles and urethra, (c) selection of needle, and (d) application of energy.
Inclusion and exclusion criteria for the technique
Among the inclusion criteria of the eligible studies, patients over 18 years old and PV between 30 and 100 ml, based on TRUS or MRI measurements, were eligible for TPLA treatment. In addition to this, LUTS with IPSS ⩾ 12, Qmax ⩽15 ml/s, or PVR 50–400 ml were common inclusion criteria. Prior urethral procedures, PSA >4 ng/ml or suspected prostate cancer, urethral stricture history, neurological disease (spinal cord surgery, Parkinson’s disease, multiple sclerosis), allergy to ultrasound contrast, underactive detrusor, bladder cancer, prior prostatic abscess, acute or chronic prostatitis, active urinary tract infection, gland volume over 100 ml, bladder stones, and active hematuria were common exclusion criteria. A detailed list of them is found in Table 2.
General inclusion and exclusion criteria.

IPSS, International Prostate Symptom Score; PVR, post-void residual; Qmax, maximum urinary flow; TRUS, transrectal ultrasound.
Operative and perioperative data
Procedural time ranged between 28 and 61 min, with the actual ablation time being between 13 and 42.6 min. In most studies, a short hospitalization time was required (1–2), while Sessa et al., 20 who performed the procedure in an outpatient setting, reported a median monitoring of 6.4 h and only one patient required re-hospitalization for pelvic discomfort. Catheterization time ranged between 4 and 17.3 days, with the majority of patients requiring a catheter for 7–8 days. The measured total energy deployed was 6616.2–10,522 J, while two studies reported the coagulation zone, which was 10.3–11.7 ml.12,19 Operative and perioperative data are summarized in Table 3.
Operative and perioperative data.

IQR, interquartile range; TPLA, transperineal laser ablation; TRUS, transrectal ultrasound.
Functional outcomes
The age of patients in the included studies ranged between 61.9 and 73.9 years old, while PV at baseline was measured between 40 and 102 ml, although in the majority of studies except one, 17 median PV before ablation was <100 ml. IPSS at baseline indicated severe disease with a median of 18.3–22.7 among studies and PVR ranged between 60 and 199.9 ml. Qmax at baseline was also low, with a median of 7.6–9.2 ml/s. QoL was severely affected in all studies, with a median score ranging between 5 and 5.8, based on the IPSS QoL-related question. In all studies, IPSS was reduced during follow-up, with median values ranging between 8–13.1 at 3 months and 5–7 at 6–12 months, indicating a moderate-term effectiveness for symptom relief. Similarly, the QoL component of IPSS was also improved, with a reported median of 1–2.1 at 3 months and 1–2.3 at 6–12 months. Qmax improved compared to baseline and ranged between 11–13.3 ml/s at 3 months and 11.5–20.5 ml/s at 6–12 months follow-up. PVR postoperatively ranged between 45.6–54.8 ml at 3 months and 41.5–60.3 ml at 6–12 months of follow-up. All functional outcomes are shown in Tables 4 and 5.
Patient characteristics and outcomes.

PAE, prostatic artery embolization, BPH, benign prostatic hyperplasia; f/u, follow-up; IIES, International Index for Erectile Function; IPSS, International Prostate Symptom Score; IQR, interquartile range; LUTS, lower urinary tract symptoms; m, months; MSHQ-EjD, Male Sexual Questionnaire - Ejaculatory Dysfunction; PV, prostate volume; PVR, post-void residual; Qmax, maximum urinary flow rate; QoL, quality of life; RCT, randomized controlled trial; TRUS, transrectal ultrasound; TPLA, transperineal laser ablation; TURP, transurethral resection of the prostate; US, ultrasound.
General advantages and disadvantages of TPLA.

LA, Local anaesthesia; GA, General anaesthesia; TPLA, transperineal laser ablation.
Complications
In three studies, no complications were recorded.13,19,20 Clavien-Dindo grade I complications were most commonly transient hematuria and dysuria, while acute urinary retention requiring re-catheterization and urinary tract infections/orchitis were the most commonly reported grade II complications. A prostatic abscess requiring drainage and prolonged course of antibiotics was the only grade III complication reported. Complication rates ranged between 1.9% and 2.3% for hematuria, 3.7% and 36.3% for dysuria, 1.9% and 19% for acute urinary retention, 0.6% and 9.1% for orchitis/urinary tract infections, and 0.6% and 4.8% for prostatic abscess formation. All complications are listed in Table 4.
Sexual function
Six studies evaluated erectile function and ejaculation postoperatively.10,15–18,20 Pacella et al. 18 reported a loss of ejaculation in 1.2% of patients, while de Rienzo et al. 16 reported no change in the IIEF questionnaire, while ejaculation returned to baseline after 3–6 months. Frego et al. 15 showed that ejaculation was preserved in 95.6% of patients, while no IIEF change was noticed at 12 months of follow-up, although only 45.5% completed the questionnaire at this timepoint. 15 Similarly, all patients retained erectile function and ejaculation in the study by Manenti et al., 17 with a mean score of ejaculatory function, as assessed by the Male Sexual Questionnaire – Erectile Dysfunction (MSHQ-EiD) questionnaire, showing improvement. Sessa et al. 20 reported preserved ejaculation in all patients and improvement in 15–29%, while erections were stable or even showed some improvement (+2–4%). Finally, Bertolo et al. 10 in their RCT showed that 96% of patients who underwent TPLA preserved their ejaculation.
Comparative studies
Two comparative studies reported the effectiveness and safety of TPLA compared to PAE 12 and TURP. 10 Cai et al. 12 found that both treatments led to improvement compared to baseline for functional outcomes, but no significant differences existed between them. Bertolo et al. 10 reported that both TURP and TPLA were effective in reducing symptoms and improving objective outcomes postoperatively at 6 months of follow-up, but TURP was superior in terms of Qmax improvement (+14.9 versus +5.4 ml/s, p < 0.001), while statistically nonsignificant differences were found regarding PVR reduction, IPSS, and QoL improvement. 10 At 1-month follow-up, 96.2% of TPLA patients retained their ejaculation, in contrast to 28% of TURP patients (p < 0.001) while the IIEF-5 score was similar between groups. 10 More patients in the TURP group were satisfied with their treatment compared to the TPLA group (80% versus 50%, p = 0.02) at 1 month postoperatively. 10
Discussion
The armamentarium for surgical management of BPH has rapidly evolved over the last 10 years. Besides MIST such as TURP and Holmium Laser Enucleation of the Prostate (HoLEP), further development of instruments and miniaturization of tools permitted the design of ultra-minimally invasive surgical techniques (uMIST), including steam injection (Rezu¯m), PAE, intraprostatic injections, insertion of prostatic urethral lift, and iTIND. 21 A recent systematic review and meta-analysis revealed that uMIST can reduce IPSS by 9.8 points, increase Qmax by 3.7 ml/s and decrease PVR without affecting erectile function and QoL, which are commonly affected when using MIST.21,22 One of the most recent additions is the TPLA, with accumulating evidence showing that this is an effective and safe technique.23,24 Two recent systematic reviews of the literature demonstrated the improvement in functional outcomes with simultaneous low complication rates and preservation of sexual function in the majority of patients;23,24 yet, the literature search was confined to a period ending in August 2022, since when a number of new clinical studies have been released. In our updated systematic, we included new evidence, including the first reported RCT on TPLA comparing it with TURP.
Findings from this systematic literature review indicate that most studies do not report in detail the perioperative management of patients; antibiotic coverage is usually prescribed within an hour from the procedure and up to 7 days, using cephalosporins and quinolones, while a common practice is also the administration of steroids to reduce the edema by their anti-inflammatory effect. 20 The decision of when is the appropriate timepoint for catheter removal was also variable, with most patients having it successfully removed after at least 7 days of catheterization. Based on the histopathological findings from an animal study, Liu et al. 11 proposed that the catheter should stay in situ for at least 7 days postoperatively since they observed that PV is increased for the first week, most likely due to inflammatory changes induced by laser energy application. 11 Bertolo et al. 10 reported a high acute urinary retention rate (19.2%), which was mostly seen in patients with early catheter removal at 3–4 days, thus confirming the aforementioned hypothesis. 10 Rest complication rates were low with 0% need for transfusion, 1.9–2.3% hematuria, 3.7–36.3% dysuria, 0.6–9.1% urinary tract infections, and 0.6–4.8% prostatic abscess formation.
Functional outcomes were improved in the vast majority of studies. Importantly, as highlighted by de Rienzo et al., 16 there seems to be a progressive improvement becoming more evident after 3–6 months. Tafuri et al. 24 reported a pooled Qmax at baseline of 8.69 ml/s, which improved among all timepoints (3 months, 13.17 ml/s; 6 months, 14.55 ml/s; and 12 months, 17.12 ml/s). Similarly, PVR decreased from 91.94 ml at baseline, to 36 ml at 3 months, 27.57 ml at 6 months, and 22.27 ml at 12 months. 24 IPSS decreased from a mean of 20.96 at baseline to 9.8 at 3 months, 6.92 at 6 months, and 6.4 at 12 months, with a similar decrease at the QoL component. 24 Although these pooled outcomes are more easily comprehended, the strength of evidence is low since they are derived from single-arm observational studies. Nevertheless, more recent data confirmed TPLA effectiveness among all of these objective and subjective outcomes. Minafra et al. 25 recently published an updated 3-year follow-up of their pilot studies, with 20 men who underwent TPLA and found a sustainable effectiveness, with IPSS being reduced by 37.2%, Qmax increased by 45.8%, PV decreased by 20.4%, and questionnaire scores related to sexual function improved by 60%, compared to baseline.
Sexual function preservation undoubtedly drives a decision during patient counseling for choosing BPH treatment options, especially in younger men. A recently published RCT by Bertolo et al., 10 focused on the evaluation of sexual function after TPLA in comparison to TURP. At the 1-month follow-up visit, 96% of the TPLA group retained ejaculation in contrast to 28% of patients who were assigned to TURP. 10 Importantly, TPLA did not differ significantly in terms of IPSS/QoL improvement and PVR reduction but was inferior to TURP in terms of Qmax increase. 10 Bladder neck preservation, along with sparing the muscular tissue surrounding the verumontanum, is considered the major component for avoiding retrograde ejaculation, 26 while the reduction in PV potentially permits better sperm flow. 17
This systematic review suffers from specific limitations derived from the design of included studies, which in the majority were observational and with a small sample size, thus adding the inherent limitations of these types of studies such as selection bias. In addition, due to the lack of comparative studies using the same groups, no meta-analysis was performed and results are presented in a systematic way. Nevertheless, this is an updated systematic literature review for TPLA adding the results of the first reported RCT on this technique.
Conclusion
TPLA of the prostate is an innovative, minimally invasive technique for managing patients with BPH. Existing studies indicate an effective technique in reducing IPSS and QoL scores, PVR reduction, and increase in Qmax, albeit the measured improvements in terms of Qmax are not equal to TURP. Although sexual function, namely ejaculation and erectile function are maintained in contrast to more invasive techniques, the mean catheterization time is 7 days and some studies report a rate of acute retention close to 20% after catheter removal. This technique can be offered as an alternative to patients, but it is important to mention that no long-term data are available for most patients, in the existing studies.
Supplemental Material
sj-docx-1-tau-10.1177_17562872231198634 – Supplemental material for Transperineal laser ablation as a new minimally invasive surgical therapy for benign prostatic hyperplasia: a systematic review of existing literature
Supplemental material, sj-docx-1-tau-10.1177_17562872231198634 for Transperineal laser ablation as a new minimally invasive surgical therapy for benign prostatic hyperplasia: a systematic review of existing literature by Lazaros Tzelves, Santhosh Nagasubramanian, Alexandros Pinitas, Patrick Juliebø-Jones, Sanjeev Madaan, Giampaolo Sienna and Bhaskar Somani in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.