
Abstract
Introduction:
We carried out systematic review and network meta-analysis to investigate the role of stem cell therapy (SCT) in the management of erectile dysfunction (ED) secondary to cavernous nerve injury in rats and post-radical prostatectomy (RP) in humans.
Patients and Methods:
The protocol was registered with PROSPERO database. We searched studies analyzing the efficacy of SCT for ED due to bilateral cavernous nerve injury (BCNI) in rats using Healthcare Databases Advanced Search (HDAS) Export software (MEDLINE, EMBASE, Scopus) from inception to September 2020. The outcome measurements, for 29 animal studies, were intracavernosal pressure (ICP), ICP/MAP (mean arterial pressure) ratio, and histological/molecular changes. All three available human trials evaluating SCT in post-RP ED were assessed for International Index for Erectile Function (IIEF) Score and Erection Hardness Score (EHS).
Results:
For ICP measurement, animal studies were divided into adipose-derived stem cells (ADSCs) subgroup and bone marrow–derived stem cells (BMSCs) subgroup. Pooled analysis of these studies showed a beneficial effect of SCT in improving erectile function in rats with BCNI using network meta-analysis (95% confidence interval, CI; p < 0.001). There was an increase in ICP/MAP ratio in stem cell groups (including co-intervention) compared with control BCNI group. Histological and molecular evaluation of penile tissue revealed an increase in neuronal nitric oxide synthase (nNOS), smooth muscle content, and anti-apoptotic activity. Human trials revealed improved IIEF (70–150% from baseline at 6 months) and EHS (80–200% from baseline).
Conclusion:
Our results confirm that SCT does improve the erectile function in rats having cavernous nerve injury. Similarly, early human results have shown promising results.
PROSPERO registration ID:
CRD42020201343.
Introduction
Prostate cancer (PCa) is the second most frequent cancer diagnosis made in men and the fifth leading cause of death worldwide. 1 Radical prostatectomy (RP) remains the most commonly employed procedure for localized PCa in patients with a life expectancy of at least 10 years, which represents 25% of patients with PCa.1,2 Erectile dysfunction (ED) is a common complication after RP. 3 It is estimated that 86% patients experience ED after RP.4,5 Several factors determine the development of ED after RP. The important ones include patient age, preoperative potency status (baseline Erectile function), comorbidities, performance of nerve-sparing RP (unilateral versus bilateral), type of surgery (intra- versus inter- versus extra-fascial), surgical technique (open versus laparoscopic versus robot-assisted RP), and level of surgical experience.4,6 It was thought that robotic techniques will reduce ED in RP, but a recent meta-analysis has not been able to establish the same. 7
Post-RP ED substantially decreases quality of life (QoL) of the afflicted men and their sexual partners. 8 The main stay of treatment is phosphodiesterase type-5 inhibitors (PDE5Is) with other strategies being intraurethral alprostadil, intracorporal injection therapy, vacuum erection devices, and surgical procedures like penile revascularization and penile prosthesis implantation. 9 It is important to mention that majority of these strategies treat ED symptomatically and do not address the underlying cause of ED. Furthermore, limitations to their use exist, such as intolerance to side effects, cost limitations, and unsatisfactory outcomes. 10 Newer modalities [such as stem cell therapy (SCT) and low intensity extracorporeal shock wave therapy (LI-SWT)] are being investigated to develop a curative treatment for post-RP ED with the aim to restore cavernous nerves and rehabilitate penile erectile tissue.10,11 Stem cells are hypothesized to address both of these goals and as such being looked into their potential role in curative management of post-RP ED.
SCTs have been used in various clinical conditions due to immunoregulatory, immunosuppressive, and regenerative properties. In recent years, it has been established that within penile tissue, stem cells can differentiate into endothelial, neuronal, or smooth muscle cells and are capable of restoring possible structural damage in the penile tissue. Based on these very properties, several animal and human trials have been performed to evaluate the role of mesenchymal stem cells (MSCs) in the treatment of post-RP ED. In ED research, three types of stem cells are commonly used, including adipose-derived stem cells (ADSCs), bone marrow–derived stem cells (BMSCs), and muscle-derived stem cells (MDSCs). 12
In this meta-analysis, an attempt has been made to summarize and analyze animal studies having SCT for ED due to cavernous nerve injury with outcome measurements being intracavernosal pressure (ICP), ICP/MAP (mean arterial pressure) ratio, and histological as well as molecular changes in penile tissue. All three available human trials evaluating SCT in post-RP ED were assessed for International Index for Erectile Function (IIEF) and Erection Hardness Score (EHS).
Methods
The study protocol was registered with PROSPERO (CRD42020201343).
Evidence acquisition
Criteria for considering studies for this review
The inclusion criteria for animal studies included the following:
Animals/population: Male rats, ED secondary to cavernous nerve injury
Intervention/exposure: SCT
Comparator/control: Sham versus bilateral cavernous nerve injury (BCNI)/vehicle/stem cell/co-intervention/combined
The inclusion criteria for human studies included the following:
Animals/population: Male patients, ED secondary to RP
Intervention/exposure: SCT
The exclusion criteria for animal studies included the following:
Animals/population: Use of stem cells in male rats in which ED was due to other causes like metabolic/neurological.
Intervention/exposure: If the interventions are ill defined or dose/frequency is not mentioned or/ structural methods are inadequate.
Comparator/control: Studies which lacked proper grouping into control, Sham, and intervention.
Study design: Studies which did not fulfill above criterion and lacked any defined outcomes.
The exclusion criteria for human trials included studies using stem cells in male patients having ED due to non-prostatectomy causes.
Outcome measures
Animal studies
Primary outcomes:
ICP measurements
ICP/MAP ratio
Secondary outcomes: (histological/molecular)
Increase in nitric oxide synthase (NOS) fibers
Increase in smooth muscle content
Miscellaneous immune response–related changes
Human studies
IIEF score
EHS
Change in penile length
Adverse effects
Search method for the identification of studies
Electronic searches
The systematic review was done in accordance with Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA). The search was limited to the English language. Healthcare Databases Advanced Search (HDAS) Export software was used for searching MEDLINE, EMBASE, and also searched other databases (inception to September 2020). Search terms included ‘Prostatectomy’, ‘Erectile dysfunction’, ‘Stem cells’, ‘Rats’, ‘Animal experiments’, and ‘Human trials’. Boolean operators (‘And’/‘Or’) were used.
Data extraction
Two reviewers (M.M.W., S.M.) independently screened all abstracts and full-text articles for eligibility according to the criteria for considering studies for this review. Any disagreements were resolved by mutual consensus. Two authors (M.M.W., S.M.) extracted data from individual studies.
For animal studies, the data were grouped into data sheets having columns for type/source of stem cells, any co-intervention, total rats, randomization of rats, mode of cavernosal nerve injury (crush/electric/cryo), route (intracavernosal, intravenous, local) and dose of stem cells (most common dose used is 1.0 × 106 cells), and assessment interval (variable, most studies have performed at 4 weeks post-intervention) (Table 1).
Animal study: data extraction results.

adMSC, adipose MSC; ADSC, adipose-derived stem cell; AUC, Area under curve; BCNI, bilateral cavernous nerve injury; BDNF, brain-derived neurotrophic factor; BM-MSCs, bone marrow–derived stem cells; CC, corpus cavernosum; CCK8,Cell Counting Kit-8; cGMP, cyclic guanosine monophosphate; d-MSCs, differentiated MSCs; ED, erectile dysfunction; bFGF, Basic fibroblast growth factor; eNOS, endothelial nitric oxide synthase; GDNF, glial cell-derived nerve growth factor; GFP, green fluorescent protein; hBDNF, human brain–derived neurotrophic factor; hBMSC,human bone marrow stem cells;HBSS, Hanks Balanced Salt solution; hUCB, human umbilical cord blood; ICA II, Icariside II; ICI, intracavernosal injection; ICP, intracavernosal pressure; iMSC, induced pluripotent stem cell–derived MSC; MAP, mean arterial pressure; MD-MSC, Muscle derived stem cells; MPG, major pelvic ganglion; MRI, magnetic resonance imaging; MSC, mesenchymal stem cell; NA, not available; NAS, neural-like cells from adipose-derived stem cells; NES, neural stem cells; NGF-hydrogel, nerve growth factor–incorporated hyaluronic acid–based hydrogel; nNOS, neuronal nitric oxide synthase; NOS, nitric oxide synthase; PBS, phosphate-buffered saline; PKH-26, red-fluorescent dye; PPI, periprostatic implantation; qRT-PCR, quantitative reverse transcription polymerase chain reaction; rAd, recombinant adenoviruses; SCs, Schwann cells; SD, Sprague-Dawley rats; SPC, smooth muscle progenitor; SPION-MSC, super-paramagnetic iron oxide nanoparticle labeling was performed for MSC; SVF, stromal vascular fraction; SWT, shock wave therapy; TUNEL, terminal deoxynucleotidyltransferase-mediated nick-end labeling; VEGF, vascular endothelial growth factor.
For three human trials using SCT for post-RP, the data were categorized into total patients, age in years, duration since procedure, cell type used (adipose versus bone marrow), dose (most common dose being 1 × 109 cells), mode of delivery (intracavernosal, intravenous, local), side effects, mode of assessment (using standard tools like IIEF), and follow-up (Table 2).
Human study: data extraction results (post-radical prostatectomy).

ADRC, adipose-derived regenerating cell; BM-MNCs, bone marrow mononuclear cells; EHS, Erection Hardness Score; IIEF, International Index for Erectile Function.
Quality assessment. SYRCLE’s RoB tool (Systematic Review Centre for Laboratory Animal Experimentation) which is an adapted version of the Cochrane RoB tool was used for animal studies (Figure 1). 45 All three human trials were evaluated in this study; no quality assessment was performed for them
Statistical analysis
Traditional meta-analysis was performed where possible. As all studies were unlikely to evaluate all treatments, a second set of analyses used a network meta-analysis approach to make indirect, as well as direct, comparisons between studies. A frequentist approach was utilized. 46 Specifically, the general approach used a model for treatment contrasts (the ‘contrast-based’), which considers treatment effects as fixed effects, and heterogeneity between studies as random effects. 47 All analyses were performed using the DerSimonian-Laird random-effects method, regardless of the amount of heterogeneity between studies. Statistical heterogeneity was assessed using the I2 statistics. Substantial statistical heterogeneity was assumed if the I2 value was above 50%.

SYRCLE for animal studies.
An inverse variance method was used for continuous data and expressed as the mean difference with 95% confidence interval (CI), and for dichotomous data, a Mantel-Haenszel method was used. A p value of <0.05 was considered significant. The preferred method of variation was the standard deviation. Where this was not available, the value was imputed. The standard deviation was assumed to be a quarter of the data range.
The studies were divided into one of three subgroups depending on the source of adult stem cells: ADSC, BMSC, and Mixed. Meta-analyses were performed for the ADSC and BMSC subtypes, but due to a small number of studies (only two), no analysis of the mixed subgroup of studies was performed.
Results
Description of studies
Literature search
Animal studies
In total, 189 articles matched initial search. After removing duplicates, 71 were screened, of which further 37 were excluded (conference abstracts, language other than English, abstract-only studies). Furthermore, SQR3 (Survey, Question, Read, Recite, and Review) technique was used and 34 articles were found relevant; however, 5 articles were excluded (nerve injury by radiation, studies involving oral therapy or use of cells other than stem cells, studies evaluating role in apoptosis); 29 studies were included for qualitative and 22 studies in quantitative analysis (Table 1). PRISMA flowchart is attached.
Human studies
Five articles matched initial search. After screening, two articles were excluded and three were included in qualitative research. PRISMA flowchart is attached.
Included studies
Animal studies
In 29 animal studies, a similar experimental protocol was followed. It involved dividing rats randomly in different groups – Sham, BCNI, Vehicle (in some), stem cell group, co-intervention group, and combined group (Stem cell and Co-intervention). Flowchart depicts stepwise approach carried out in animal experiments (Figure 2). Stem cells used included – ADSC (16 studies), BMSC (8 studies), and others (5 studies). Most studies used Sprague-Dawley (SD) rats, total of about 1,017, while only one study used white rats (15). Details are provided in Table 1.

Flowchart depicting method of research in animal experiments.
Cavernous injury technique
Bilateral crush injury was most common form of cavernous nerve injury and used in 21 studies.14–18,20–26,30,31,34–39,41 Usually, this involved using a non-serrated hemostat away from major pelvic ganglion (MPG). In five studies, cavernous nerve injury was caused by transection injury,13,32,33,38,40 in two studies electric coagulation,19,27 and in one study Cryo-injury 28 was used.
Co-Interventions and modifications
Some studies used certain co-interventions or modifications to enhance the effect of stem cell intervention. Co-interventions included brain-derived neurotrophic factor (BDNF) in six studies;14,27,30,34,37,41 oral Icariside II (ICA II) in two studies;13,22 and low shock wave therapy and oral Udenafil were used in one study each.26,34 Modifications included use of fibrin scaffolds, Matrixen (biocompatible polymer), exosomes, nanotechnology, and super-paramagnetic iron oxide nanoparticles.
Route of administration
Most common route of administration of stem cells was intracavernosal route. It was used in 17 studies.13,14,16–18,20,21,23,24,27–30,35,38–40 The usual technique for IC injections (ICIs), included rolling up the prepuce to expose the penis and injecting to the lateral aspect of the penis. The needle was inserted around 3–4 mm. Before injection, drainage via the dorsal vein was halted by circumferential compression of the base of the penis using external compression (like an elastic band). The compression was released in around 1 min after injection of cells.
In four studies, stem cells were injected directly to MPG or cavernous nerves (periprostatic implantation, PPI).15,31,36,37 In five studies, ICI was used in combination with either MPG or PPI.22,25,32,33,41 For PPI of stem cells, different scaffolds like Fibrin or Matrixen were used. In most studies, mixtures were instilled into fissures between vesico-prostatic junction and seminal vesicles. In two studies, stem cell infusion was done around injured nerve.26,34 In one study, stem cells were administered through intravenous route (right jugular vein). 19 The most common dose of stem cells used is 1.0 × 106 cells.
ICP measurement
Initially, the number of studies providing data in a suitable format for analysis was evaluated, along with the number of animals. A total of 22 studies provided data suitable for meta-analysis. This consisted of 13 studies in the ADSC subgroup, 7 in the BMSC subgroup, and 2 in the Mixed subgroup. Data from a total of 909 animals were collected. Information on the number of studies on which data in each treatment group were collected, along with the pattern of the treatment combinations, was analyzed using a network map.
ADSCs
The first set of analyses considered the ADSC studies only. Both direct comparisons only and a network meta-analysis were performed. The results of both sets of analyses are shown in Table 3. Both analyses show the mean difference between each pair of treatments, in addition to corresponding CIs and the significance of the group differences. On comparing, stem cell group performed significantly better than BCNI group as traditional meta-analysis revealed difference of 27 (95% CI, P value <0.001) and network meta-analysis revealed difference of 28 (95% CI, P value <0.001). Overall, the traditional meta-analysis and network meta-analysis gave fairly similar results. Typically, the same pairs of groups varied from each other (or not) in both sets of analyses. As expected, all groups were found to have significantly lower values than the sham group.
Summary of meta-analysis results.

ADSC, adipose-derived stem cell; BCNI, bilateral cavernous nerve injury; BMSC, bone marrow–derived stem cell; CI, confidence interval.
Differences reported as Group 2 minus Group 1.
The BCNI group had significantly lower ICP values than all other groups, with the exception of the vehicle group, where no difference was observed. The traditional meta-analyses suggested a very high degree of heterogeneity between the study results for all comparisons. A graphical illustration of these direct comparisons between groups is shown in a Forest plot in Figure 3.

Forest plots for direct comparisons (ADSC studies – left side, BMSC studies – right side).
BMSCs
A similar set of analyses was performed for the BMSC studies. The meta-analysis results, using both approaches, are summarized in Table 3. The results suggested that again the sham group tended to have the highest values. On comparing, again stem cell group performed significantly better than BCNI group as traditional meta-analysis revealed difference of 23 (95% CI, P value <0.001) and network meta-analysis revealed difference of 21 (95% CI, P value <0.001). For the traditional meta-analyses, the I2 values indicated heterogeneity between studies. For these studies, the vehicle group performed worst, with the network meta-analyses suggested significantly lower ICP values than all other groups. A graphical illustration of the results for the direct comparisons is shown in a Forest plot in Figure 3.
ICP/MAP ratio
ICP and MAP ratio was evaluated from 26 studies;13–37,39 3 studies did not provide ICP/MAP ratio values.38,40,41 We found mean ICP/MAP ratio was higher in stem cell group (0.51) compared with BCNI group (0.25). Further for combined intervention group, ICP/MAP ratio was observed to be even higher than stem cell group at 0.65 suggesting that the co-interventions further enhanced the benefit (Figure 4).

Mean ICP/MAP ratios.
Histological/molecular evaluation
All 29 studies evaluated penile tissue as well as MPG (studies which involved periprostatic intervention); 21 studies reported an increase in level of neuronal nitric oxide synthase (nNOS), and 26 studies reported either increase in smooth muscle content or increase in ratio of smooth muscle to collagen ratio. Other changes reported included anti-apoptotic role played by stem cells. The summarized results are given in Table 4.
Results from histological/molecular evaluation.
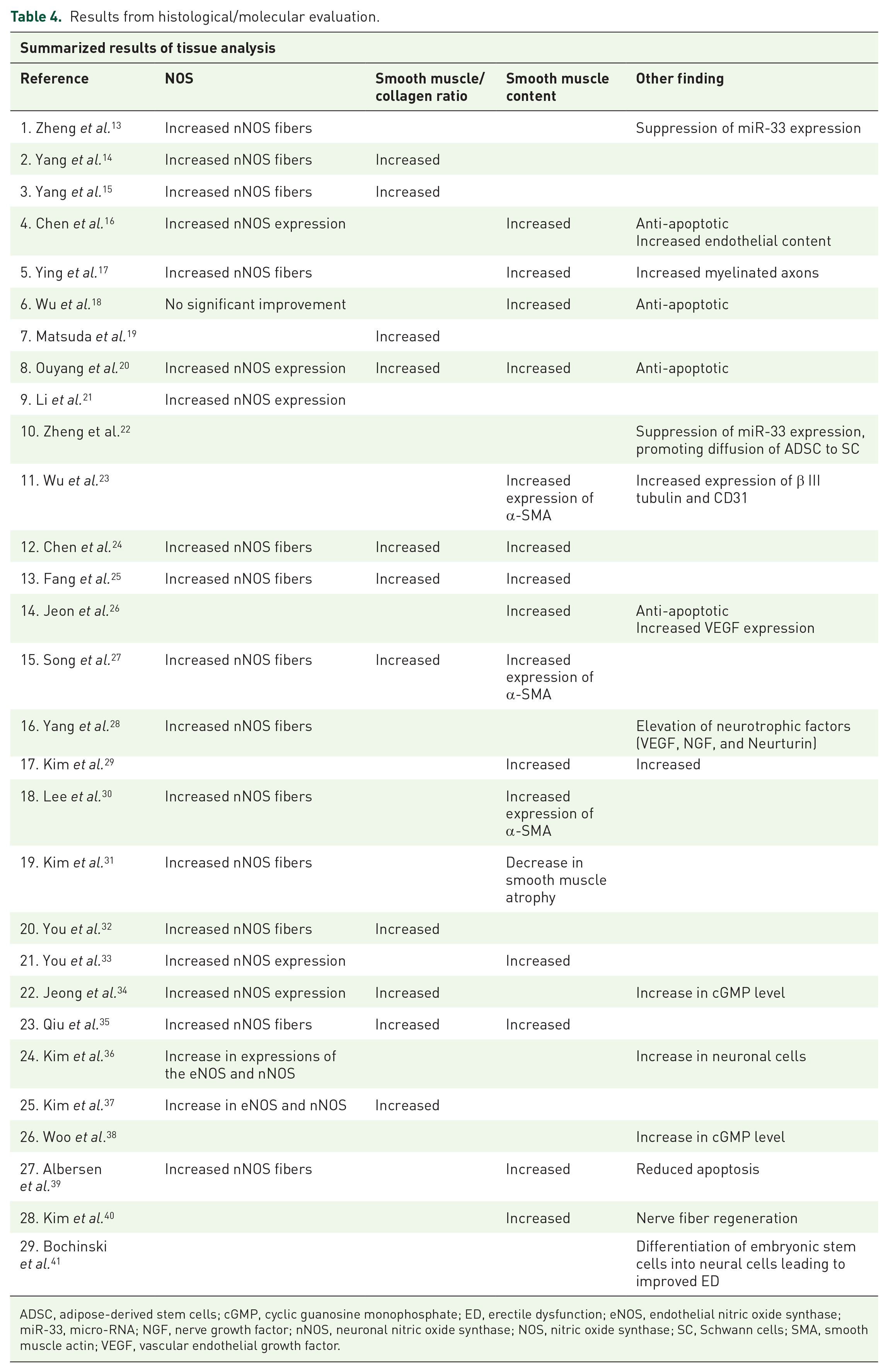
ADSC, adipose-derived stem cells; cGMP, cyclic guanosine monophosphate; ED, erectile dysfunction; eNOS, endothelial nitric oxide synthase; miR-33, micro-RNA; NGF, nerve growth factor; nNOS, neuronal nitric oxide synthase; NOS, nitric oxide synthase; SC, Schwann cells; SMA, smooth muscle actin; VEGF, vascular endothelial growth factor.
Human studies
The three phase I/II trials included in this study included two open label clinical trials and one open label extension study.42–44 The trials included patients who had ED post-RP and failed to recover using conventional therapy. Open-label trials can be used to compare treatments or gather additional information about the long-term effects in the intended patient population. Since all three trials included patients who had failed to recover on conventional therapy, these three trials were non-comparative and looked at long-term effect of stem cells on post-RP ED. One of the trials was open label extension. 43 A total of 35 patients were included in three trials. The results are summarized in Table 5.
Outcomes of SCT in human trials.

EHS, Erection Hardness Score; IIEF, International Index for Erectile Function; NA, not available; SCT, stem cell therapy; SHIM, Sexual Health Inventory for men.
IIEF score (International Index For Erectile Dysfunction): Two trials used IIFF-15 score and found there was an increase in score; one study revealed an increase from baseline of 25.3 to 39.7 at 6 months, 42 and the other study indicated an increase from 18.7 to 46.6 for same duration. 43 One trial used IEFF-5 scoring and found that in continent group of patients, it increased from 6 to 16 in a 6-month period; however, there was no improvement in incontinent group.
EHS: One trial reported an elevation in EHS from baseline 1.3 to 2.6 in 6 months, 42 the second reported increase from 1.8 to 3.3 for same duration, 43 and third trial indicated an increase from 1 to 3 at 6 months in the continent group. 44 However, there was no change in incontinent group.
Penile length: In one trial, penile length was also considered. It increased from 12.4 to 13.3 cm by end of 3 months. However, by end of 6 months, it was around 12.9 cm. 42
Adverse outcomes: One trial reported mild postoperative pain at the bone marrow (BM) aspiration with no evidence of prostate cancer reactivation. 42 Second trial reported 8 men developed transient redness and swelling at injection site. 5 men in this series also developed minor abdominal wall hematomas (post-liposuction). 44 The third trial has not reported any adverse outcome 43 (Table 2).
Discussion
Cavernous injury is widely accepted to be responsible for post-RP ED due to the damage caused by incision, heat, and mechanical stress. 48 Although, nerve-sparing RP was introduced 30 years ago, ED still remains a challenge with RP surgery.49,50 A recent prospective series has shown that up to 75% of men reported ED, 1 year after RP with minimal difference between robotic and open surgery groups. 51 Therefore, it is now commonly believed that, although leaving the cavernosal nerves (CNs) intact, nerve-sparing RP still causes subtle changes that are not obvious to the surgeons. 52 These changes cause CNs to undergo Wallerian degeneration and eventually lose their connection to the corpora cavernosa. 53 Alternatively, the surgery-incurred insults may temporarily prevent the CNs from releasing nitric oxide (NO) into the corpus cavernosum (CC), and without NO-induced engorgement, the penile tissue becomes hypoxic and its cavernous musculature is replaced by collagens and fibrous scar tissue.52,53
SCT is among different novel approaches being investigated to manage post-RP ED. Stem cells are undifferentiated or partially differentiated cells and are classified as totipotent (e.g. zygote), pluripotent [e.g. embryonic stem cells (ESCs)], multipotent (e.g. hematopoietic and MSCs), and unipotent according to the number of cell lines in which they could be differentiated. Stem cells have been used for the treatment of cardiovascular, 54 neurological, 55 autoimmune, 56 and hematologic diseases. 57 In recent years, SCT has been proposed for the treatment of ED as stem cells can differentiate to endothelial, neuronal, or smooth muscle cells, and therefore restore possible structural damage in the penile tissue. 58 Most commonly used stem cells used in the treatment of ED are MSCs. MSCs are able to demonstrate therapeutic effects by their ability to produce an array of bioactive molecules including growth factors capable of inducing increased cell proliferation and immunomodulatory effects. 59 They lead to stimulation of angiogenesis and revascularization, modulation of immune and inflammatory responses, inhibition of apoptosis, and trophic effects such as stimulation of mitosis, proliferation, and differentiation of intrinsic stem/progenitor cells. 60 This is termed as paracrine action of stem cells, because few stem cells can be detected after transplantation, and almost no direct evidence supports the theory that transplanted stem cells have differentiated into vascular endothelial cells, smooth muscle cells, or nerves. 61
The current meta-analysis examined 29 preclinical studies of SCT in the treatment of ED secondary to BCNI in rats and also evaluated three human clinical trials. The animal studies were analyzed for ICP measurement, ICP/MAP ratio, and histological/molecular results. Our study focused mainly on ICP measurements as it is considered a reliable method for direct measure of erectile function. It allows for the acquisition of data on basal ICP, peak ICP, plateau ICP, time to erection and detumescence time, duration of response. 62
Meta-analysis of ICP values (post-SCT) including ADSC as well as BMSC stem cell groups revealed statistically significant improvement in ED in SCT intervention group as compared with BCNI group. There is minimal literature in the form of a systemic review or a meta-analysis available regarding ICP measurements in ED in BCNI rats to compare. We also evaluated ICP/MAP ratio for animal studies. We found that there is an increase in ICP/MAP ratio in stem cell intervention group as compared with BCNI group. A previous meta-analysis based on ICP/MAP ratio had also revealed that there is a significant difference of erectile functions between stem cell transplantation group and control group. 63 We noticed that for both ICP (meta-analysis) and ICP/MAP ratio, the efficacy of SCT was enhanced by the addition of co-interventions. This has been reported previously as well. 63
In case of animal studies, histology of penile tissue post-SCT was also analyzed. It revealed an increase in NOS, ratio of smooth muscle to collagen, and anti-apoptotic activity in intervention groups. In a previous systematic review, it has been established that SCT does lead to structural changes in CC resulting in increased endothelial and smooth muscle cell markers, increase in neural cell markers, decrease in apoptosis, as well as a decrease in collagen content. 48
The three human trials in post-RP patients did reflect improvement in SHIM and EHS scores after SCT. The trials have revealed that SCT in humans has a potential efficacy suggested by a significant improvement in IIEF scores, erectile function with minimal adverse effects. However, in one trial, the SCT therapy results could not produce desired results in men having urinary incontinence. 44 This has been already established that urinary continence seems to be a prerequisite for having sexual intercourse post-RP. 64
Adult stem cells in regenerative medicine do have issues and concerns. The most important concern being development of recurrences as well as other tumors in patients receiving SCT due to conflicting evidence that adult stem cells can promote tumor genesis. 65 Several hypotheses have proposed that the events in either stem and/or differentiated cells, such as genomic instability, inflammatory microenvironment, cell fusion, and lateral gene transfer, should be considered as the possible origin of cancer stem cells (CSCs), are responsible for the sustained and uncontrolled growth of malignant tumors, and are proposed to play significant roles in metastasis and recurrence 66 but also the chemotaxis and subsequent migration of patient stem cells to the hypoxic tumor mass promoting angiogenesis; however, the specific response of the stem cell to the malignant mass may well be due to the malignancy type. 59 In the majority of animal trials, animal was sacrificed at around 4 weeks, so this aspect has not been addressed. The issues with human trials included in this study include very limited number of patients, SCT treatment started after a gap of few months to years, sometimes overlapping both SCT with other therapies, no long-term follow-up details, and also pre-screening for risk factors, and the presence of secondary malignancy may well be required to reduce risk factors.
In order to understand SCT in post-RP patients, a double-blind randomized controlled study is need of hour; however, it will not be an easy task, as a number of questions need to be addressed – When to start? Which type of stem cell to use? What quality control of stem cells to be used? What source? What is ideal dose? Which route? How to do follow-up?
Conclusion
Our results confirm that SCT does improve the erectile function in rats having cavernous nerve injury. Furthermore, co-interventions and specific modifications do improve efficacy of SCT. Similarly, early human results have shown promising results. Thus, regenerative medicine approach to the treatment of ED appears to hold much promise.
Supplemental Material
sj-docx-1-tau-10.1177_17562872221086999 – Supplemental material for Is there a role for stem cell therapy in erectile dysfunction secondary to cavernous nerve injury? Network meta-analysis from animal studies and human trials
Supplemental material, sj-docx-1-tau-10.1177_17562872221086999 for Is there a role for stem cell therapy in erectile dysfunction secondary to cavernous nerve injury? Network meta-analysis from animal studies and human trials by Mudassir M. Wani, Bhavan P. Rai, William Richard Webb and Sanjeev Madaan in Therapeutic Advances in Urology
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Authors recieved no financial support for this research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.