
Abstract
Background and aims:
Prostatic urethral lift (Urolift™) is a minimally invasive technique to treat male lower urinary tract symptoms (LUTSs) due to benign prostatic hyperplasia (BPH). The aim of the present study was to assess safety and medium- to long-term outcomes in the relief of urinary symptoms.
Methods:
We included 35 men, affected by severe symptomatic BPH evaluated by International Prostate Symptom Score (IPSS), with normal erectile function (EF) and ejaculatory function (EjF) evaluated by the International Index of Erectile Dysfunction (IIEF-5) and Male Sexual Health Questionnaire for Ejaculatory Dysfunction (MSHQ-EjD-SF). Exclusion criteria were prostate larger than 70 cm3, bladder neck sclerosis, concomitant third prostatic lobe, and/or other cervical urethral obstruction or cancer. All patients, preoperatively, performed uroflowmetry (UFM) with peak flow (Q-max) and post void residual volume (PVR), digital rectal exam, transrectal prostate ultrasound to measure prostate volume, PSA, and cystoscopy. Follow-up was scheduled at 1–3–6 months, then yearly, evaluating UFM, IPSS, IIEF-5, and MSHQ-EjD-SF.
Results:
All procedures were performed by a single senior surgeon and follow-up was 33.8 ± 12 months. Preoperative PSA was 0.82 ± 0.4 ng/ml and mean operative time was 19.6 ± 10 min and 3 (2–4) implants per patient were used. Parameters reported at last follow-up schedule were: Q-max increase of 68% (p = 0.001), PVR reduction 68% (p = 0.005), and IPSS reduction 55% (p < 0.0001). EF and EjF were similarly preserved, and no patients presented retrograde ejaculation. A total of 88.6% of patients were satisfied with LUTSs improvement and 100% satisfied with EjF.
Conclusion:
Urolift can improve urinary disorders secondary to BPH, preserving EjF and EF. It is a safe and easy method, reproducible, and with low incidence of complications. Careful selection of patients is mandatory. The main reason for dissatisfaction is the higher expectation of better BPH symptoms relief although patients with high bladder neck and/or prostate volume >45 cm3 were aware of the possible failure.
Introduction
In 2002 IT was estimated that 15 out of 1000 men every year are diagnosed with lower urinary tract symptoms (LUTSs) due to benign prostatic hyperplasia (BPH). 1 LUTS severity is influenced by the patient’s lifestyle and country of origin; 2 however, age is the most important clinical factor.
The histologic prevalence of BPH increases from 8% to 50% between the fourth and sixth decade of age, 3 whereas LUTS from BPH occurs in up to one-quarter of males by age 50 years. While in younger men incidence rates are much lower, the impact of the disease and its treatment on patients’ quality of life may be higher.4,5 Indeed, male LUTSs may be associated with sexual satisfaction disorders due to erectile dysfunction and ejaculatory dysfunction (EjD). 6 Furthermore, medical (5 alpha reductase inhibitor and alpha blockers) and surgical therapies [simple prostatectomy, transurethral resection of the prostate (TURP), and laser enucleation] may cause retrograde ejaculation and/or worsen erectile function. 7
A recent trial showed that the majority of BPH patients are more interested in preserving their sexual health than resolving their urinary symptoms (95% versus 92%). 8 These issues often discouraged younger patients in performing any kind of procedure.
About 8 years ago, the Food and Drug Administration approved Urolift™ as a minimally invasive, effective, and safe procedure for the treatment of BPH, preserving prostate tissue and ejaculatory function. Multiple small permanent suture-based implants are delivered under cystoscope guidance, resulting in an opening of the prostatic urethra leaving a continuous anterior channel through the prostatic fossa extending from the bladder neck to the verumontanum. 9
The procedure may not require spinal or general anesthesia and allows an early return to daily activities. 10 Additionally, compared with traditional BPH surgical treatments, Urolift has been shown to be the only option allowing preservation of ejaculation in almost 100% of patients 11 and, since 2019, European Association of Urology (EAU) guidelines strongly recommend Urolift for the treatment of men with LUTS interested in preserving ejaculatory function, with prostates <80 cm3 and no third lobe. 12
The aim of the present study was to evaluate medium- to long-term functional results in terms of LUTS improvement and to evaluate safety and ejaculatory function in a population of patients affected by BPH symptoms treated with Urolift.
Materials and methods
Study population
After local institutional review board approval (Ethical Committee at the University Hospital ‘Ospedali Riuniti’, Foggia, Italy – Protocol 155/CE/2017 authorization number 618 of 18 December 2017), we retrospectively reviewed our BPH database to evaluate outcomes of patients treated with Urolift. Preoperatively, all patients were informed about all surgical treatment options and signed a written informed consent to participate in the study.
Patients with moderate to severe LUTSs as evaluated by International Prostate Symptom Score (IPSS), and with normal erectile function (EF) and ejaculatory function (EjF) according to the International Index of Erectile Dysfunction (IIEF-5) and Male Sexual Health Questionnaire for Ejaculatory Dysfunction (MSHQ-EjD-SF) were enrolled. Further, satisfaction rates were assessed by asking to answer ‘Yes’ or ‘No’ at each follow-up to the questions ‘Are you satisfied with urinary function?’ and ‘Are you satisfied with ejaculatory function?’.
Urolift was not offered to patients who were not primarily motivated to preserve EjF. Additionally, patients with prostate volume (PVol) higher than 80 cm3, bladder neck sclerosis, third lobe, and/or other cervical urethral obstruction were excluded.
According to our protocol, all patients preoperatively underwent uroflowmetry (UFM) with evaluation of the peak flow rate (Q-max) and post void residual volume (PVR), urinalysis, digital rectal exam, transrectal prostate ultrasound to measure PVol, PSA, and cystoscopy. If necessary, a urodynamic examination was performed before surgery.
Patients with less than 2 years of follow-up were excluded in order to evaluate medium- to long-term functional outcomes.
Urolift procedures
The Urolift system (Urolift™; Neotract Inc., Pleasanton, CA, USA) requires a 2.9 mm 0° lens and a 20F cystoscopy tube with custom bridge.
It is a single-use delivery device that consists of three elements: the nitinol capsular tab to the prostate capsule and a stainless-steel urethral end piece tensioned by a permanent polyethylene pterephthalate suture. By endoscopic transurethral, under vision, after mechanical compression of the prostatic lobe, the nitinol anchor is passed through the parenchyma and anchored to the prostate capsule. Then, the implant is released from the control of precise triggers.
The devices were placed laterally, 1.5 cm distal to the bladder neck, released at 20–30° to the right and left of 12 o’clock position. The intent of the technique was to enlarge the prostatic urethra as much as possible, likewise additional devices may be released, until the desired result is achieved. Enlargement can be verified with cystoscopy anterior to the verumontanum.
All procedures were carried out by a single senior surgeon (PA) under spinal anesthesia. A urethral catheter was left in place and removed on postoperative day 1 before discharge.
Statistical analyses were performed using Stata-SE 15 (StataCorp LP, College Station, TX, USA). All tests were two-sided with a significance level set at p < 0.05.
Follow-up visits
Follow-up visits were scheduled at 1, 3, 6, and 12 months after the procedure and then annually. An independent investigator (ND) assessed functional outcomes objectively and subjectively.
Objective evaluation was performed by UFM with measurement of PVR. IPSS, IIEF, and MSHQ-EjD-SF were administered for subjective assessment and patients asked whether they were satisfied with urinary or sexual function at each appointment.
At month 6, all underwent flexible cystoscopy to assess prostatic urethral enlargement, to exclude erosions or extrusions of the capsular tab into the bladder, and to exclude post-surgical urethral stenosis in the case of severe worsening of the urinary flow. PSA was repeated at 6 months and then according to risk factors.
Results
Data were collected on 35 BPH patients with a mean age of 50.5 ± 11 (21–78) years, who consecutively underwent Urolift from March 2013 to March 2019. Of these, 18/35 (51.4%) were younger than 50, 13/35 (37.1%) up to 60, and 4/35 (11.4%) over 60 years. Every patient has more than two years of follow-up and median last follow-up 33.8 (24–63) months. Median PSA was 0.82 (0.2–1.7) ng/ml preoperatively, and 1.2 (0.3–4) ng/ml six months after surgery. Median PVol was 31.4 (18–67) cm3. Median operative time was 19.6 ± 10 (10–45) minutes and average of 3 implants (2–7) per patient were used. They were usually discharged the day after surgery, once the foley had been removed, or with the indwelling bladder catheter in the case of complications.
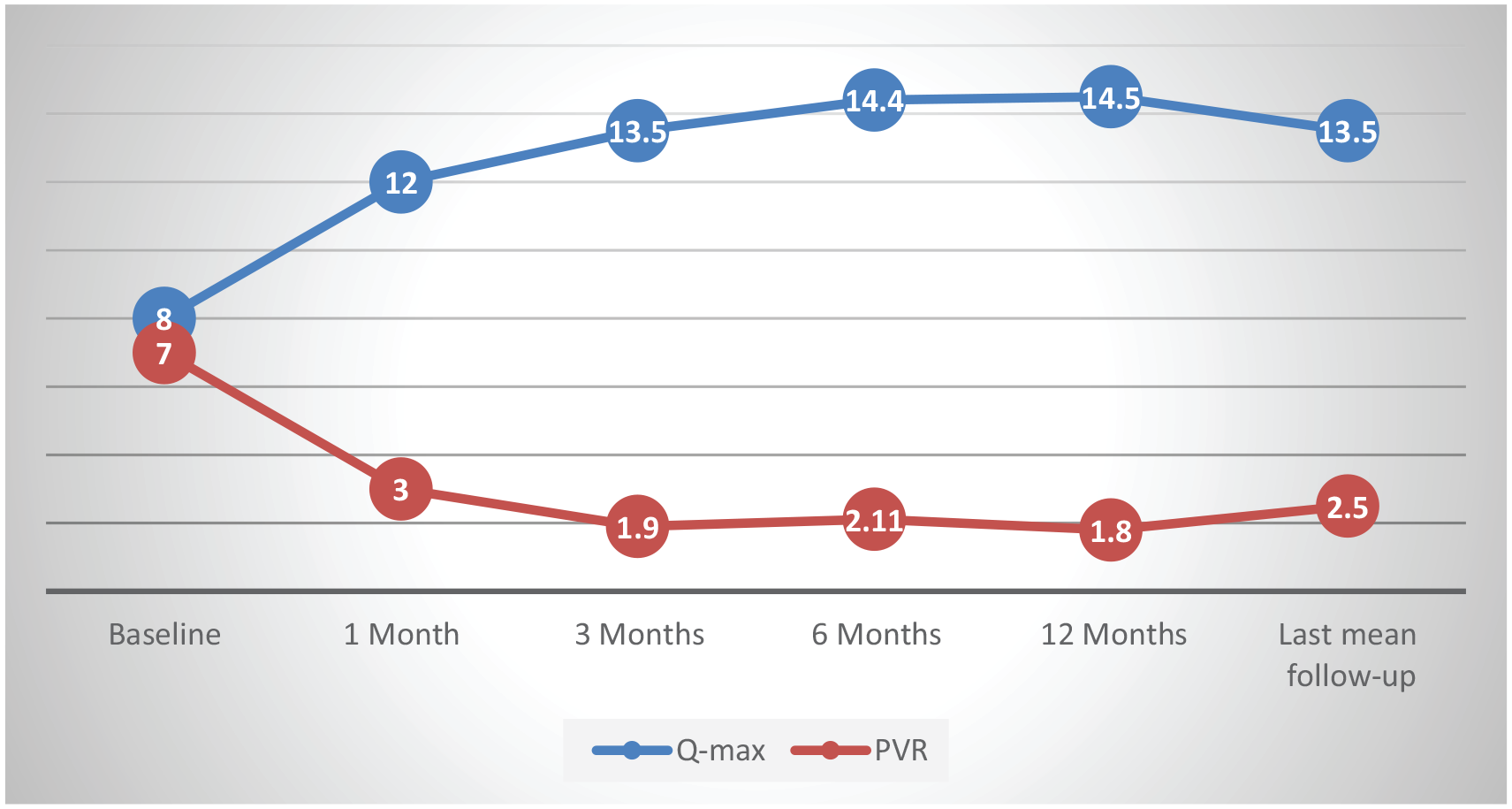
Functional outcomes are reported in Table 1 and Figure 1, and subjective results in Figure 2. At the last follow-up, a median Q-max increase of 68% (p = 0.001), a PVR reduction of 68% (p = 0.005), and an IPSS reduction of 55% (p < 0.0001) were observed. EF and EjF were preserved in every patient, and no one presented retrograde ejaculation. Most symptoms were moderate to severe and resolved within four weeks after the procedure and remained stable until the last follow-up.
Functional outcomes at follow-up.

Data are reported as median (interquartile range).
IIEF-5, International Index of Erectile Dysfunction; IPSS, International Prostate Symptom Score; MSHQ-EjD-SF, Male Sexual Health Questionnaire for Ejaculatory Dysfunction; PVR, post void residual volume; Q-max, peak flow rate; VV, voided volume.
Functional outcomes at follow-up visits.

Subjective outcomes at follow-up.
Overall, 88.6% (31/35) of the patients at last follow-up were satisfied with LUTS improvement and would recommend the procedure. All (35/35) were satisfied with EjF.
For persistence of LUTSs, 4/35 (11.4%) patients required retreatment: two patients at 26 months underwent TURP while two rejected it to preserve EjF and were unsure whether to undergo retreatment. One patient, for urethral stricture, underwent endoscopic urethrotomy resolving urinary LUTS.
Unsatisfied patients had a PVol >45 cm3 or a slight high bladder neck at cystoscopy. All other satisfied patients had a PVol not more than 45 cm3 and without slight high bladder neck. One patient, with familiarity for prostate cancer, 26 months after surgery underwent radical prostatectomy for localized prostate cancer.
None showed pelvic pain or dysuria. Most patients returned to their day activities after discharge. Acute urinary retention occurred in two patients after catheter removal (managed with placement of transurethral catheter leg bag for 7 days, grade 2 complication according to Clavien–Dindo classification) and one patient had hematuria requiring hemostatic endoscopic intervention (grade 3a), the only patient discharged three days after surgery.
Statistical analysis
Outcomes of this study were urinary function according to Q-max, PVR, voided volume and IPSS, and sexual function assessed with IIEF and MSHQ.
Descriptive statistics was performed for the overall population. Continuous variables were reported as median and interquartile range at each follow-up and compared by the Mann–Whitney U-test whereas categorical variables were reported as rates and tested by the Fisher’s exact test or the chi-square test, as appropriate. Statistical analyses were performed using Stata-SE 15 (StataCorp LP, College Station, TX, USA). All tests were two-sided with a significance level set at p < 0.05.
Discussion
The choice of surgical treatment for patients affected by symptomatic BPH is a highly debated topic. In recent years we have witnessed an evolution of mini-invasive surgical approaches to benign urological diseases. When proposing treatments, in some cases, we should not only think about obtaining the best functional urinary outcome. The effects of an invasive treatment can influence the psychological aspect of the patients and the well-being of the couple, especially in younger patients. 13 In order to tailor surgical management to patient preferences, Urolift may represent a valid option in the urologist’s armamentarium, being the only currently available technique that can guarantee 100% ejaculation preservation.8,14
In this scenario, every man younger than 50 years old or motivated to preserve EjF should be offered such procedure. Our data showed preservation of sexual function in all patients, with a medium- to long-term improvement in Q-max and PVR of 68% (p = 0.0001) resulting in a significant drop in IPSS score of 55% (p = 0.001).
Since many options are available for the treatment of BPH, the question remains of optimal patient selection for each treatment. At present, EAU Guidelines suggest a different surgical therapy based on the patient’s ability to receive anesthesia, cardiovascular risk, and PVol. Independently of the size of the prostate, laser surgery is recommended as a solution in high-risk patients who cannot discontinue antiplatelet or anticoagulant therapy. In all other cases, the choice is evaluated only on the basis of prostate size, so that in prostates up to 30 g and between 30 g and 80 g, TUIP and TURP are the gold standard, respectively, compared with the other techniques. 12 As shown in a meta-analysis of 23 studies with a total of 2245 patients who underwent TURP for prostate up to 80 g, the improvement of Q-max and PVR can be up to 162% and 77% respectively, with a 70% reduction in IPSS. 15 TUIP (trans urethral incision of the prostate)
As reported in a prospective multicenter study by Reich in 2008, in about 10,000 patients undergoing TURP, Q-max increased significantly to 21.6 ± 9.4 ml/s (from 10.4 ± 6.8 ml/s, p < 0.0001), while PVR decreased to 31.1 ± 73 ml (from 180.3 ± 296.9 ml, p < 0.0001). 16 Despite good urinary functional results reported in the literature, the risk of complications remains high and up to 11%.16,17 Furthermore, resection of prostate tissue can lead to erectile dysfunction from 3.4% to 32% and EjD from 53% to 72%. 18 Ejaculation-sparing TURP techniques have been suggested; still about 10% of patients experience EjD. 19 Laser techniques reduce postoperative complications mainly in terms of bleeding and hospital stay, 20 and comparing the results of laser with TURP, at 5-year follow-up, IPSS was reduced up to 70%, whereas anejaculation occurred in 88% of patients. 21 Interesting long-term results (4 years) were reported on using water vapor thermal therapy (Rezum, Boston Scientific, Marlborough, MA, USA) in a multi-center randomized sham-controlled trial that showed how Q-max improved by 50% and IPSS reduced of 47% with low retreatment rate (4.4%). It is possible to treat patients with mild third lobe or central adenoma, characteristics that would expose the Urolift to minor urinary outcomes. Although it is minimally invasive, it is still an ablative technique, requiring an indwelling catheter for about 2 weeks and at least 3 months before seeing its effectiveness. 14 Image-guided robotic waterjet ablation (AquaBeam, PROCEPT BioRobotics Inc., Redwood Shores, CA, USA) is characterized by targeted high-speed saline flow that ablates prostate lobe in real-time ultrasonography, with improvements in IPSS compared with TURP (respectively −16.9 and −15.1). Larger prostates (50–80 cm3) demonstrated greater benefit although the technique was exposed to higher postoperative complications than TURP (42% versus 26%). 14 Similarly, as shown in a recent study, other novel minimally invasive technologies, such as iTIND, and prostatic arterial embolization showed a significant improvements in LUTSs, with a minor but not negligible risk of EjD compared with Urolift, where EjD risk is zero and urinary results are immediate. 14
In 2019, the Urolift was added in the European guidelines to TURP and lasers, with a ‘strong’ recommendation (level of evidence 1a) for surgical treatment of BPH in patients motivated to preserve ejaculation, with prostates less than 80 g and in the absence of a third lobe. 12
As we know, TURP showed better urinary objective outcomes than Urolift. But, in a study comparing TURP versus Urolift involving 10 European centers with a total of 80 patients and up to 2 years’ follow-up, the TURP arm had superior urinary outcomes in terms of Q-max and IPSS (5 versus 15.8 points, p = 0.002; −9.2 versus −15.3 points, p = 0.004). However, improvements in terms of IPSS quality of life, BPH impact index and PVR reduction were similar between the two techniques (−2.5 versus −3.3 points, p = 0.066; −4.1 versus −5.4 points, p = 0.131; −10.6 versus −42.5 ml, p = 0.091). 22 Similar results was reported by Sønksen in a 1:1 randomized trial with 2-year follow-up comparing TURP and Urolift. Both improve LUTSs; also here there was no significant difference between IPSS quality of life and BPH impact index (−2.8 versus −3.1 points, p = 0.4; −5 versus −5.2 points, p = 0.8), while better IPSS and Q-max were confirmed in the TURP arm (−11. 4 versus −15.4 points, p = 0.02; 4 versus 13.7 points, p < 0.0001) with a significant improvement also of PVR (−7.4 versus −70 points p = 0.002) in respect to the findings of Gratzke. 23 In this situation, it can be seen that adenomectomy techniques with or without sparing of the ejaculatory ducts certainly restore a greater urinary flow than recent devices; the subjective perception of improvement demonstrates the same result in subjective evaluations administered to patients both in the short and the long term. So, apparently, a large debulking was not always necessary.
Given the results, in selected patients, the same benefit can be expected in the medium to long term.
A drawback of the technique is the higher retreatment rate with Urolift (up to 13.6% at 4 years of follow-up) compared with TURP (11% versus 6%).10,22,24 Similarly, retreatment was necessary in 11.4% (4/35) of our patients for persistence of symptoms. Over time, we realized that the failed patients had a prostate greater than 45 cm3 or a slightly high bladder neck, so we subsequently decided not to offer the Urolift to patients with these preoperative characteristics.
Jones et al. 9 reported the issue of prostate volume as a limitation of the procedure, in that it is feasible in oversized prostates but offers suboptimal long-term outcomes, as there is often central obstructive adenoma that is not well controllable with Urolift.
In the LIFT study, a prospective randomized controlled study involving 19 US centers and with 206 patients randomized 2:1 to the Urolift procedure or blinded control, Roehrborn showed mean significant improvements in IPSS, quality of life, and Q-max (41.1%, 48.8%, 53.1%), that were statistically significant at 3-year follow-up, with approximately 10% retreatment and mild adverse events. 25 The five-year follow-up showed a durable improvement in IPSS and Q-max of 36% and 44% respectively. Sexual function was stable over 5 years with no de novo sustained erectile dysfunction or EjD. 10 The difference in the urinary long-term improvements of the IPSS between our study and Roherborn’s (55% versus 36%) is probably attributable to the lower mean age (50 versus 67 years) and lower prostate volume (31 versus 44 cm3), parameters directly related to the increase in IPSS over time. 26 Other minor, but no less important, reasons that may have contributed to better outcomes over time are that they included patients with baseline mild-to-moderate erectile dysfunction (IIEF 13 versus 20) and lower EjF (MSHQ-EjD-SF 8.7 versus 11). We excluded patients with erectile dysfunction or EjD, because if present they were offered a different surgery, as they were probably interested in better resolving the urinary disorder. The inhomogeneity of the starting data then probably led them to a higher long-term urinary dissatisfaction (11.4% versus 18%); however, the correct and accurate prospective data collection led both to show the discrete functional results of the Urolift that were then overlapping. The common limitations of both, compared with studies of traditional techniques, were the exclusion of prostates with third lobe or greater than 80 cm3, although, unlike them, over time, we did not further propose Urolift to patients with medium to large prostates. 25
Considering literature reports, ideal candidate patients for this procedure are young and sexually active patients and with not large prostate, but this minimally invasive technique is exposed, however, to high 5-year retreatment rates ranging 22.9–48% 27 with an annual rate, according to Miller on 2000 patients, of 6% per year. 28
In our hands and from our results, the main limitation of this technique is represented by correct selection of patients, who should undergo a complete preoperative evaluation. Even if we performed all procedures with small prostates (up to 80 g), without third prostatic lobe, and in patients motivated to preserve ejaculation, all patients with high bladder neck and those with PVol greater than 45 cm3 reported unfavorable results, declaring themselves dissatisfied with the technique.
Although several authors do not consider volume to be a limitation for the technique and that the third prostatic lobe can be anchored and displaced with acceptable functional results, we did not enlist them in our initial experience.29,30
The main limitations of the present study are the retrospective nature of the study, the lack of direct comparison with other techniques, and the small sample size. However, there are several strengths such as the ability to test the effectiveness of the treatment in carefully selected patients and a medium- to long-term follow-up.
Further comparative studies with other minimally invasive techniques may be necessary to confirm these results.
Conclusion
Urolift is a viable, safe, and durable minimally invasive surgical technique for the treatment of symptomatic patients with BPH, especially if young, who are motivated to preserve EjF. Careful patient selection is critical to achieve improved and long-term functional outcomes. The technique was successful in terms of maintenance without impairment of EjF. In addition, the procedure has been fast, safe, feasible, and with immediate results.
Therefore, this technique should be part of every urologist’s clinical background as a minimally invasive surgical approach tailored in sexually active patients suffering with BPH.
Footnotes
Author contributions
Conceptualization, Nicola d’Altilia, Pasquale Annese; Data curation, Nicola d’Altilia, Ugo Giovanni Falagario, Francesco Del Giudice; Formal analysis, Ugo Giovanni Falagario, Matteo Ferro; Investigation, Nicola d’Altilia, Pasquale Annese, Vito Mancini; Methodology, Gian Maria Busetto, Ugo Giovanni Falagario, Giuseppe Carrieri, Ottavio de Cobelli; Project administration, G.M.B., F.S. and E.R.; Supervision, Ottavio de Cobelli, Matteo Ferro, Angelo Porreca, Vito Mancini; Writing – original draft, Nicola d’Altilia; Writing – review & editing, Gian Maria Busetto, Ugo Giovanni Falagario, Matteo Ferro.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.