
Abstract
Single-port (SP) robotic surgery is a novel technology and is at the beginning of its adoption curve in urology. The goal of this narrative review is to provide an overview of SP-robotic partial nephrectomy (PN) 4 years after the introduction of the da Vinci SP dedicated platform, focusing on perioperative outcomes, length of stay, and surgical technique. A nonsystematic review of the literature was conducted. The research included the most updated articles that referred to SP robotic PN. Since its commercial release in 2018, several institutions have reproduced robotic PN by using the SP platform, both via a transperitoneal and a retroperitoneal approach. The published SP-robotic PN series are generally based on preliminary experiences by surgeons who had previous experience with conventional multi-arms robotic platforms. The reported outcomes are encouraging. Overall, three studies reported that SP-robotic PN cases had nonsignificantly different operative time, estimated blood loss, overall complications rate, and length of stay compared to the conventional ‘multi-arms’ robotic PN. However, in all these series, renal masses treated by SP had overall lower complexity. Moreover, two studies underlined decreased postoperative pain as a major pro of adopting the SP system. This should reduce/avoid the need for opioids after surgery. No study compared SP-robotic versus multi-arms robotic PN in cost-effectiveness. Published experience with SP-robotic PN has reported the feasibility and safety of the approach. Preliminary results are encouraging and at least noninferior with respect to those from the multi-arms series. Prospective comparative studies with long-term oncologic and functional results are awaited to draw more definitive conclusions and better establish the more appropriate indications of SP robotics in the field of PN.
Keywords
Background
The laparoscopic approach to partial nephrectomy (PN) has emerged during the last two decades showing similar perioperative, oncological, and functional outcomes to those of the traditional open approach.1,2 Laparo-endoscopic single-site surgery (LESS) was conceived more than 15 years ago as an evolution in laparoscopic surgery to potentially further reduce invasiveness.3,4 The term ‘LESS’ has been coined to incorporate a group of related techniques that perform laparoscopic surgery through a single abdominal access site, typically at the level of the umbilicus. 5 Indeed, LESS increase its popularity due to a perceived impression that reducing the number of ports would result in reduced morbidity and improved cosmesis compared to conventional multiport laparoscopy.
Since the initial report by Raman et al., 4 LESS has been used to perform various major urological procedures, including PN. Although many reports demonstrated the feasibility of LESS, this approach is even more technically demanding than the standard pure laparoscopic one. This has prevented the widespread diffusion of the technique, particularly for performing PN. 6
The advent of robotic platforms permitted to overcome some technical challenges of laparoscopy (such as limited moving space within the abdomen, lack of a wrist, and other technical difficulties) and helped to widen the indications of minimally invasive PN to more surgeons. Nowadays, the preferred approach to PN is de facto the robotic approach.7,8
Similarly to traditional laparoscopy, the robot has been used in an attempt to improve the performance with LESS, since it allows for the console left- and right-hand masters to be interchanged electronically, thus eliminating the ‘reverse handedness effect’ typical of conventional LESS. 9 Several studies on robotic LESS applied to many urological procedures including PN followed, 10 but despite some reported improvements, consistent drawbacks remained, including the external clashing and the limited accessibility for the bedside assistant. This was because the da Vinci (Intuitive, Sunnyvale, CA, USA) robotic platform was not primarily conceived for LESS purposes. 11
Similar to the history of pure LESS relative to pure laparoscopy, robotic LESS did not gain popularity. 12 In 2018, the USA Food and Drug Administration (FDA) approved the use of a ‘purpose-built’ robotic platform specifically conceived for the single-site approach. All the major urologic surgeries were duplicated by using the novel ‘da Vinci SP’ (Intuitive) robotic platform. 13 Specifically, the first single-port (SP)-robotic PN was published by Kaouk et al. 14 in November 2018. Since then, promising perioperative outcomes have been reported in the field of PN.14–22
The history of robotic single-site surgery in urology
What led us to the availability (although in the United States and Far East only at the moment) of the SP robotic platform is the hypothesis that a virtually ‘scarless’ surgery could decrease the morbidity associated with surgical access, given the lower numbers of transcutaneous points of access (i.e. the trocar sites). Such an approach could potentially translate into superior outcomes, lower complication rates, and faster recovery than the traditional multi-port surgery. 23
The idea of single-access surgery was born decades ago. 24 However, only in the early 1990s the first excision laparoscopic procedure was published in gynecology. 24 In 2007, at the 25th World Congress of Endourology, Rane et al. 25 presented the first LESS successful case in urology. Nevertheless, the genuine enthusiasm progressively decreased due to the intrinsic technical challenges associated with the use of a single access point, namely the reduced instruments’ range of motion and the unfavorable ergonomics. 26
Robotic single-site surgery: the beginning
The advent of robotic platforms renewed the interest in LESS. 14 In 2009, the Cleveland Clinic (Cleveland, OH, USA) group led by Kaouk reported the first successful series of robot-assisted single-site surgeries (including prostatectomy, pyeloplasty, and nephrectomy) performed in humans by using the multi-arms da Vinci S (Intuitive) robotic platform. 6 The authors underlined that, although the da Vinci S platform was not primarily conceived to perform single-site surgery, it facilitated the surgical dissection and the intracorporeal suturing if compared to non-robot-assisted LESS. 6 However, plenty of limitations remained, mostly relative to the clashing of robotic arms due to the instruments working in parallel (Figure 1).

Robotic single-site approach: the beginning.
Robot-assisted VeSPA single-site surgery
Intuitive Surgical Inc. then developed a novel set of instruments and accessories specifically dedicated to SP robotic surgery, named ‘VeSPA single site’, in an attempt to overcome such limitations. 27
The set included a multichannel access port with room for four cannulas and an insufflation valve: two out of four curved cannulas were for robotic instruments, and the other two straight cannulas (8.5 mm cannula for the robotic endoscope and a 5 mm for the bed-side port. Crossing the curved cannulas midway through the access port permitted the instruments to achieve triangulation of the target.
Si system software allowed to maintain the same-sided hand-eye control of the instruments. The surgeon’s right-hand controls the screen-right instrument even though the instrument was in the left robotic arm (and vice versa) (Figure 2).

The ‘VeSPA single-site’ instruments used with the Si da Vinci platform.
The Cleveland Clinic group again pioneered an early experience on the animal and the human cadaver models.28,29 The authors reported reduced external collisions among the robotic arms since the curved cannulas angled the robotic arms distant from each other.
Several clinical experiences witnessed the feasibility, safety, and efficacy of the VeSPA single-site approach for performing major urological procedures in selected patients. Particular emphasis was put on the cosmetic results.30–32
On the other hand, contrary to the ‘standard’ robotic instruments, the curved VeSPA single-site instruments did not include the EndoWrist® technology at their distal end, which made intracorporeal suturing more onerous and, again, prevented a widespread diffusion of the approach.28,29
Robot-assisted SP surgery: the advent of the purpose-built platforms
In 2014, the Cleveland Clinic and the University of Lille groups reported the first experience with a new robotic platform specifically designed to perform SP robotic surgery, namely the prototype SP999 of the da Vinci SP surgical system. 7 Prostatectomy, nephrectomy, and pyeloplasty interventions were performed on humans, with encouraging perioperative results and no conversions.
The system was designed to guarantee the surgeon the same intraoperative abilities as the existing multi-arms da Vinci platforms, except that three articulating instruments and an articulating camera were inserted into the patient through a single, multichannel port. Exclusive to this novel platform was an additional joint, the so-called elbow, which provides triangulation at the surgical site through the SP.
The SP1098 prototype was introduced as a ‘second-generation’ evolution of the SP999 that was tested within a preclinical setting only.33–37 Its components were virtually unmodified from the former model. Considering innovations, the SP1098 included a novel 25-mm multichannel port. Moreover, it has high-definition 3D optics, implementing instrument arm control, and an instrument guidance system. 11
Finally, the third-generation da Vinci SP platform included further refinements and received clearance from the USA FDA on May 31, 2018, and became available on the market (Figure 3).

The evolution of the Intuitive Inc. purpose-built da Vinci robotic platform, from the prototype SP999. (a) Used for the very first clinical experiences, through its second generation the prototype SP1098. (b) Used exclusively for pre-clinical experiences on the human cadaver model, till the USA FDA approved SP platform. (c) Nowadays available on the market.
Herein, we provide a narrative review of the ‘state of the art’ of SP-robotic PN 4 years after the introduction of the da Vinci SP platform on the market. Specific focus is given to perioperative outcomes of surgery. Finally, details of the surgical technique are provided.
Methods
A nonsystematic review of the literature within the PubMed (MEDLINE) and Ovid databases was accomplished using the keywords ‘single-port’, ‘partial nephrectomy’, and ‘nephron-sparing surgery’ (Table 1). The research included the most up-to-date articles (published since 2018 – namely, the FDA approval year of the SP platform) that were published in core clinical journals in the English language (up to 30 November 2022).
Methodology overview.

PubMed (MEDLINE) and Ovid databases were completed using the keywords ‘single-port’, ‘partial nephrectomy’, and ‘nephron-sparing surgery’, filtered for human and adult pathologic conditions.
The peer-review process was independently performed by two authors (U.C. and R.B.). Discrepancies were solved by a third party (R.C.). After a first screening based on the title and abstract, full texts of potentially eligible studies were evaluated and selected. Additional relevant articles were selected from manuscript bibliographies.
The reviewers carried out data extraction collecting the main studies’ features, including first author, year of publication, country, number of patients treated, main characteristics of patients, and perioperative outcomes.
Results were reported in the form of a narrative review. The primary aim was to evaluate the impact of SP-robotic PN on perioperative outcomes and length of hospitalization. The secondary aim of this review was to provide an overview of the SP-robotic PN techniques. Because of the absence of clinical trials (randomized and nonrandomized), weighted cumulative analysis and comparative analyses were not performed.
Evidence synthesis
The principal features of the studies included in the present literature review are summarized in Tables 2 and 3. The narrative review includes three areas of interest as discussed below.
Overview of collected studies on cadaver models and initial experience.
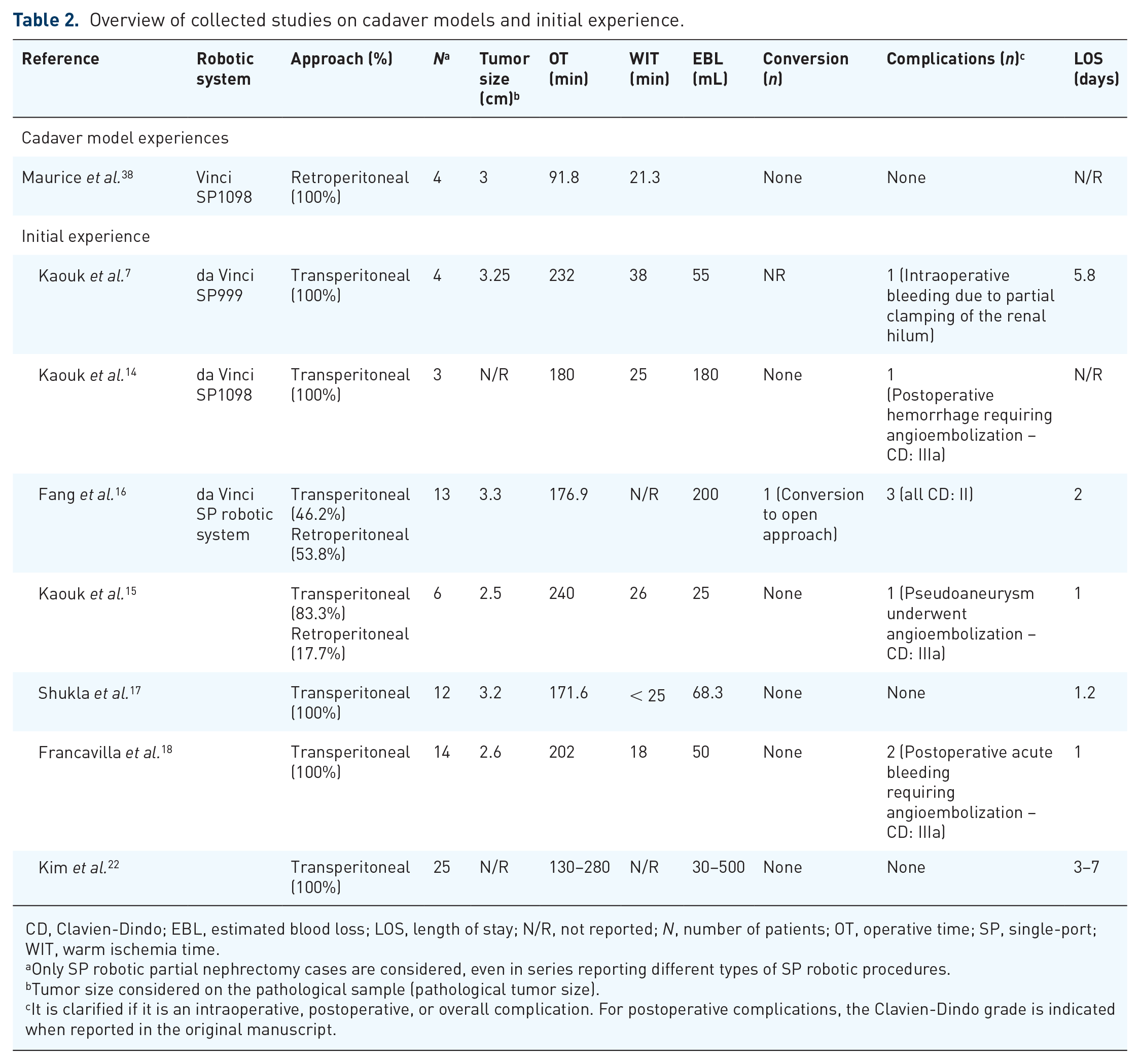
CD, Clavien-Dindo; EBL, estimated blood loss; LOS, length of stay; N/R, not reported; N, number of patients; OT, operative time; SP, single-port; WIT, warm ischemia time.
Only SP robotic partial nephrectomy cases are considered, even in series reporting different types of SP robotic procedures.
Tumor size considered on the pathological sample (pathological tumor size).
It is clarified if it is an intraoperative, postoperative, or overall complication. For postoperative complications, the Clavien-Dindo grade is indicated when reported in the original manuscript.
Collected comparative studies of single-port versus multi-port robotic partial nephrectomies.
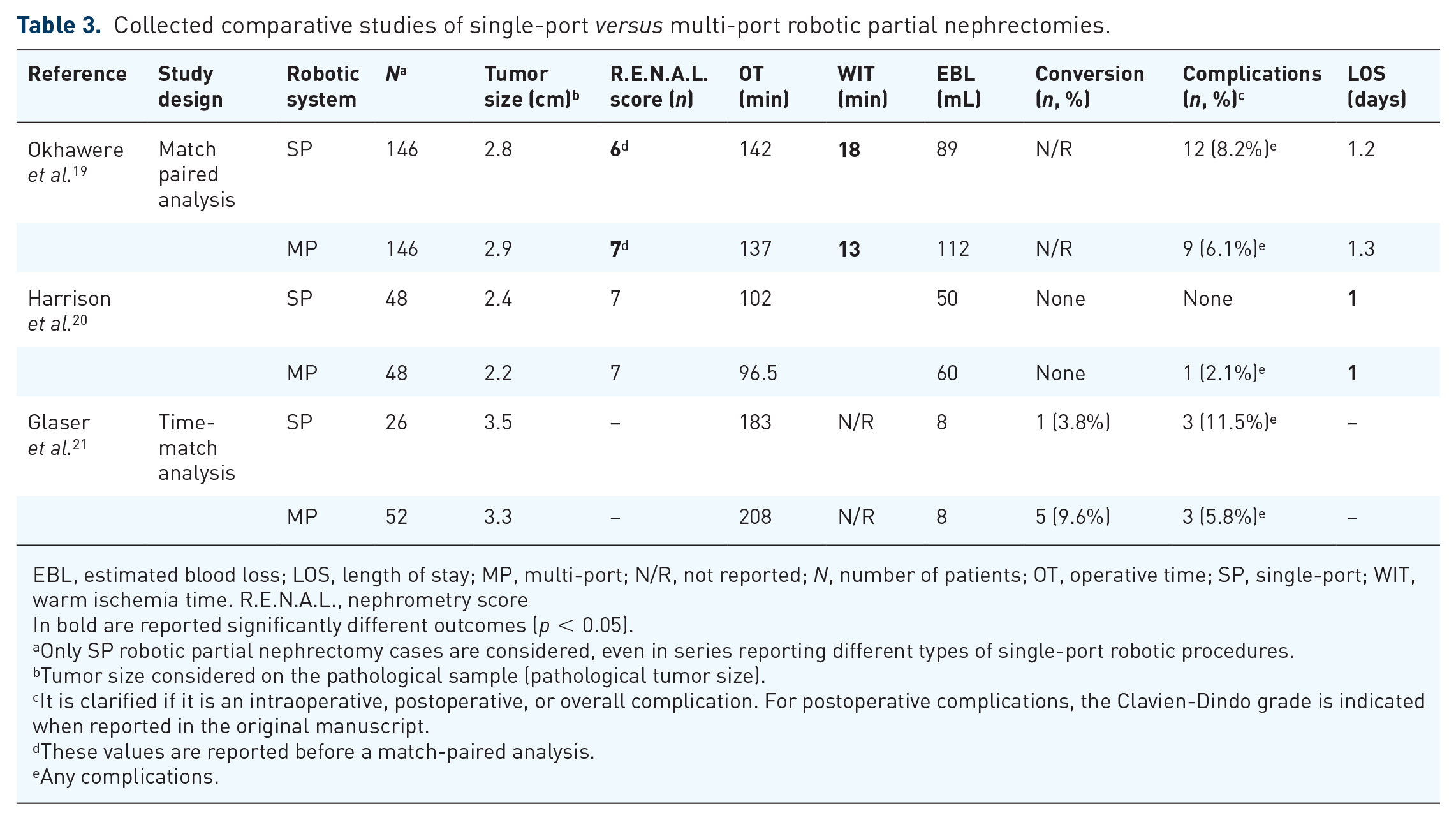
EBL, estimated blood loss; LOS, length of stay; MP, multi-port; N/R, not reported; N, number of patients; OT, operative time; SP, single-port; WIT, warm ischemia time. R.E.N.A.L., nephrometry score
In bold are reported significantly different outcomes (p < 0.05).
Only SP robotic partial nephrectomy cases are considered, even in series reporting different types of single-port robotic procedures.
Tumor size considered on the pathological sample (pathological tumor size).
It is clarified if it is an intraoperative, postoperative, or overall complication. For postoperative complications, the Clavien-Dindo grade is indicated when reported in the original manuscript.
These values are reported before a match-paired analysis.
Any complications.
Outcomes of robotic single-site partial nephrectomy before the advent of the purpose-built platforms
Within the setting of the pioneer experiences in robot-assisted single-site surgery described in Table 2, the limited range of motions, the collisions, and the challenges relative to the incorporation of the fourth robotic arm somehow ‘compromised’ the outcomes of PN. Nevertheless, several reports described shorter convalescence, less pain, and improved cosmesis.39,40
On the other hand, within a series of 51 PN cases performed for 3 cm renal masses on average, Lee et al. 41 reported a mean ischemia time of 27 min (range, 12–65 min), mean operative time >200 min, 2 conversions, and a relatively high transfusion rate (14%). On the same page, by a comparative analysis between 89 patients treated with ‘conventional’ robotic PN and 78 patients treated with robot-assisted single-site PN, Komnios et al. 42 reported a much lower rate of trifecta achievement via the robotic LESS approach (43% versus 26%, respectively).
Outcomes of SP-robotic partial nephrectomy
The feasibility of SP-robotic PN was first reported in 2017 by Maurice et al. 42 The SP1098 platform was used in the human cadaver model to perform PN approaching both the anterior and posterior surface of the kidney. All cases were completed with neither intraoperative complications nor the need for conversion.
Since the commercial release in 2018, several institutions have reproduced robotic PN by using the SP platform, both via a transperitoneal and a retroperitoneal approach.15–22 Note, the SP platform is relatively new, so published SP-robotic PN series are generally based on the preliminary experiences of surgeons with previous experience in conventional multi-arms robotic platforms.15–22
Interestingly, a number of authors agreed that a learning curve for SP cases does exist, even for surgeons who have an extensive experience with multi-arms platforms. This is mostly associated with the ability to use the new articulating SP camera. The instruments of the SP system provide similar degrees of freedom of standard multi-arms da Vinci platforms, with some differences in intracorporeal suturing (typical of PN). It has been reported that the loss of the EndoWrist technology could mostly affect expert robotic surgeons (with a consistent number of procedures performed using the earlier multi-arms da Vinci platforms). 43
Finally, the SP platform requires accurate coordination between the instruments’ and the camera’s movements to compensate for the smaller working area and the narrower visual field. 18 It is interesting to underline that expert robotic surgeons reported cases of postoperative acute bleeding (3 cases considering all included studies – Table 2), managed with angioembolization. This is probably relative to the different feelings and tension forces applied during suturing. Such a complication is generally rare within the robotic PN series, especially among expert robotic surgeons.14,15,18 At the moment, the literature is unable to suggest a minimum number of procedures to perform before surgeons can feel confident with the technology. Undoubtedly, patient selection is key.
In the setting of a match-paired analysis of 146 SP versus 146 standard robotic PN by the ‘Single Port Advanced Robotics Consortium’ (SPARC), Okhawere et al. 19 showed that the majority of the SP-robotic PN cases treated (52%) presented with a low tumor complexity. Such lower complexity masses can be more appropriate to start with the SP learning curve. Before marching, the SP group had a lower mean tumor size (2.93 versus 3.42 cm, p = 0.0001) and a significantly lower median R.E.N.A.L. score (6 versus 7, p < 0.001). Matching balanced for these differences, with both groups having similar mean tumor size (2.9 cm) and median RENAL nephrometry score of 6. Regarding perioperative outcomes, SP and conventional robotic PN groups had nonsignificantly different operative times, estimated blood loss, overall complications rate (8 versus 6%, p = 0.2), and length of stay. Notably, when stratifying by tumor complexity, the operative time of SP-robotic PN procedures for high-complexity renal masses was shorter (108 versus 167 min, p < 0.05). Finally, notwithstanding the overall low complexity of the renal masses included in the study, SP-robotic PN had a longer mean ischemia time (18.3 versus 13.8 min; p < 0.001). In summary, although the differences in the port configurations and the surgical technique/approach used typically of a multicentric design represented a limitation of the analysis, the SPARC analysis showed that SP-robotic PN is a safe procedure in the hands of expert robotic surgeons. 19
Similarly, Harrison et al. 20 compared the perioperative and short-term functional and oncological outcomes of SP-robotic versus multi-arms robotic PN by a propensity-score analysis. Before matching, the cohort included 48 and 238 patients who underwent SP and multi-arms procedures, respectively. This study overstressed the concept that one major strong point of the SP system was decreased postoperative pain, which theoretically avoids (or at least decreases) the need for opioids after surgery. 20 While there was only a subtle difference in terms of median length of stay (1.4 versus 1.6 days, p = 0.004), following 1:1 propensity-score matching, the SP cohort had lower opioids use both on postoperative day 1 (4.6 versus 9.8 morphine milligram equivalents [MME], p = 0.02) and cumulative during the in-hospital stay (5.1 versus 9.3 MME, p = 0.03).
Conversely, other groups published different experiences reporting a similar length of stay (the vast majority of patients were discharged on postoperative day 1) and without any differences in the MME administered either during the hospitalization or in the outpatient setting. 21 The reader will argue that such differences are ‘relevant’ from a statistical point of view rather than from a clinical one.20,21 Another explanation for the lack of relevant differences between SP and conventional multi-arms robotic PN is that a number of centers worldwide already use a same-day/overnight discharge pattern after robotic PN. Thus, even if SP-robotic can decrease the number of skin incisions and the relative pain associated, we can conclude that robotic PN has achieved a high standard whatever the platform used. 44
Focus on length of stay after SP-robotic PN
It is a common feeling in the literature that a potential benefit of SP-robotics is the chance to more likely consider a same-day discharge pattern after surgery. Promising results have been reported by various single-center studies both on PN and other surgical interventions.45,46 Abaza et al. 45 assessed the impact of the adoption of the SP-dedicated platform on the length of stay after their initial 100 SP procedures (performed between 2019 and 2020). Their series was also compared to a cohort of ‘conventional’ robotic PN cases.
Note, Abaza et al. 45 routinely offer same-day/overnight discharge after robotic procedures performed at their Institution since 2016, which means they have consolidated an outpatient pathway even before the advent of the SP platform. The SP group evaluated included 59 prostatectomies, 18 PNs, and other procedures. Interestingly, the rate of same-day discharge in the SP group was higher compared to multi-arms surgeries, despite the authors declaring they equally offer this discharge pattern to all patients (88% versus 51%, p < 0.0001). Specifically, among PN patients, 83% of SP patients went home the same day of surgery versus 17% of multi-arms cases (p < 0.001).
On the other hand, we remark that other series analyzed such discharge patterns after urological robotic procedures underlying that the same-day discharge is feasible even when using the multi-arms robotic platforms. 44
In the setting of a bi-centric USA experience that reported the outcomes of robotic PN cases performed between 2010 and 2019 by using multi-arms robotic platforms, 173 (60.5%) patients who were discharged on the first postoperative day had lower BMI (29 versus 32, p = 0.02), were more likely treated via a retroperitoneal approach (13 versus 9%, p < 0.001), and had lower rates of overall (3.6 versus 30.5%, p < 0.001) and major (Clavien-Dindo grade ⩾ III) postoperative complications (1.8 versus 6.1%, p < 0.001). Logistic regression analysis found operative time and the occurrence of a postoperative complication as independent predictors of prolonged hospital stay.
A concept always stressed at congresses and meetings by Jihad Kaouk, the first adopter of the SP platform, is that the purpose-built SP robot allows for ‘regionalizing the surgery to the location of the disease’, leading to a ‘minimal impact surgery’ Simone Crivellaro says. For example, it is interesting to note how surgeons performing SP-robotic PN are more likely to choose a retroperitoneal approach, which in many series has been associated with a shorter length of stay.19,20,47 This finding is likely due to one of the key features of the SP robot, which is well suited to work within narrow spaces such as the retroperitoneum, facilitates access and docking, and reduces the need for dissecting several anatomical structures before performing the resection of the renal mass. 48
Hospital stay and cost-effectiveness
To date, no study compared SP-robotic versus multi-arms robotic PN in cost-effectiveness. The restriction in terms of financial resources of the health systems brings an honest and deep reflection on the costs. It can be considered a priority and should be a crucial component of the approval process for any medical innovation/technology, especially in surgery. Innovations in surgery often require the use of expensive equipment which required a careful demonstration of their feasibility, safety, and health benefits, as well as cost-effectiveness. Likewise, the use of the da Vinci SP as a dedicated surgical instrument for PN cases will have to be assessed and compared financially to the standard of care.
SP robotic partial nephrectomy: technical details and main differences with the multi-port robotic system
The SP system presents a number of intrinsic key differences compared to the multi-arms platforms that necessarily lead to some modifications in the PN technique.11,19,43
The fully wristed camera and its ‘cobra’ mode, together with the possibility of an en-bloc rotation of all the instruments, allow for the optimal vision of the target anatomy and are unique to the SP platform. As we already mentioned before, the instruments of the SP surgical system allow degrees of freedom comparable to those of the standard multiport da Vinci platforms, but differences can be perceived, particularly during the renorrhaphy phase of PN, because of the novel elbow, so that the dynamics of suturing is modified. Moreover, the reader should keep in mind that the SP platform lacks the EndoWrist technology.
From a technical point of view, by utilizing the ‘Hasson technique’, a 2- to 2.5-cm fascial opening is performed to place the cannula with a blunt obturator directly through it. Otherwise, it can be practiced a slight extension of the incision with the aim of accommodating adjacent additional ports and instruments. Moreover, a gel cap such as the GelPORT (Applied Medical, Rancho Santa Margarita, CA) can also be used (Figure 4(a) and (b)).

(a, b) The dedicated SP multichannel cannula and an assistant port are introduced through the same incision via a wound protector GelPORT. (c) Sketch of the concept of ‘floating docking’ aimed to increase the working distance needed from the port site and the target anatomy.
For a transperitoneal approach, allocating the port on the umbilicus may provide a muscle-sparing incision. It can also be further extended to extract the specimen. The whole instruments and the robotic camera are put in place through the multichannel SP port. Interestingly, the latest SP system requires a 10-cm working distance between the port site and the target anatomy. 19 With shorter distances, there will not be an unfold of the robotic instruments and the full range of motion. It is common when patients have thin body habitus as well as large masses at the lower pole approached retroperitoneally. Two solutions are generally used to manage this aspect: the first one is to allocate the ports far away from the target anatomy (which is not always possible in the case of large masses approached via a retroperitoneal route); the second one is the so-called floating docking technique, which consists in moving the seal of the wound protector system, through which the trocars are placed, further from the skin level (Figure 4(c)).19,49
Concerning the assistant port, this can be allocated just adjacent to the SP cannula but is ‘handcuffed’ to it having restricted maneuverability. 19
Limitations in suction should be overcome using a flexible suction catheter managed by the operator, like the ‘Remotely Operated Suction Irrigation System’ (ROSI, VTI, Nashua, NHI), which is normally allocated through the adjacent assistant port through the same cut or the fourth channel of the SP cannula if the fourth arm instruments are not used.
At present, the SP instruments’ armamentarium is restricted in its scope with respect to that of the multi-arms X and Xi platform.50,51 For instance, the ProGrasp™ forceps are not currently available, as well as cutting-edge energy devices like the Vessel-sealer and large clip applier. Furthermore, near-infrared fluorescence is not on the market yet.
Another limitiation is due to the fact that most of the series published about SP robotic procedures (including SP -robotic PN) had been affected by the recent COVID-19 pandemic that could have limitated the diffusion and utilization of the SP robotic platform. However, a number of centers had used some strategies to minimize the impact of the worldwide pandemic. 52
Conclusion
The SP-robotic approach to PN appears to be feasible and safe. The preliminary reports about perioperative outcomes are encouraging and at least noninferior to those from the multi-arms series. We believe that the continued use of the platform is justified in centers where the technology is available. Well-designed comparative studies with long-term oncologic and functional results will be necessary to draw more definitive conclusions and better establish the future role and appropriate indications of the SP platform.