
Abstract
Objective:
The objective of this study is to determine the preoperative patient characteristics predicting prolonged length of hospital stay (pLOS) following robotic-assisted radical prostatectomy (RARP).
Methods:
The National Surgical Quality Improvement Program (NSQIP) database was used to select patients who underwent RARP without other concomitant surgeries between 2008 and 2016. Patients’ demographics, comorbidities, and laboratory markers were collected to evaluate their role in predicting pLOS. The pLOS was defined as length of stay (LOS) >2 days. A multinomial logistic regression was constructed adjusting for postoperative surgical complications to assess for the predictors of pLOS.
Results:
We obtained data for 31,253 patients of which 20,774 (66.5%) patients stayed ⩽1 day, 6993 (22.4%) patients stayed for 2 days, and 3486 (11.2%) patients stayed for >2 days. Demographic variables – including body mass index (BMI) <18.5: odds ratio (OR) = 2.8, 95% confidence interval (CI) = [1.7–4.8]; smoking: OR = 1.2, 95% CI = [1.1–1.4]; and dependent functional status: OR = 3.1, 95% CI = [1.6–6.0] – were predictors of pLOS. Comorbidities – such as heart failure: OR = 4.6, 95% CI = [2.0–10.8]; being dialysis dependent: OR = 2.7, 95% CI = [1.4–5.0]; and predisposition to bleeding: OR = 2.0, 95% CI = [1.5–2.7] – were the strongest predictors of extended hospitalization. In addition, pLOS was more likely to be associated with postoperative bleeding, renal, or pulmonary complications.
Conclusion:
Preoperative patient characteristics and comorbidities can predict pLOS. These findings can be used preoperatively for risk assessment and patient counseling.
Introduction
Prostate cancer is the most common non-cutaneous malignancy in the United States with 248,530 new diagnoses and 34,130 deaths in 2021. 1 It is estimated that a third of patients with prostate cancer will undergo radical prostatectomy (RP). 2 Robotic-assisted radical prostatectomy (RARP) represents between 45% and 80% of all RP performed in the United States and is the preferred surgical modality to treat clinically significant localized cancer.3,4 Evidence from the only available randomized trial comparing open and RARP showed that the two procedures have similar two-year functional and oncological outcomes. 5 Moreover, in a randomized clinical trial comparing the five-year outcomes of laparoscopic and robotic RP, patients who underwent RARP had higher continence and potency rates. 6 RARP is also associated with less intraoperative adverse events, lower estimated blood loss, and shorter hospital stay.7,8 Using the National Surgical Quality Improvement Program (NSQIP) database, Monn et al. 9 showed that, in comparison with RARP, open RP has on average a day increase in length of stay (LOS). Accordingly, most patients are discharged at the first or second postoperative day following RARP. 9
The length of hospital stay is a health indicator used by medical services to assess the quality of care delivered in hospitals. 10 Effectively, prolonged length of hospital stay (pLOS) is associated with higher rates of hospital-acquired infections, increased side effects from medications, and elevated mortality rates. 10 At the economical level, pLOS begets increased medical fees and overall social costs. 11 In 2010, the US Health Care Cost and Utilization Report announced that inpatient services accounted for about 21% of national health care expenditures. 12 Furthermore, the surgery-specific estimated LOS is utilized by many sponsoring parties, like insurance companies, to decide on pre-authorization and reimbursement of patients. 12 In addition, medical resource allocation is of paramount importance when discussing public health issues on a national and international level. Effectively, LOS is an important indicator of resource utilization and a reason for increased hospital cost. 13 As such, the ability to identify the preoperative factors contributing to pLOS is important.
The determinants of a pLOS include preoperative, intraoperative, and postoperative factors. 14 Although spaced out in time, these factors are highly intertwined where one preoperative factor can be a predictor of successive intraoperative and postoperative events. Nevertheless, at the patient’s presentation to the clinic, the surgeon can only rely on the preoperative factors to predict the likelihood of pLOS. In view of the increase use of minimally invasive surgery and the increase concern about LOS as a quality indicator and a financial determinant, we sought to determine the preoperative predictors of pLOS following RARP. Therefore, if the patients’ preoperative factors predict pLOS, then the patient’s medical profile would become a reliable indicator.
Methods
Patients
We used the American College of Surgeons’ National Surgical Quality Improvement Program (ACS-NSQIP) database, a prospectively filled and validated 30-day outcomes registry from 708 hospitals (of which 622 are in the United States) in 2018, to analyze patients’ data. This is an existing de-identified database and does not constitute human subject research; hence, no institutional review board approval was needed. Using the current procedural terminology (CPT) code for RARP (55866), we selected patients who underwent RARP with or without lymphadenectomy for prostate cancer without any other concomitant surgeries, using general anesthesia, between 2008 and 2016. We collected anonymous data entered by ACS trained surgical clinical reviewers, including demographics, preoperative comorbidities, and laboratory values.
Outcome selection
We categorized all patients into the ordinal outcome LOS: LOS ⩽ 1 day, LOS = 2 days, and LOS > 2 days. 9 While LOS ⩽ 1 day represents the most common expected LOS for RARP in the literature, 15 we have created two additional groups to capture patients with moderate LOS (LOS = 2 days representing 75% percentile LOS in large RARP cohorts9,15) and pLOS. The category LOS = 2 days was created to account for delays due to logistics or conditions requiring medical observation, and the cutoff for pLOS was set at LOS > 2 based on previous studies and clinical experience.16,17 Thus, we hypothesize that the predictors associated with pLOS are different than either LOS ⩽ 1 day or LOS = 2 days. All patients were categorized into one of the three groups, and only patients with missing LOS were excluded. The rate of postoperative surgical complications were categorized by organ system: respiratory (pneumonia and unplanned intubation), thromboembolism (pulmonary embolism, deep vein thrombosis, and thrombophlebitis), wound (surgical site infections, SSIs; organ space SSI; and wound dehiscence), renal (acute renal failure, progressive renal failure requiring dialysis, and urinary tract infections), sepsis (sepsis and septic shock), cardiac (cardiac arrest requiring cardiopulmonary resuscitation and myocardial infarction), and bleeding (bleeding requiring transfusion) were compared among the three LOS categories.
Covariates
We collected information on patient age, body mass index (BMI), race (White versus non-White), current smoker status, dependent functional status, patient comorbidities, bleeding diathesis, and preoperative laboratory parameters, including white blood count (WBC), serum creatinine, and hematocrit. Due to low proportions in their respective categories, we have included ‘Black or African American’, ‘Asian’, ‘American Indian or Alaska Native’, and ‘Native Hawaiian or Pacific Islander’ into the non-White race category. Further information on covariate definition is available in Table 1.
Demographics, comorbidities, and laboratory markers stratified by postoperative length of stay..

COPD, chronic obstructive pulmonary disorder; SD, standard deviation; WBC, white blood count.
Whether patient has smoked cigarettes within the 12 months prior to admission.
Partially or totally dependent, requiring some or total assistance from another person for daily activities as well as patients with prosthetic devices.
Diagnosis of hypertension documented in patient’s medical records and the condition is severe enough that it requires long-term treatment (>2 weeks) with antihypertensive medication within 30 days of the patient’s procedure.
Chronic or persistent condition that places the patient at risk of excessive bleeding including chronic anticoagulation that has not been discontinued prior to the procedure.
Regular oral or parenteral corticosteroids or immunosuppressant medication use for a chronic condition within 30 days of procedure.
Statistical analysis
A chi-square test was carried out for the categorical variables, and one-way analysis of variance (ANOVA) was conducted for the continuous variables and the categorical outcome LOS (LOS ⩽ 1 day, LOS = 2 days, and LOS > 2 days). To address our hypothesis and capture the variability in the predictors of moderate LOS (LOS = 2 days) and pLOS (LOS > 2 days), a multinomial logistic regression was done using LOS ⩽ 1 as a reference and adjusting for patients’ demographics, preoperative comorbidities, and laboratory data. Missing values were not imputed, as the percentage of missing for each variable was less than 10%. A p < 0.05 for two-tailed tests was set a priori as a cutoff for statistical significance. The Statistical Package for the Social Sciences (IBM SPSS for Windows, version 24; IBM Corp., Armonk, NY, USA) was used to report the results.
Results
Among 31,253 patients, 20,774 (66.5%) patients stayed ⩽1 day, 6993 (22.4%) patients stayed for 2 days, and 3486 (11.2%) patients stayed for >2 days. Notably, extreme BMI (<18.5 and ⩾30), smoking, non-White race, and functionally dependent patients were associated with pLOS (p < 0.0001 for all variables; Table 1). Patients with pLOS were also more likely to have dyspnea, chronic obstructive pulmonary disorder (COPD), congestive heart failure (CHF), hypertension, diabetes mellitus (DM), dialysis, and a predisposition to bleeding (p < 0.0001 for all variables; Table 1). Moreover, preoperative laboratory findings including WBC >11,000 cells/mm3 (p = 0.0005), serum creatinine >1.2 (p < 0.0001), and hematocrit <40% (p < 0.0001) were also associated with pLOS. Patients with pLOS had a higher average operative time (239.1 ± 93.6 min) than patients who had LOS ⩽1 day (194.9 ± 60.7 min) (p < 0.0001). Some factors like disseminated cancer at time of surgery, open/infected wounds, and chronic steroid use were not associated with LOS.
At the multivariable level, and in comparison with patients with LOS ⩽ 1 day, every 10-year increase in age resulted in 17% increased risk for pLOS (Table 2). Functional dependence and being underweight were the most significant demographic factors predicting pLOS – odds ratio (OR) = 2.65, 95% confidence interval (CI) = [1.4–5.0] and OR = 3.1, 95% CI = [1.6–6.0] – respectively. Other demographic factors – including a smoker status: OR = 1.2, 95% CI = [1.1–1.4] and non-White race: OR = 1.5, 95% CI = [1.4–1.7] – were also associated with pLOS. The most notable contributing comorbidities were CHF: OR = 4.6, 95% CI = [2.0–10.8]; dialysis dependent: OR = 2.8, 95% CI = [1.7–4.8]; and predisposition to bleeding: OR = 2.0, 95% CI = [1.5–2.7]. Other comorbidities delaying discharge included pulmonary compromise, chronic steroid intake, DM, and hypertension requiring medication (Table 2). Effectively, a serum creatinine >1.2, WBC >11,000 cells/mm3, and hematocrit <40% had significant impact on pLOS: OR = 1.28, 95% CI = [1.15–1.43]; OR = 1.31, 95% CI = [1.06–1.62]; and OR = 1.39, 95% CI = [1.25–1.54], respectively. Furthermore, every 20-min increase in operative time resulted in 18% increased risk of pLOS (Table 2).
Predictors of prolonged length of hospital stay.
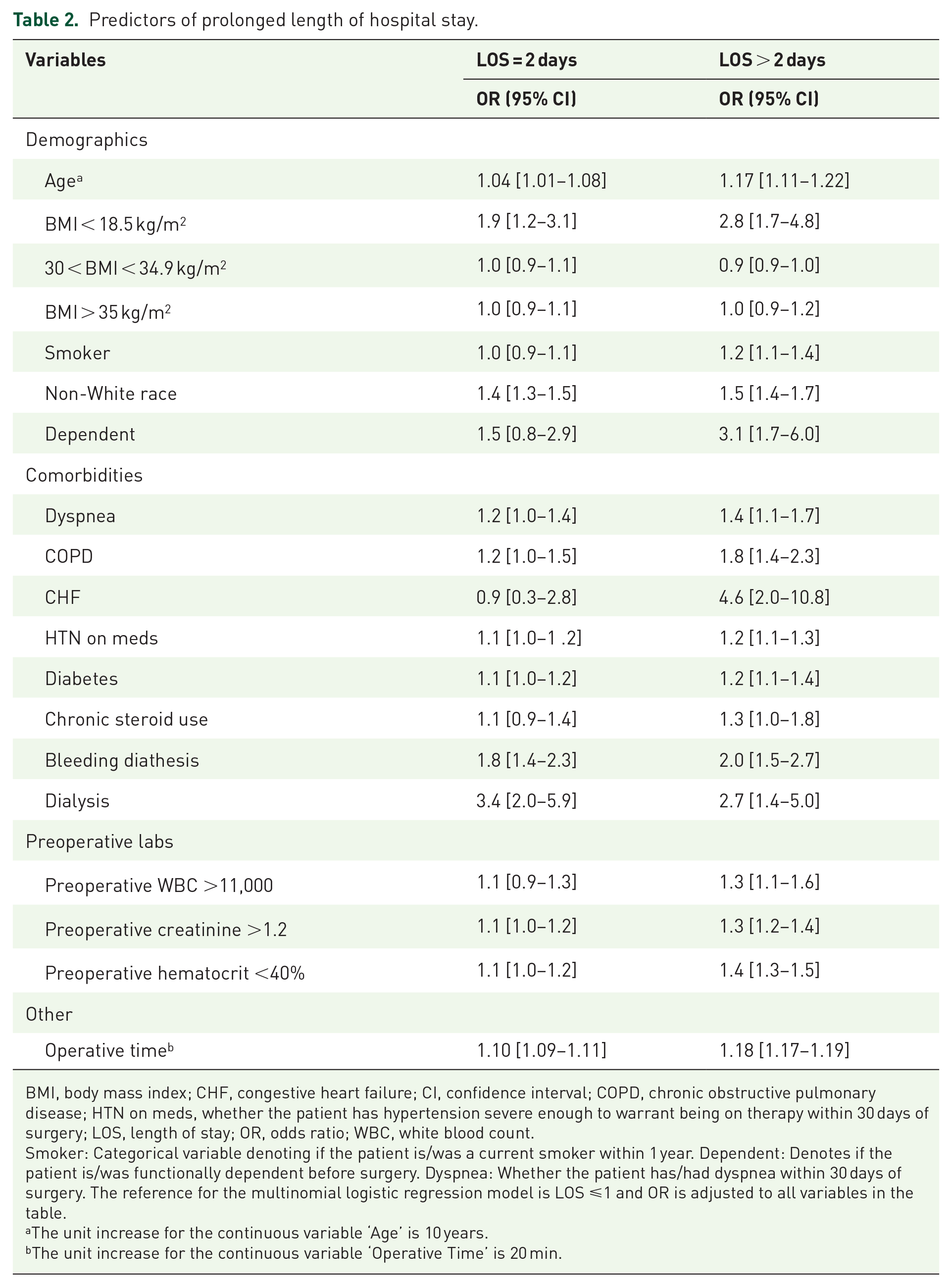
BMI, body mass index; CHF, congestive heart failure; CI, confidence interval; COPD, chronic obstructive pulmonary disease; HTN on meds, whether the patient has hypertension severe enough to warrant being on therapy within 30 days of surgery; LOS, length of stay; OR, odds ratio; WBC, white blood count.
Smoker: Categorical variable denoting if the patient is/was a current smoker within 1 year. Dependent: Denotes if the patient is/was functionally dependent before surgery. Dyspnea: Whether the patient has/had dyspnea within 30 days of surgery. The reference for the multinomial logistic regression model is LOS ⩽1 and OR is adjusted to all variables in the table.
The unit increase for the continuous variable ‘Age’ is 10 years.
The unit increase for the continuous variable ‘Operative Time’ is 20 min.
Most of the postoperative complications were among patients with pLOS (Supplementary Figure 1). Intraoperative or postoperative bleeding requiring transfusion (8.18%), renal (2.15%), and pulmonary (1.41%) complications were the most frequent adverse events in these patients. Furthermore, the 30-day mortality rates were 0.06%, 0.09%, and 0.26% for LOS ⩽ 1 day, LOS = 2 days, and LOS > 2 days, respectively (Supplementary Figure 1).
Discussion
In our study, we found that demographics, comorbidities, and preoperative laboratory values were independent predictors of pLOS. In addition, pLOS was more likely to be associated with postoperative bleeding, renal, or pulmonary complications.
Using the NSQIP data between 2003 and 2004, Wallner et al. reported on the predictors of pLOS among all urological surgeries (without performing sensitivity analyses among the surgery type). Similar to our results, the authors found that elevated serum creatinine, low hematocrit, history of cardiac events, longer operative time, and intraoperative transfusion extended the LOS. 18 In a NSQIP study on 864 patients undergoing radical nephrectomy, Lorentz et al. 12 found that age, hematocrit level, heart failure, functional dependence, and open procedures were associated with longer recovery. As for patients undergoing prostatectomy, Coelho et al. 16 showed that age, American Society of Anesthesiology score >3, large prostate, African American race, and prolonged operative times were the main predictors of pLOS. In addition, Charlson comorbidity index >2 was also associated with LOS > 1 day in patients undergoing RARP. 19 Huang et al.’s 20 work on 793 patients who underwent prostatectomy in China revealed that operation time, intraoperative blood loss, preoperative leukocytosis, and open surgery were the determinants of prolonged hospital stay. Nevertheless, their average LOS was much higher (11.7 days) than ours (1.66 days) which could be attributed to differences in the health care system, discharge policies, and other sociocultural factors. 20
In our study, the preoperative laboratory markers predicted pLOS as these values insinuate a worse overall health. Furthermore, heart failure and dependent functional status were the most important predictors. Froehner et al. 21 have also shown that heart failure is one of the comorbidities that increase overall post-prostatectomy morbidity and mortality. In parallel, patients’ functional status is a very important predictor of postoperative outcome and has been studied in many surgical procedures, including bariatric and orthopedic surgeries.22,23
Through this study, patients were stratified according to their medical profile contributing to pLOS in a very common oncological procedure. We found that specific patient characteristics and comorbidities contribute to pLOS. These results could be further leveraged to develop a clinical predictive tool surgeons could use to identify and counsel high-risk patients on the expected postoperative course. 12 Other tools such as frailty indices have been evaluated to predict morbidity and mortality following RARP. 24 Strategies to mitigate postoperative morbidity are becoming central to a value-based health care system in the United States where there is a paradigm shift from fee-for-service to bundled payments. 25 As such, the preemptive optimization of medical comorbidities by a multidisciplinary team could mitigate or prevent postoperative adverse events. Besides, patients deemed as high risk for pLOS and postoperative complications could be offered alternative non-surgical treatments such as external beam radiation therapy.
Some limitations inherent to the database include an inability to account for clinic-pathologic data such as prostate size, tumor grade, or stage. Therefore, we could not assess whether higher grade, extracapsular extension, or seminal vesical invasion influenced the LOS. In addition, the database lacks information on the socioeconomic status and whether the procedure was a salvage or primary prostatectomy. Similarly, the reconstruction technique of RP could play a role in the catheterization time and postoperative complications, including anastomosis stricture and urine leakage. 26 For instance, Porpiglia et al. 27 have devised an intraoperative anastomosis quality score for RARP which was utilized to categorize patients based on the urethral and bladder neck features. The authors demonstrated that patients with poor anastomosis quality had longer hospitalization and increased postoperative complications. 27 As such, this tool could be utilized to optimize postoperative management and minimize postoperative complications that could prolong hospital stay. Moreover, the NSQIP database captures only early complications and mortality within 30 days of follow-up, so urological complications that are encountered later including lymphocele formation, anastomotic urine leak, or anastomotic stricture could not reported. Despite these limitations, these results are helpful in risk stratification of patients presenting for RARP.
Conclusion
Preoperative patient characteristics, comorbidities, and baseline metabolic profile can be used as predictors of a prolonged hospital recovery following RARP. This information can be used for counseling and selection of treatment options in patients with localized prostate cancer.
Supplemental Material
sj-jpg-1-tau-10.1177_17562872221080737 – Supplemental material for Patient characteristics predicting prolonged length of hospital stay following robotic-assisted radical prostatectomy
Supplemental material, sj-jpg-1-tau-10.1177_17562872221080737 for Patient characteristics predicting prolonged length of hospital stay following robotic-assisted radical prostatectomy by Albert El Hajj, Muhieddine Labban, Guillaume Ploussard, Jabra Zarka, Nassib Abou Heidar, Aurelie Mailhac and Hani Tamim in Therapeutic Advances in Urology
Footnotes
Acknowledgements
The American College of Surgeons’ National Surgical Quality Improvement Program (ACS-NSQIP) and the hospitals participating in the ACS-NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Authors’ note
Abstract published in Journal of Endourology as part of the 37th World Congress of Endourology.
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This is a retrospective database; therefore, ethical approval is not needed for de-identified database.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of data and material
The data belong to the American College of Surgeons’ National Surgical Quality Improvement Program (ACS-NSQIP) and access is given to participating hospitals only.
Code availability
Codes are available upon request from the primary investigator.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.