
Abstract
Background:
Research on the use of tissue interposition flaps (TIFs) in vesicovaginal fistulae (VVF) repair is a broad area where a very wide range of natural and synthetic materials have been used. The occurrence of VVF is also diverse in the social and clinical settings, resulting in a parallel heterogeneity in the published literature on its treatment. The use of synthetic and autologous TIFs in VVF repair is not yet standardized with a lack of the most efficacious type and technique of the TIF.
Objectives:
The aim of this study was to systematically review all synthetic and autologous TIFs used in the surgical repair of VVFs.
Data sources and methods:
In this scoping review, the surgical outcomes of autologous and synthetic interposition flaps used in VVF treatment meeting the inclusion criteria were determined. We searched the literature using Ovid MEDLINE and PubMed databases between 1974 and 2022. Study characteristics were recorded, and data on the change in fistulae size and location, surgical approach, success rate, preoperative patient evaluation and outcome evaluation were extracted from each study independently by two authors.
Results:
A total of 25 articles that met the inclusion criteria were included in the final analysis. A total of 943 and 127 patients who had received autologous and synthetic flaps, respectively, were included in this scoping review. The fistulae characteristics were highly variable with regard to their size, complexity, aetiology, location and radiation. Outcome assessments of fistulae repair in included studies were mostly based on symptom evaluation. Physical examination, cystogram and methylene blue test were the methods in order of preference. Postoperative complications, such as infection, bleeding, donor site, pain, voiding dysfunction and other complications, were reported in patients after fistulae repair in all included studies.
Conclusion:
The use of TIFs in VVF repair was common especially in complex and large fistulae. Autologous TIFs appear to be the standard of care at the moment, and synthetic TIFs were investigated in prospective clinical trials in a limited number of selected cases. Evidence levels of clinical studies evaluating the effectiveness of interposition flaps were overall low.
Keywords
Introduction
Vesicovaginal fistulae (VVF) is an abnormal communication between the bladder and the vagina that causes continuous urinary incontinence. 1 It has a significant negative impact on the psychosocial well-being and the quality of life of the women suffering from this condition. 2 VVF occurs mainly due to birth trauma and prolonged obstructed labour in the developing world. Whereas in developed countries, VVF mainly occurs after urogynaecologic interventions mainly for malignant disease and pelvic radiation therapy. Although the true incidence of VVF is unknown, it is estimated at 0.3–2%. 3 Estimates suggest that at least 2 million women, mainly those living in low-resource countries, suffer from VVF with 30,000–130,000 new cases occurring each year in Africa alone. 4
The management of VVF could be conservative or interventional based on fistulae characteristics, such as size, location and the surgeon’s experience. Conservative management strategies, such as continuous bladder drainage, catheterization and injection of therapeutic products [such as tissue adhesives and platelet-rich plasma (PRP)], are preferred for small-sized (< 1 cm) fistulae as first-line management. 5 The definitive treatment of VVF is surgical repair. During surgical repair, the fibrotic tissues around the fistulae are excised, and a tension-free and watertight closure of the fistulae is achieved. 6 In many cases, a well-vascularized tissue flap is placed between the bladder and vagina to ensure a successful outcome. 7 Tissue interposition flaps (TIFs) provide a barrier between the bladder and vaginal suture lines and they increase success by enhancing tissue formation and neovascularity. 8 Using an interposition flap for the treatment of VVF promotes healing and decreases the incidence of fistulae recurrence. 9
In the literature, both autologous and synthetic TIFs have been used. Autologous TIFs have been used more commonly compared to the synthetic ones, and the Martius flap is the most frequently used autologous TIF. Autologous TIFs have obvious advantages over the synthetic flaps, such as proven efficacy and lack of concerns regarding immunogenicity; however, they may not always be available for use and they are associated with donor site morbidity. Synthetic TIFs can be a good alternative with the advantages of being immediately available resulting in shorter operative times, no donor site morbidity and potentially better efficacy. So far, several products have been repurposed for use as a synthetic TIF in VVF repair, yet none of them gained widespread use by the international surgical community. These products are mainly tissue sealants and hemostatic agents that have been used by various surgical disciplines to control bleeding and enhance healing. In the literature, several synthetic TIFs have been used in clinical trials, such as fibrin glue and gelatin matrix. All synthetic TIFs were approved by the US Food and Drug Administration (FDA) for human use; however, none of them was designed and approved specifically for VVF repair. Up to date, despite recent advances in material sciences and design, a purpose-designed synthetic TIF that can satisfy the surgeons’ need for an additional layer of good-quality tissue in between suture lines during VVF repair has not been developed. This can explain the lack of widespread acceptance of synthetic flaps by the surgical community worldwide and their use appears to be limited to several case studies or small-scale clinical trials.
In this study, we have performed a scoping review for all the available autologous and synthetic TIFs used in VVF repair. We explored the types of TIFs used, material properties of synthetic flaps and the surgical outcomes.
Methods
This scoping review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 10 Studies included in the scoping review were examined in terms of study characteristics, efficacy outcomes, study methodology, follow-up period, distribution by country, preoperative–postoperative evaluation methods and postoperative complications.
A summary of the material characteristics of the synthetic TIFs that have been used so far is listed in Table 1. With the recent advances in biomaterials science, it could be expected that novel, purpose-designed synthetic TIFs could be offered in the market to improve surgical outcomes for patients with VVF.
A summary of material characteristics of synthetic TIFs.

Search strategy and definitions
We conducted a systematic search of the literature covering the period from 1974 to 2022 using Ovid MEDLINE and PubMed databases for all clinical studies reporting outcomes of VVF repair using autologous or synthetic TIFs used in VVF repair. We used vesicovaginal, gynaecologic, obstetric and genitourinary fistulae keywords to determine the main framework of the study. The research specified using keywords required for TIFs used in VVF repair.
The study protocol was prospectively constructed and published on an online repository on 22 June 2021 (https://data.mendeley.com/datasets/7fj8rmfps6/1) (doi: 10.17632/7fj8rmfps6.1).
Inclusion/exclusion criteria
The inclusion criteria were as follows: (1) all studies reporting results of patients who were diagnosed with VVF (prospective, retrospective trials, case–control studies and clinical case series with and without control groups); (2) the treatment intervention included an interposition flap; (3) objective and subjective outcome measures were clearly defined; (4) studies more than 10 patients. Studies were excluded if (1) patients have been diagnosed with another type of fistulae or gynaecological problems; (2) autologous/synthetic grafts were not used in VVF treatment; (3) studies less than 10 patients; (4) objective and subject outcome measures were not clearly defined; (5) studies were not full text available. Reviews, book chapters and conference abstracts were excluded from the scoping review.
Study selection
The PRISMA flow diagram was followed during the scoping review. First, all abstracts and titles found as a result of the search with the required keywords were screened. After abstract and title screening, records identified through database searching were analysed, and articles that did not meet the inclusion criteria were excluded (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of study selection.
Data extraction
Two independent investigators evaluated all the potentially eligible studies independently and performed the data extraction separately. Any disagreements that could not be reconciled by discussion were resolved by a third person.
The following data were extracted from each study independently by two researchers: (1) characteristics of included studies, (2) methodology of the study (retrospective, prospective, randomized), (3) definition of surgical success, (4) follow-up period for each case, (5) patients’ radiation therapy history, (6) control arm of the study, (7) preferred surgical approach, (8) the type of interposition flap, (9) fistulae characteristics, (10) preoperative evaluation, (11) outcome evaluation, (12) postoperative outcomes, (13) the success rate of studies and (14) distribution of studies by country. Throughout the search, data from patients diagnosed with VVF and who used autologous and synthetic TIFs in their treatment were collected. The included studies were analysed with the number of patients, the control arm of the study, surgical approaches and follow-up periods.
Clinical data of the patients were determined and fistulae characteristics were extracted from each study. Studies involving fistulae smaller than 1.5 cm and larger than 3 cm were considered in separate groups. In addition, fistulae with sizes between 1.5 and 3 cm, and whose size was not clearly defined in the study were classified as mixed and included in the third group. Data on the complexity of the fistulae were extracted from each study. The data on the aetiology of fistulae were also recorded. In addition, data on prior radiotherapy were extracted and included in fistulae characteristics.
Diagnostic tests used in the preoperative patient evaluation were recorded, and the number of studies using each method was reported. Likewise, different outcome evaluation methods after surgeries were recorded for each study. In addition, the postoperative complications reported in each study were recorded, and the use of standardized reporting systems (such as Clavien–Dindo classification) was indicated.
The surgical success rates were recorded as overall success, success after primary surgery and success after secondary surgery, following the reported numbers in each study. Included studies were also classified based on the Organization for Economic Co-operation and Development (OECD) data, as the occurrence and treatment of VVF may vary significantly in different parts of the world. 11 The distribution of studies according to countries, based on the OECD data, was analysed along with the number of patients and fistulae aetiologies. Studies were assigned to an OECD country based on the centre where the patients were operated.
Results
Study characteristics
A total of 25 articles that met the inclusion criteria were included in the scoping review. It has been provided that, 10 different types of autologous interposition flaps (Martius, omental, peritoneal, urachal, abdominis muscle, gracilis muscle, ileal segment, bladder wall, rotational bladder and Singapore flaps) and 7 different kinds of synthetic interposition flaps (Fibrin glue, cyanoarclic glue, small intestinal submucosa, acellular collagen matrix, oxidized cellulose, gelatin matrix and PRP) have been used in VVF repair surgeries. All studies were grouped arbitrarily into three groups with regard to the number of patients included: small (studies including < 10 patients), medium (studies including 10–50 patients) and large (studies including > 50 patients) (Table 2). Only studies that report outcomes for ⩾ 10 patients were included in the final analysis (n = 25).
Number of studies reporting on small (studies including < 10 patients), medium (studies including 10–50 patients) and large (studies including > 50 patients) patient groups.

Gracilis muscle flap, rotational bladder flap, Singapore flap, urachal flap, ileal segment flap.
A total of 943 and 127 patients who had received autologous and synthetic flaps, respectively, were included in this scoping review. The most commonly used autologous and synthetic interposition flaps were Martius Flap and the Fibrin glue, respectively. Included studies were also reviewed in terms of study design; three of them were prospective randomized controlled studies, two were prospective and the rest were retrospective case series. Furthermore, 5 of all included studies had control arms, and 15 studies had no control groups. In three of the studies, TIFs were compared with other surgical alternatives. When the preferred surgical approaches in the studies were examined, it was determined that nine transvaginal, nine transabdominal, two transvaginal injections, two both transabdominal/transvaginal and one transperitoneal approaches were used. In the studies reviewed, the duration of follow-up after VVF repair ranged from 3 to 66 months (Table 3).
Characteristics of included studies a randomized into trimming fistulae tract or not.
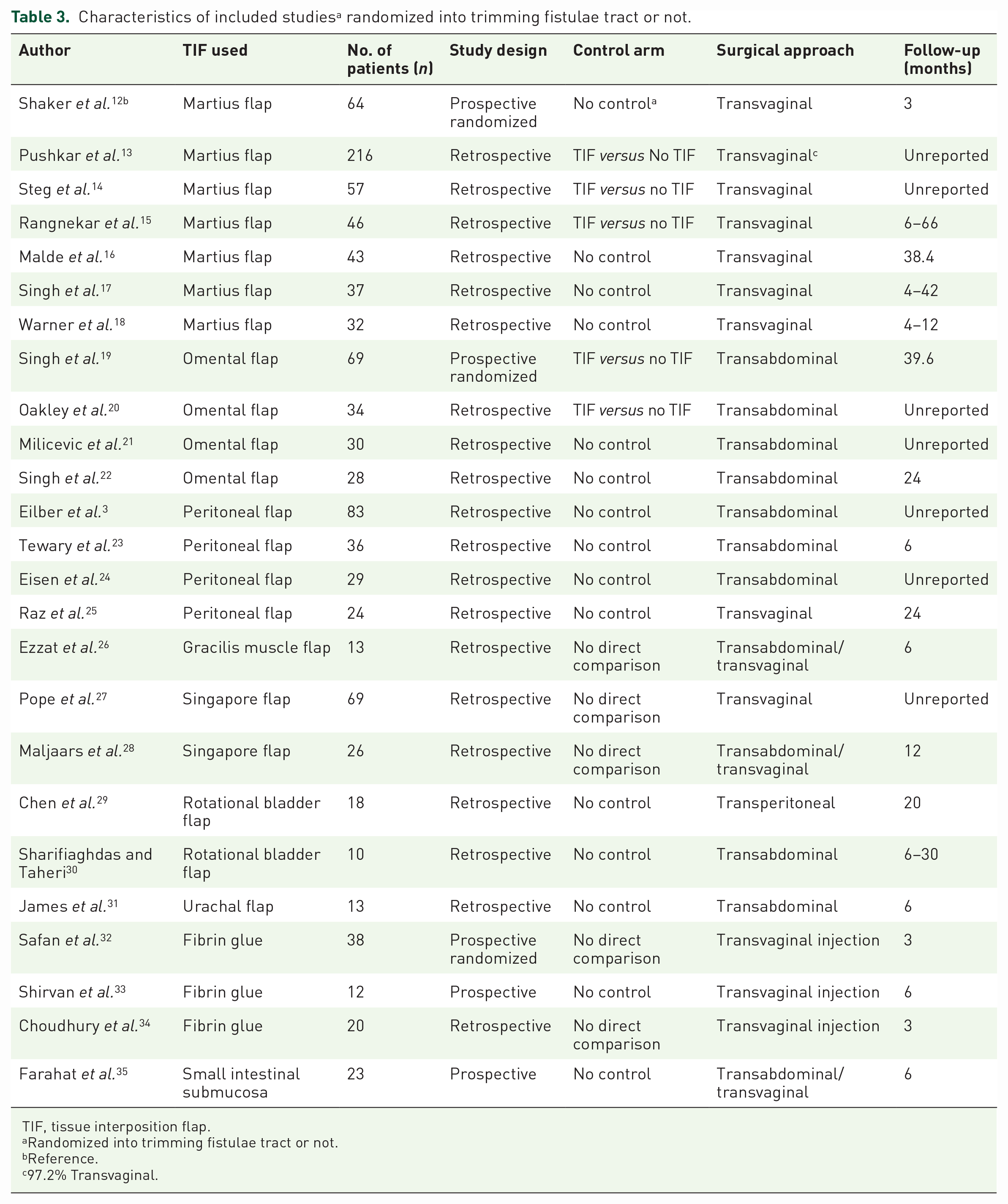
TIF, tissue interposition flap.
Randomized into trimming fistulae tract or not.
Reference.
97.2% Transvaginal.
The distribution of the number of patients by years is given in Figure 2. According to the graph, it is seen that the number of patients has increased over the years associated with an increase in the number of studies. This increase is particularly evident after 2000.

Distribution of the number of patients by years in included studies.
Fistulae characteristics
The fistulae characteristics were highly variable with regard to their size, complexity, aetiology, location and radiation. Fistulae sizes in 14 studies were mixed, < 1.5 cm in 7 studies and > 3 cm in 2 studies. Autologous flaps were commonly used in fistulae of 1–7.5 cm in size. A gracilis muscle flap was used to repair the largest fistulae of 7.5 cm in size. Synthetic flaps were used in fistulae of 5 mm–2.5 cm in size. Fistulae were analysed in terms of complexity; it was found that seven of the studies were primary and the others were mixed. The aetiology of VVF was mainly gynaecologic in the included studies, and in 12 of the studies, patients with radiation-induced fistulae were included. However, 14 of the studies were found to be gynaecologic, 7 of them were obstetric, 1 of them was both gynaecologic and obstetric, and 3 of them were unreported. Fistulae locations are clearly specified as posterior bladder wall, supratrigonal and bladder neck in three studies. Besides that, the fistulae locations were mixed in 15 studies, and locations were not specified in 7 studies.
In 12 of the studies, radiotherapy-induced VVF were included, whereas in the other 12, radiotherapy-induced fistulae were excluded. In one study, radiation status was unreported (Table 4).
The distribution of preoperative fistulae characteristics in included studies.
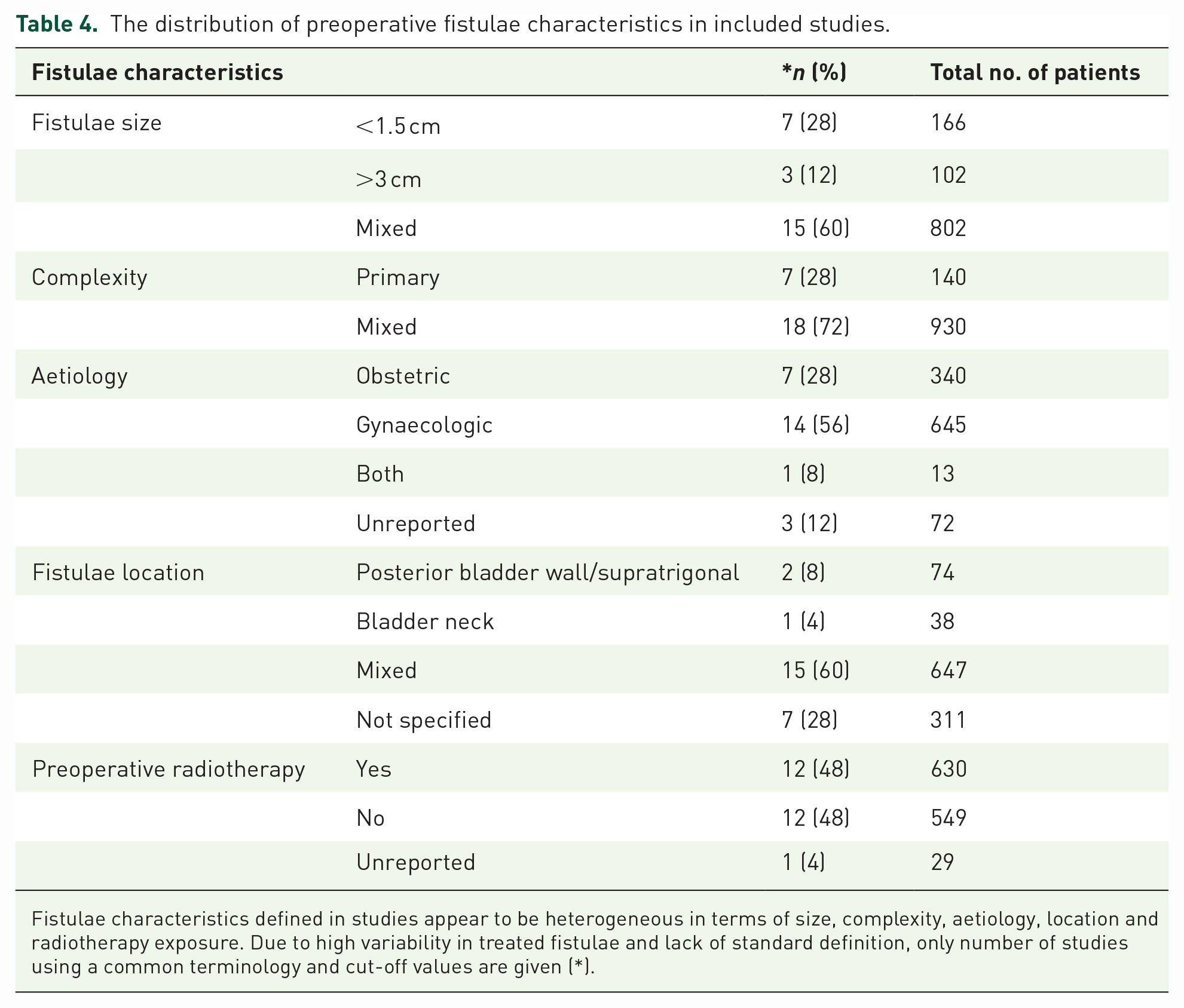
Fistulae characteristics defined in studies appear to be heterogeneous in terms of size, complexity, aetiology, location and radiotherapy exposure. Due to high variability in treated fistulae and lack of standard definition, only number of studies using a common terminology and cut-off values are given (*).
Preoperative diagnosis
In included studies, eight diagnostic tests were used for preoperative evaluation. Among these tests, the most commonly used one was cystoscopy and the least commonly used one was the methylene blue (three swabs) test. Other diagnostic tests were intravenous urography (IVU), computed tomography (CT)/magnetic resonance imaging (MRI), vesicoureteral reflux (VUD)/voiding cystourethrogram (VCUG) and urodynamics in the order of use from most to least. The diagnostic method was not defined in five studies (Table 5).
The method of preoperative patient evaluation used in each study.
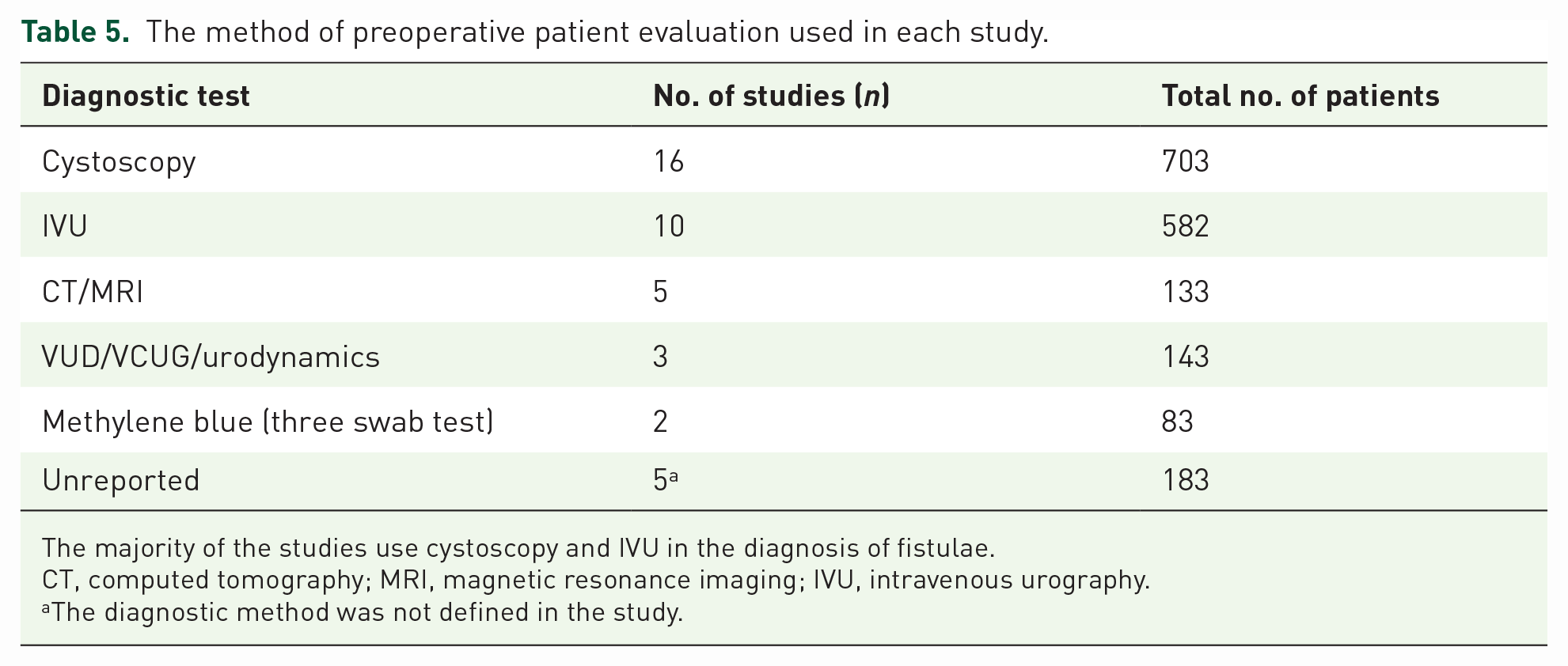
The majority of the studies use cystoscopy and IVU in the diagnosis of fistulae.
CT, computed tomography; MRI, magnetic resonance imaging; IVU, intravenous urography.
The diagnostic method was not defined in the study.
Postoperative outcome assessment
Outcome assessments of fistulae repair in included studies were mostly based on symptom evaluation. Physical examination, cystogram and methylene blue test were the methods in order of preference. The method of definition of surgical outcomes was not mentioned in eight studies (Table 6).
The method of definition of surgical outcomes used in included studies.

The surgical outcomes were mainly determined by symptomatic assessment of patients and physical examination.
Reported overall success rates after VVF repair surgeries were between 53.8 and 100. Five studies reported success rates after primary and secondary surgery separately. In 11 studies, success rates were reported individually for each group and 3 of these studies were prospective randomized (Supplemental Table 1).
Postoperative complications
Postoperative complications, such as infection, bleeding, donor site, pain, voiding dysfunction and other complications, were reported in patients after fistulae repair in all included studies. The most common postoperative complications were infection and voiding dysfunction. There were no postoperative complications in four studies. Postoperative complications were unreported in eight studies. Standardized reporting of postoperative complications was performed in only three of the studies.19,23,31 All postoperative complications are provided separately for each study in the Supplemental Table 2. Studies with a standardized assessment of complications (according to the Clavien–Dindo classification) are summarized in Table 7.
The postoperative complications reported after the VVF repair.

VVF, vesicovaginal fistulae.
Distribution of studies by country
The incidence of VVF differs between developed and underdeveloped countries. According to the distribution based on OECD data, 8 of the studies included in this scoping review belong to OECD member countries (32%) and 17 studies belong to non-OECD countries (68%) (Figure 2). The total number of patients in studies conducted in OECD member countries was 315 and in non-OECD countries was 755 (Figure 3).

Distribution of studies (n) by country as defined by the corresponding address.
The aetiology of the included studies was examined on the basis of countries; the aetiology of fistulae was gynaecologic in all studies belonging to OECD member countries and the success rates of these studies vary between 82% and 100%. In one study from OECD member countries, the aetiology of VVF was not reported. 24 In studies from non-OECD countries, fistulae origins were found to be both gynaecologic and obstetric. It is determined that the success rates of gynaecological VVFs are distributed between 80.4% and 100% while those of obstetric fistulas were distributed between 53.8% and 96.04%. The aetiology of VVF was not specified separately in two studies from non-OECD countries, it was accepted as mixed26,35 (Table 8).
The aetiology of fistulae, the country of study, OECD membership status and the success rate of fistulae repair are given in the table for each study separately.
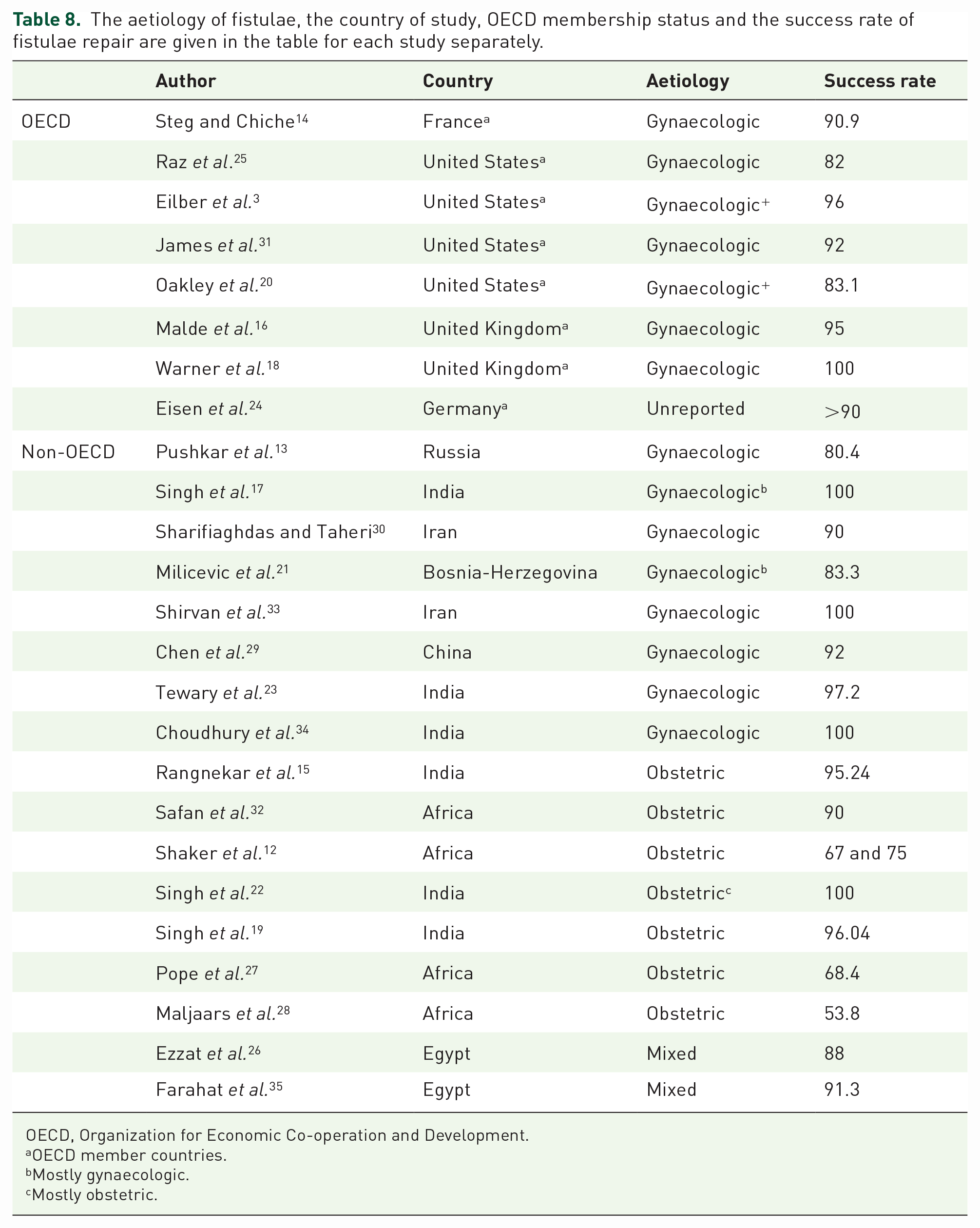
OECD, Organization for Economic Co-operation and Development.
OECD member countries.
Mostly gynaecologic.
Mostly obstetric.
Discussion
In this study we have, for the first time, systematically reviewed all autologous and synthetic TIFs used in VVF repair in terms of flap characteristics and surgical results. It appears that the autologous interposition flaps have been used more commonly than the synthetic ones when repairing VVF. Reported surgical success rates are equally high for both autologous and synthetic TIFs; however, most studies are prospective or retrospective cohort studies involving small patient groups. Indeed, the main finding of this article is that the available evidence base on the use of TIFs in VVF repair is rather weak with methodologically limited studies and significant heterogeneity between study findings. For example, most studies do not have appropriate controls and most of the studies did not report complications in a standardized manner making it difficult to comment on the safety of the two types of TIFs. Therefore, available evidence on the comparative efficacy and safety of autologous and synthetic TIFs in VVF repair is heterogenous and does not allow any conclusion to be made.
Nevertheless, we have seen that the number of patients has increased over the years due to the increase in the number of studies. As a result of the analysis, it has been determined that the studies published in the field of VVF repair using TIFs have increased over the years. This increase makes us think that VVF repair is a topic that has received more attention in the literature over the years. It could be hoped that as studies published on this subject increase, clinically more robust data could emerge that could eventually lead to better treatment options for patients.
Another issue is related to the heterogenous nature of the fistulae and patients included. The study populations appear to be highly variable with regard to fistulae size, complexity and fistulae location. This variability affects the success rate of fistulae repair and the presence of postoperative complications.
The diagnostic methods used and definitions of surgical outcomes are also not standardized. The diagnosis of fistulae, such as history, physical examination, simple clinical tests and imaging methods used in complicated cases, may vary depending on the country, the hospital, facilities and the surgeon’s preference. There is no consensus on this. In our study, we saw that while simple diagnostic methods such as cystoscopy and IVU were preferred, complex tests were less needed. In five of the studies included in this scoping review, the diagnostic methods were not defined.16,18,26 –28 This is an indicator of methodological heterogeneity in the literature and is a parameter that hinders standardization in this regard. We hope that our study will bring these limitations of the current literature by providing a quick snapshot of the currently available clinical data and be starting point for better designed clinical studies.
Synthetic TIFs have the potential advantages of shortening the operative times, decreasing donor site morbidity and being more effective in cases where autologous tissues are not of desired quality. This review demonstrated that studies reporting on the use of synthetic TIFs are generally small/medium-sized, prospective studies without controls and they are published relatively more recently. Therefore, although available studies showed similar efficacy with synthetic flaps, currently available evidence does not allow us to draw any conclusions on their clinical safety and efficacy.
With regard to material properties of the studied synthetic TIFs, all were derivatives of the natural extracellular matrix or hemostatic agents most of which were biodegradable and absorbable. We believe absorbable soft tissue substitutes should be the preferred type of material for this particular application; however, further design requirements can be defined with a view to develop a purpose-designed synthetic TIF for this particular clinical application. This idea is mainly based on our previous work on synthetic materials used in the same anatomical site in women with urinary incontinence. The clinical experience with non-absorbable materials used in women with stress urinary incontinence (such as the polypropylene mesh) has demonstrated significant complications in a proportion of women that is mainly due to the material being a nondegradable/permanent implant.36 –38 Following on from this experience, we expressed our opinion, based on previous clinical data and expert consensus reports, on using absorbable materials in the vaginal area in females. 39 Current advances in tissue engineering and materials science could allow construction of a purpose-designed synthetic TIF. Nevertheless, well-designed clinical studies using standardized pre- and postoperative assessments and including patients with similar fistulae characteristics will be required to effectively test any new materials.
The postoperative complications that are proclaimed in included studies are variable. In eight of the studies that involve a total of 438 patients, the postoperative complications were not defined. The standardization of only three of the reported postoperative complications also supports the idea that studies in VVF repair have a low level of evidence.
When the studies included in the scoping review were examined in terms of their levels of development of the countries, the number of patients in OECD member countries was quite low compared to the number of patients in non-OECD member countries. In addition, all synthetic interposition flaps in this review were used in non-OECD member countries. The aetiology of the fistulae and treatment approaches may be different. Since treatment results may be affected, we separated these two, which may have affected the success rate. When the aetiologies of VVF cases seen in OECD member and non-OECD member countries were compared, it was seen that all of the VVF aetiologies in OECD member countries were gynaecological in origin, while VVF aetiologies in non-OECD countries were both gynaecological and obstetric in origin. When the gynaecologic and obstetric fistulas were compared by considering their success rates, it is seen that the success rate of gynaecologic fistulae was higher than the obstetric fistulae. The reported success rates of obstetric fistulae were highly variable between the studies.
Our scoping review has some limitations; the first limitation of this article is, we did not include studies with less than 10 patients to avoid further heterogeneity in results. The second one is, we could not refine our search on a more specific group of patients (e.g. post-radiotherapy patients) or more specific type of fistulae which will surely result in more heterogeneity in our findings. The third limitation is that we only included studies published in English language.
In conclusion, the current evidence comparing autologous and synthetic TIFs is not robust. Further studies on larger and more homogeneous groups with more standardized methodologies on patient assessment are required.
Supplemental Material
sj-docx-1-tau-10.1177_17562872231182217 – Supplemental material for A scoping review of tissue interposition flaps used in vesicovaginal fistulae repair
Supplemental material, sj-docx-1-tau-10.1177_17562872231182217 for A scoping review of tissue interposition flaps used in vesicovaginal fistulae repair by Halime Serinçay, Hayrullah Uğur Güler, Kezban Ulubayram and Naşide Mangır in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.