
Abstract
Introduction:
Emphysematous pyelonephritis (EPN), an acute necrotizing infection of the kidney and surrounding tissues, is associated with considerable mortality. We evaluated how existing critical care scoring systems could predict the need for intensive care unit (ICU) management for these patients. We also analyzed if CT-imaging further enhances these predictive systems.
Patients and Methods:
A retrospective analysis of 90 consecutive patients diagnosed clinico-radiologically with EPN from January 2011 to September 2020. Five scoring systems were evaluated for their predictive ability for the need for ICU management and mortality risk: National Early Warning Score (NEWS), Modified Early Warning Score (MEWS), ‘quick’ Sequential Organ Failure Assessment score (qSOFA), Systemic Inflammatory Response Syndrome score (SIRS), and Sequential Organ Failure Assessment score (SOFA). CT images were classified as per Huang & Tseng and evaluated as stand-alone or added to the different predictive models. Receiver operating characteristic (ROC) curves were plotted for each critical care score and CT-Class using logistic regression, to obtain the area under curve (AUC) value for comparison of ICU admission predictability. Patients were analyzed up till discharge.
Results:
Ninety patients were diagnosed with EPN. Twenty-six patients required ICU management and nine patients died. The best scoring system to predict the need of early ICU management is NEWS (AUC 0.884). CT Class had no independent predictive power, nor did it add significantly to improvement in most of the early warning scoring systems, but rather guided us to the need for radiological, endourological or surgical intervention.
Conclusion:
In patients with EPN, the NEWS scoring system predicts best the requirement of ICU care. It aids in triage of patients with EPN to appropriate early management and reduce mortality risk.
Introduction
Emphysematous pyelonephritis is a potentially fatal urologic emergency characterized by acute necrotizing parenchymal and perirenal infection often caused by gas-forming uropathogens. It is commonly associated with diabetes mellitus, urinary tract obstruction with or without associated renal and /or immune dysfunction.1–3 There has been a paradigm shift in its management and prognosis with the balance of treatment tilting in favor of aggressive medical management, with percutaneous or endourological drainage as indicated in case of urinary obstruction.4–7
However, there remains a need to better identify patients who would benefit from early ICU management, thereby obviating subsequent potentially unnecessary surgical intervention, improving renal salvage rates, and better overall patient outcomes.8–11 Systemic Inflammatory Response Syndrome (SIRS), Modified Early Warning Score (MEWS), National Early Warning Score (NEWS), Sequential Organ Failure Assessment Score (SOFA), and Quick Sequential Organ Failure Assessment Score (qSOFA) are among the clinical scoring systems used to predict patient outcomes in emergency care,12–16 in addition to its utility in the management of conditions leading to sepsis and/or multi-organ dysfunction syndrome (MODS).17–23
While in emergency care, decision making is based on different systems in use, it remains unclear which one performs best in EPN, and if the systems can be further improved including specific data based on the condition treated.
To address this, we assessed the individual predictive accuracy of each of five scoring systems -MEWS, NEWS, SOFA, qSOFA and SIRS, when applied to a large EPN cohort. In addition, we studied the different scoring systems in combination with the CT Class to assess any potential improvement in predicting the need for early and aggressive intensive care management.
Patients and methods
Study design and participants
A retrospective analysis of 90 consecutive patients with a clinico-radiological diagnosis of EPN from January 2011 up to September 2020 in our tertiary hospital, was conducted after obtaining approval from the Kasturba Medical College (KMC) and Kasturba Hospital (KH) Institutional Ethics Committee: IEC No: 583-2019.
Variables and scoring systems
Five scoring systems were applied using the appropriate clinical variables for calculating MEWS, NEWS, SIRS, qSOFA and SOFA scores (Supplemental Material Table 1). Patients were analyzed up till discharge. The individual CT Class was also analyzed independently and in combination with each scoring system, to assess patient outcomes, primarily, the need for ICU management, and secondarily, mortality. The need for ICU admission was taken in conjunction with the Critical Care Specialist and was primarily based on the need for support of two or more organ systems.
Definitions and management protocol
EPN is a clinico-radiological diagnosis, the hallmark finding being presence of intra-renal or extra-renal gas on non-contrast CT scan (NCCT). The appropriate stage was designated as per the Huang and Tseng 29 classification (Figure 1).

Huang & Tseng Emphysematous Pyelonephritis (EPN) Classification (a) Class 1 – Gas in the collecting system only, (b) Class 2 – Gas in the renal parenchyma without extension into the extra renal space, (c) Class 3A – Extension of the gas or abscess into the perirenal space, (d) Class 3B – Extension of the gas or abscess into the Para- renal space, (e) Class 4 – Bilateral EPN or solitary kidney with EPN.

(a) ROC curves of the various scoring systems. (b) Comparison of ROC curves of the various scoring systems with combination of CT Class.
Statistical analysis
The data were entered into the Microsoft Excel spreadsheet 2007 and analyzed with IBM SPSS version 22 software. Descriptive data were presented as mean and standard deviation (SD) for normally distributed continuous variables, and as median and interquartile range (IQR) for skewed variables. Data were presented as frequency (n) and percentages (%) for categorical data. Comparison of proportions was performed using the chi-square test and non- parametric data by Mann–Whitney U test. All results were considered significant at a P-value of < 0.05. Receiver operating characteristic curves were plotted for each score and CT-Class using logistic regression, to obtain the area under curve (AUC) value for comparison of ICU admission predictability.
Results
Class 2 EPN was the commonest type as detected by computed tomography in 35 (39%).
Class 4 EPN was seen in 12 patients. Bilateral EPN on presentation was seen in 11 (12%). One patient had a solitary kidney.
Baseline characteristics including 90 patients are depicted in Table 1.
Baseline Characteristics on 90 patients.

EPN, Emphysematous pyelonephritis.
Association with urolithiasis was observed in 22 (24%).
Blood culture was positive in 24 (27 %) patients including Escherichia coli (n = 22), Enterococcus faecalis (n = 1), and both (n = 1). Urine culture was positive in 31(34.4%) patients including E Coli (n = 23), Klebsiella pneumonia (n = 4), Enterococcus faecalis (n = 2), and Candida albicans (n = 2). It is noteworthy that the 2 patients with Candida were suffering from diabetes. Pus culture demonstrated 10 samples positive for E Coli, one for Klebsiella pneumonia, and one for Enterococcus. A similar microbiological culture pattern was observed in the 22 patients with urolithiasis. Papillary necrosis was demonstrated in four.
Deranged renal parameters were seen in 75 (83%) on presentation, of which 18 (2%) were oliguric. Eighteen patients had chronic kidney disease (CKD) (20%). Seventy five patients had acute kidney injury (AKI). Urinary diversion was required in 50/90 (56%), 40 (44%) underwent DJ ureteral stenting, 10 (11%) patients had percutaneous nephrostomy inserted, and 5 (6%) required percutaneous tube drain insertion into the peri/para nephric space. CT evaluation directed us to the need for radiological, endourological, or surgical intervention, especially in case of urinary obstruction.
Four patients (4.4%) underwent nephrectomy – one emergency, and three elective/staged. All made good clinical recovery. Renal replacement therapy by hemodialysis was required in seven (8%). Eventually 26 patients (29%) required ICU care, and 9 patients (10%) died. All nine patients that died were under ICU care.
Prediction findings from scoring systems
AUROC analysis demonstrated the predictability of the five scoring systems, listed in descending order: NEWS 0.884; MEWS 0.882; qSOFA 0.826; SOFA 0.790; and SIRS 0.749 (Figure 1(a)). All the scoring systems performed well, each achieving AUC > 0.7. NEWS was best at predicting the need for ICU admission, with a sensitivity of 65.4%, specificity of 89.1%, positive predictive value of 70.8%, and negative predictive value of 86.4%. (Table 2). Seventeen of the 26 ICU admitted patients (65.4%) had NEWS ⩾ 5, in comparison to 7 of the 64 non-ICU patients (10.9%) having NEWS ⩾ 5. The AUC of NEWS was found to be statistically significantly larger only to SIRS, both alone, and in combination with CT Class (Supplemental Material Tables 2 and 3).
Area under the ROC curve, sensitivity, and specificity data of the various scoring systems.
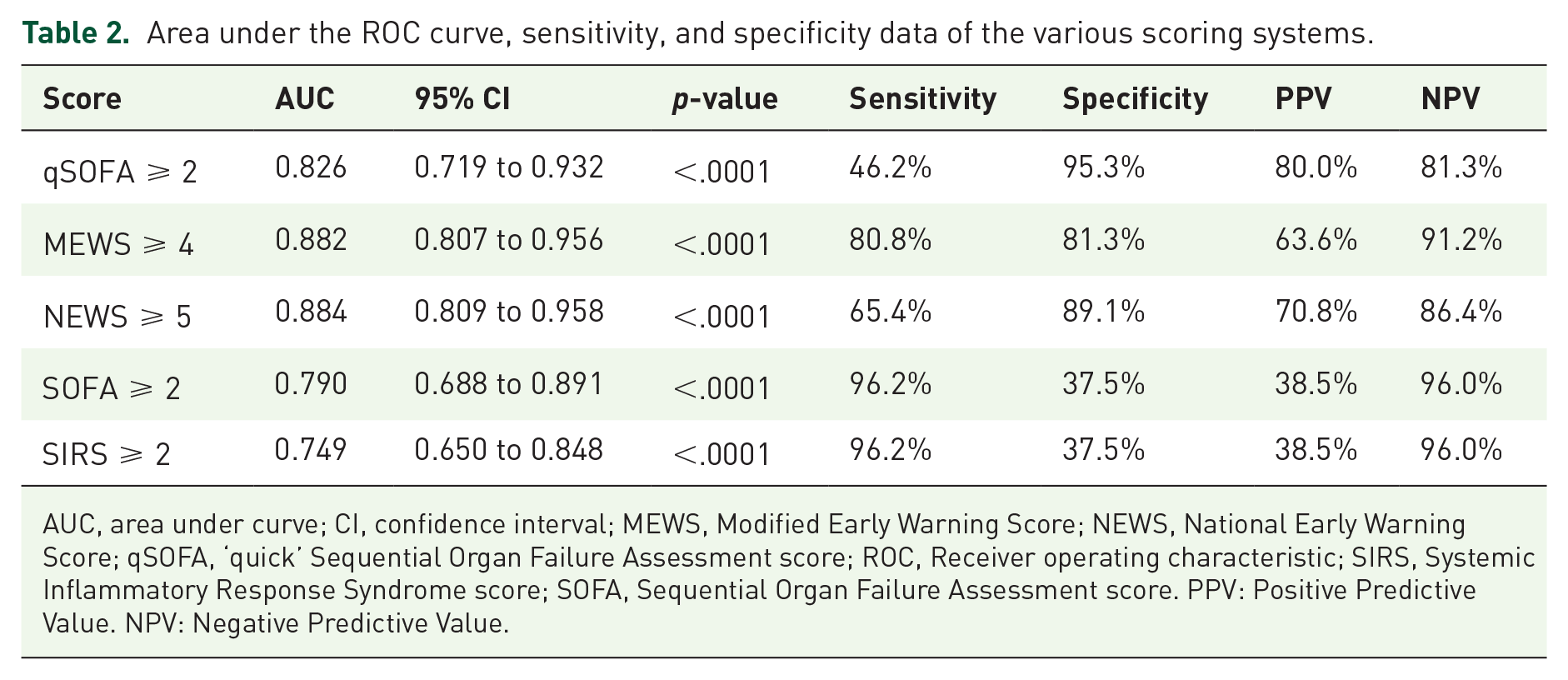
AUC, area under curve; CI, confidence interval; MEWS, Modified Early Warning Score; NEWS, National Early Warning Score; qSOFA, ‘quick’ Sequential Organ Failure Assessment score; ROC, Receiver operating characteristic; SIRS, Systemic Inflammatory Response Syndrome score; SOFA, Sequential Organ Failure Assessment score. PPV: Positive Predictive Value. NPV: Negative Predictive Value.
CT-Class did not have an independent predictive power, with an AUC of 0.667, (Supplemental Material Tables 4 and 5) but did improve the AUROC values when applied to the early warning scoring systems. (Supplemental Material Table 6) (Figure 1(b)). CT Class 3 EPN was associated with the highest rates of ICU admission. (Supplemental Material Table 4). The data depicting the association of the scoring systems and CT Class with mortality is shown in Supplemental Material Table 3(A) and (B).
Discussion
The use of predictive systems in outcomes is increasingly in vogue in urology. CROES, STONE, and GUYS to predict stone free rate, the RENAL, PADUA, C-index, CSA in kidney cancer and the Partin’s nomogram in prostate cancer.24–28 These nomograms are based on big data to predict outcome and offer guidance in medical management in specific situations.
Emphysematous pyelonephritis (EPN) is an acute, severe necrotizing, often polymicrobial gas-forming infection affecting the renal parenchyma, the collecting system, and perirenal tissue.1–3,29,30 High mortality rates of up to 78% half a century ago was due to poor recognition by virtue of its rarity. This often led to early nephrectomy, which was then the treatment of choice.
A heightened index of suspicion, coupled with early cross-sectional imaging has permitted an algorithmic comprehensive management of EPN comprising of aggressive resuscitation, appropriate antibiotic therapy and the correction of any reversible precipitating factors, along with percutaneous or endourological decompression, as indicated.4–7 Nephrectomy, emergent or elective, is now relegated to a last option. These advances have decreased mortality rates to 18%, with improved renal salvage rates and overall patient outcomes. 6
With the progress made in earlier diagnosis and more effective medical and minimally invasive treatment of EPN, one avenue for improvement in the treatment of EPN remains, and that is the timely institution of ICU management. It is well documented that delays in admitting patients requiring ICU care is associated with higher mortality rates. 31 Objective criteria to assess and predict an EPN patient’s need for ICU admission has, however, yet to be established. General guidelines for admission to the ICU are available from the Society of Critical Care Medicine, 32 though these recommendations are highly dependent on clinical expertise and experience. Existing scoring systems such as NEWS, SOFA, qSOFA, and SIRS are not disease-specific and a consensus is yet to be reached on their appropriate clinical use.12–16
Kapoor et al. 7 found altered mental status, thrombocytopenia, renal failure, and severe hyponatremia, at presentation, to be significantly associated with higher mortality. They did not find any association with the radiological classification. They reported higher renal salvage (22/24, 92%) with minimally invasive treatment. These findings were further corroborated by the study by Aswthaman et al. 4
Falagas et al. 8 reported a meta-analysis of 7 studies (175 patients) to assess the risk factors for mortality in EPN. The overall mean mortality rate was 25%. Conservative treatment alone, bilateral EPN, Wan type 1 EPN and thrombocytopenia all had higher mortality. In addition, altered consciousness, systolic blood pressure of < 90 mmHg, and a serum creatinine > 2.5 mg/dL also contributed to mortality.
Recently, more attempts have been made to improve the prediction of clinical outcomes of EPN patients by combining the variables used previously, in formulating EPN-specific-scoring systems. The novel prognostic scoring systems described by Prakash et al., 9 and Jain et al. 10 however focus mainly on predicting the associated mortality rates and the need for nephrectomy, but are of limited sample size, and remain to be validated. Krishnamoorthy S et al. has provided another elaborate risk stratification protocol using eighteen variables including clinical, biochemical, hematological, and radiological findings to better predict prognosis. This too focused more on mortality rates and was not externally validated. 11
The present work in this large cohort of patients with EPN attempts to identify the best approach to evaluating and triaging these critically sick patients, to expedite their care using MEWS, NEWS, SOFA, qSOFA and SIRS. In our study, all the predictive clinical scoring systems performed well, each achieving AUC > 0.7. NEWS was best at predicting the need for ICU admission. CT Class neither had an independent predictive power, nor did it add significantly to improvement in most of the early warning scoring systems. We may therefore safely conclude that for EPN we can best use the NEWS to evaluate the level of severity and need to ICU admission.
The National Early Warning Score (NEWS2) was developed by the Royal College of Physicians to improve the detection of and response to clinical deterioration in patients with acute illness, especially sepsis. NEWS is based on a simple aggregate scoring system in which a score is allocated to physiological measurements. A NEW score of 5 or more is the key trigger threshold for urgent clinical review and action. 13
The early warning scores have demonstrated varying sensitivities and specificities in the early detection of organ dysfunction, sepsis, and in-hospital mortality.17–22 They expedite the care of critically ill patients with EPN who present with varying degrees of sepsis and organ dysfunction by virtue of its simplicity and utility to the entire range of treating medical and nursing staff.
While CT scanning can confirm and classify EPN, the present study demonstrated that this does not have strong predictive power for ICU admission. However, CT imaging provides information of the extent and localization of the EPN and helps us to decide on the need for radiological, endourological or surgical intervention.
The limitation of this work is the retrospective nature of the evaluation with data collection during a period covering almost one decade. Also, different critical care professionals were involved using different systems and decision-making policies for evaluating and treating critically sick patients. On the other hand, this is one of the largest data sets available to study the use of different scoring systems in this rare but serious disease.
Conclusion
In our study, a NEWS score ⩾ 5 best predicted the requirement for expedited ICU care, and the mortality rate in EPN, thereby improving patient outcomes. Eight of the nine patients that died had NEWS ⩾ 5. Combination with CT-Class did not significantly further enhance the predictive value of these scoring systems. CT evaluation rather guides us to the need for radiological, endourological or surgical intervention.
More robust, prospectively conducted studies will be required to determine the extent to which aggressive early ICU management translates to reduced mortality rates, along with its financial implications.
Supplemental Material
sj-docx-1-tau-10.1177_17562872221078773 – Supplemental material for Evaluation of early scoring predictors for expedited care in patients with emphysematous pyelonephritis
Supplemental material, sj-docx-1-tau-10.1177_17562872221078773 for Evaluation of early scoring predictors for expedited care in patients with emphysematous pyelonephritis by Arun Chawla, Sunil Pillai Bhaskara, Ravi Taori, Jean J.M.C.H de la Rosette, Pilar Laguna, Akhilesh Pandey, Sitaram Mummalaneni, Padmaraj Hegde, Shwetapriya Rao and Prakashini K in Therapeutic Advances in Urology
Supplemental Material
sj-docx-2-tau-10.1177_17562872221078773 – Supplemental material for Evaluation of early scoring predictors for expedited care in patients with emphysematous pyelonephritis
Supplemental material, sj-docx-2-tau-10.1177_17562872221078773 for Evaluation of early scoring predictors for expedited care in patients with emphysematous pyelonephritis by Arun Chawla, Sunil Pillai Bhaskara, Ravi Taori, Jean J.M.C.H de la Rosette, Pilar Laguna, Akhilesh Pandey, Sitaram Mummalaneni, Padmaraj Hegde, Shwetapriya Rao and Prakashini K in Therapeutic Advances in Urology
Supplemental Material
sj-docx-3-tau-10.1177_17562872221078773 – Supplemental material for Evaluation of early scoring predictors for expedited care in patients with emphysematous pyelonephritis
Supplemental material, sj-docx-3-tau-10.1177_17562872221078773 for Evaluation of early scoring predictors for expedited care in patients with emphysematous pyelonephritis by Arun Chawla, Sunil Pillai Bhaskara, Ravi Taori, Jean J.M.C.H de la Rosette, Pilar Laguna, Akhilesh Pandey, Sitaram Mummalaneni, Padmaraj Hegde, Shwetapriya Rao and Prakashini K in Therapeutic Advances in Urology
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Approved by Kasturba Medical College (KMC) and Kasturba Hospital (KH) Institutional Ethics Committee: IEC No: 583-2019. The requirement for written Informed Consent was waived by the approving ethics committee as this was a retrospective study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.