
Abstract
Introduction:
One of the most challenging aspects of inflatable penile prosthesis (IPP) surgery is reservoir placement. The traditional space of Retzius (SOR) is not suitable for all patients. For example, radical cystectomy or prostatectomy may alter the anatomical SOR. Hence, traditional placement of the reservoir in this space increases the risk of bowel or vascular injury. Also, patients with bilateral inguinal hernias repaired with mesh, or those with previous reservoirs that have been retained, are not eligible for a Retzius reservoir. Our study reports on the use of midline sub-rectus muscle placement of a penile prosthesis reservoir in these patients as an alternative to high submuscular placement commonly used.
Methods:
A retrospective chart review of male patients who underwent IPP surgery between June 2017 and 2021 was conducted. Patients were divided into two groups based on the location of the reservoir: SOR versus Midline Submuscular Reservoir (MSMR). Complication rates were compared, including herniated reservoirs, infections, bowel injuries, and vascular injuries.
Results:
Our cohort included 461 patients who underwent IPP surgery between June 2017 and 2021 in one tertiary center. SOR was used in 89% of patients and MSMR in 11% of patients (n = 413 and 48, respectively). Median follow-up for all patients was 28 months. The mean age was 67 ± 8 years. There was no statistically significant difference between the two groups regarding age or comorbidities (BMI, diabetes mellitus, hypertension, hyperlipidemia, and coronary artery disease). The complication rate was low in both the SOR and MSMR groups, with device malfunction being the most common (2% versus 4%, respectively; p = 0.32). The infection rate was 0.5% in the SOR group with no infections in the MSMR group (NS). There was only one case of herniation requiring surgical revision in the SOR group and no cases of bowel or vascular injury.
Conclusion:
Placement of a penile prosthesis reservoir within a midline rectus submuscular space is a safe and effective technique when the SOR is compromised by previous surgery or bilateral inguinal canals are not accessible.
Introduction
Worldwide, erectile dysfunction (ED) is on the rise, as is the number of penile prostheses implanted.1,2 Inflatable penile prosthesis (IPP) is considered the gold standard treatment for patients with ED who had a lack of response to medical treatments.
The most common reservoir placement for a three-piece IPP is in the space of Retzius (SOR), which is accessed via an extraperitoneal approach through the external inguinal ring and piercing the transversalis fascia. 3 While this is an ideal location in a virgin IPP case, the SOR is often compromised or obliterated in patients with prior abdominal/pelvic surgery such as radical prostatectomy. Prior inguinal hernia repair also makes accessing this space challenging. Furthermore, there have been reported complications of SOR placement, specifically bladder, vascular, or bowel injuries; reservoir herniation; or migration and dislocation of reservoir.4–6
A multitude of techniques have been described to circumvent the challenges of accessing the SOR in men with prior surgery. These ectopic reservoir locations include intra-abdominal, high submuscular, subcutaneous, and even within the retroperitoneum.7–10 While these alternative locations are useful in the setting of hostile retropubic anatomy, they are not devoid of their own risks, with the most reported adverse events being palpable reservoir, device herniation, and reservoir leak.11,12
We describe our technique of midline submuscular reservoir (MSMR) placement in men with a hostile pelvis after radical prostatectomy or cystectomy, and for patients with bilateral inaccessible external inguinal rings. In addition, we report the safety and efficacy outcomes in 48 men who underwent MSMR reservoir placement.
Materials and methods
A retrospective chart review of male patients who underwent IPP surgery for treatment of erectile dysfunction between June 2017 and June 2021 was conducted. Institutional Review Board approval was given by the Mount Sinai Health System Institutional Review Board (STUDY-20-01505) with a waiver of informed consent. All surgeries were performed by a single high-volume surgeon at a tertiary care center in New York City. Inclusion criteria were patients aged 18 years or older undergoing IPP surgery with a minimum 6-month follow-up. Patients were divided into two groups based on the location of the reservoir: SOR versus MSMR. Complication rates were compared, including herniated reservoirs, infections, bowel injuries, and vascular injuries. Case characteristics were summarized using means and percentages. Fisher’s exact tests were used to compare categorical variables. A multivariable logistic regression model was used to analyze the association between reservoir location and complication rate while controlling for case characteristics screened through univariable analysis. Statistical analysis was performed using Stata 16 (StataCorp, College Station, TX). Tests with a p value <0.05 were considered statistically significant.
Midline submuscular technique
For the procedure, patients signed a written consent form. Our technique for penile prosthesis follows a standard vertical scrotal incision with assistance of a Wilson retractor (Figure 1). Prosthesis cylinders and pump are placed first. Once it is time for reservoir placement, an index finger is used to palpate the pubic tubercle via the scrotal incision. This can be performed on either the patient’s right or left side of the phallus. After identification of the pubic tubercle, dissection is carried cephalad to the level of the rectus fascia. A retractor can be used to mobilize Scarpa’s fascia and the overlying fat while exposing the rectus fascia. The fascia is then entered sharply using a tonsil clamp at 4 cm above the pubis and lateral to the linea alba. Using the index finger, blunt separation of the rectus muscle (RM) is carried out to the level of the posterior sheath of the rectus. Thus, a submuscular space is created between the RM and posterior sheath of the RM. Care is taken not to violate the posterior sheath to avoid entering the SOR or peritoneal cavity. Further dissection of the layers of RM is preformed while the underlying transversalis fascia is palpated. An S retractor is now placed in the sub-rectus space and the reservoir is placed using a ring clamp. The reservoir is placed in the midline, between the RM and the posterior sheath of the RM (Figure 2). The RM prevents herniation of the reservoir. The small defect on the rectus fascia does not require closure. As the reservoir is embedded within the muscle, it is less likely to herniate or become palpable to the patient (Figure 3). After placement of all IPP components and cycling of device, a Jackson-Pratt drain is placed in the scrotum, just overlying the tubing. Layers of Dartos are closed in running locking fashion using 3-0 chromic, with care being taken to not accidentally violate the tubing or any device components. Scrotal skin is closed with 3-0 chromic in a vertical mattress fashion. The device is inflated and a mummy wrap dressing applied using Kling. Patients are then seen 2 days postoperatively for drain and dressing removal with wound check. A follow-up visit is performed at 6 weeks for device cycling teaching, as needed, and periodically thereafter.

Standard vertical scrotal incision with assistance of a Wilson retractor.

Inflatable penile prosthesis reservoir in the midline submuscular space with its anatomical boundaries.

An abdominal CT image of a 68-year-old patient who underwent IPP surgery. Reservoir in the submuscular space.
Results
Our cohort included 461 patients who underwent IPP surgery between June 2017 and June 2021 in one tertiary center by a single high-volume surgeon. SOR was used in 89% of patients and MSMR in 11% of patients (n = 413 and 48, respectively). Median follow-up for all patients was 28 months. The mean age was 67 ± 8 years. There was no statistically significant difference between the two groups regarding age or comorbidities [body mass index (BMI), diabetes mellitus, hypertension, hyperlipidemia, and coronary artery disease] (Table 1). Most MSMR cases were involving patients with inaccessibility of the inguinal rings (68.7%), and bilateral hernia surgery was the most common condition affecting reservoir location (41.6%; Table 2). The average IPP cylinder size was 21.1 cm and 21.2 cm in the SOR and SMSR groups, respectively (p = 0.93). The complication rate was low in both groups, with device malfunction being the most common (2% versus 4% respectively; p = 0.32). The infection rate was 0.5% in the SOR group with no infections in the MSMR group (NS; Table 3). There was only one case of herniation in the SOR group and no cases of bowel or vascular injury in either group. The ectopic location of the reservoir was not associated with an increased risk of complications in univariable or multivariable analysis.
Patient demographics and comorbidities.

BMI, body mass index.
Indications for placement of MSMR.
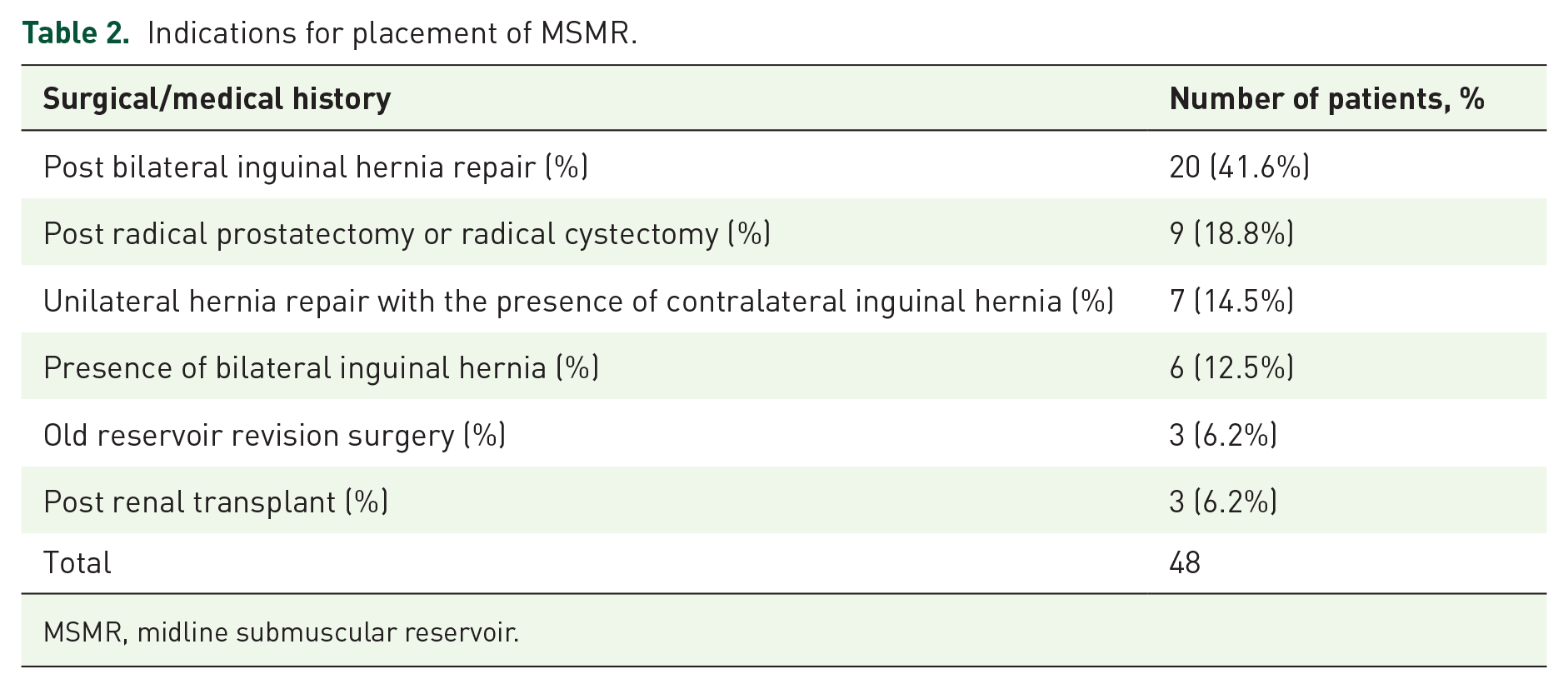
MSMR, midline submuscular reservoir.
Inflatable penile prosthesis reservoir location and complication rates.

Discussion
The literature has numerous examples of ectopic reservoir placements including: intra-abdominal, high submuscular, subcutaneous, and retroperitoneal. Despite diminished rates of bladder, bowel, and vascular injuries, surgical revisions due to a painful/palpable reservoir and reservoir herniation were still observed.11–13
Our technique of submuscular rectus reservoir placement is another tool in the armamentarium of the prosthetic urologist. It obviates the need for entering the inguinal canal and placing a high submuscular reservoir, especially in men who have inaccessible bilateral inguinal rings. When correctly placed, the reservoir sits in the middle of the rectus muscle bellies, thereby avoiding both intraperitoneal and extraperitoneal locations, which may otherwise be compromised by prior surgeries. In thin patients who may require submuscular reservoir placement, oftentimes the reservoir is visible at the level of the skin. With this approach, the reservoir is not visible, regardless of the body habitus.
Our MSMR group had neither pelvic organ injury (bladder, bowel, or vascular) nor surgical revision due to reservoir herniation or pain. We did have two cases of revision due to device malfunction (4%).
Few ectopic reservoir placement techniques still rely on the accessibility of the inguinal ring. A publication by Garber et al. described their experience with sub-external oblique reservoir placement. Briefly, the external ring is accessed, and blunt dissection just superficial to the spermatic cord and through the inguinal canal is performed. A Deaver retractor is used to raise the undersurface of the external oblique fascia, and a Foerster clamp is then used to place the reservoir high into the canal, with the lock-out valve above the spermatic cord. 14 With our technique, there is no need to access the inguinal ring.
A recent publication presented a novel technique of accessing the SOR without need for accessing the external inguinal ring, however. Mykoniatis et al. described a technique of reservoir placement through the external oblique muscle fascia to gain access into the SOR. This is an easily reproducible technique as the fascia can be visualized medially by lateral retraction of the spermatic cord and punctured with Metzenbaum scissors. 15 This technique depends on access to the SOR which might be violated in patients after radical prostatectomy or cystectomy.
Grimberg et al. retrospectively examined an IPP database of 534 patients, comparing 51 (9.6%) patients who underwent counter-incision (CI) reservoir implantation with non-CI reservoir implantation. Despite similar complication rates between CI and non-CI cohorts, the CI cohort had significantly more removals and replacements. 16
If the need to remove the reservoir arises in the future, a second incision would not be necessary with MSMR placement. The reservoir would be readily accessible. In addition, it provides excellent cosmesis and patient comfort.
The size of the IPP reservoir depends on the size of the cylinders. 17 The average IPP cylinder size was 21.1 and 21.2 cm in the SOR and MSMR groups, respectively (p = 0.93). We use a 125-mL reservoir and fill it between 90 and 110 mL according to the prosthesis size. We assume that post-operative pain and reservoir bulging are less likely to be affected by similar reservoir fluid amounts across groups.
In selection of the ideal reservoir placement, patient body habitus, history of prior pelvic or groin surgery, and individual anatomy must be considered. Thus, the prosthetic urologist must be very facile in his or her ability to modify reservoir placement to account for the aforementioned factors. Of course, if a technique is easily reproducible, it allows for greater adoption within the surgical community. Unlike some of the other touted ectopic reservoir placements, our midline submuscular rectus space does not rely on the vagaries of blind dissection on flimsy fascial layers that are often difficult to identify with blunt palpation. Rather, it is contingent upon sound anatomic landmarks such as bone and muscle. Because we do not violate these fascial layers or enter the inguinal canal, the theoretical risk of hernia formation is practically nonexistent. 18 Because the reservoir is buttressed on either side by the substantial muscle bellies of the rectus, patient device palpation, erosion, and migration are also unlikely.
Limitations of our study include its retrospective design. However, given that it is a description of technique, we feel that the merits and utility of this technique outperform the study design. To support our findings, a large cohort prospective study is needed in the future. One of the theoretical drawbacks of this technique is potential injury of inferior epigastric vessels, which pierce the transversalis fascia, and passing in front of the arcuate line, ascend between the rectus abdominis muscle and the posterior sheath. In our experience, we have not had a single epigastric vessel injury or other hematoma formation using our submuscular rectus reservoir.
Conclusion
In men with inaccessible bilateral inguinal rings, reservoir placement in a submuscular rectus space is an easily reproducible and safe alternative at the time of inflatable penile prosthesis placement.
Supplemental Material
sj-doc-1-tau-10.1177_17562872221139109 – Supplemental material for Midline submuscular penile prosthesis reservoir placement for patients with bilateral inaccessible inguinal rings: technique and outcomes
Supplemental material, sj-doc-1-tau-10.1177_17562872221139109 for Midline submuscular penile prosthesis reservoir placement for patients with bilateral inaccessible inguinal rings: technique and outcomes by Ariel Zisman, Shirin Razdan, Alexandra Siegal, Michaela Sljivich, Christine Bieber, Patrick Ho and Robert Valenzuela in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.