
Abstract
Objective
To determine the predictive value of C-reactive protein (CRP) plus albumin plus procalcitonin for long-term mortality in patients with infective endocarditis.
Methods
This retrospective study included patients hospitalized with infective endocarditis between February 2008 and December 2021. CRP, procalcitonin, and albumin levels were measured within 24 h of admission and dichotomized as high or low. A CRP plus procalcitonin plus albumin points system (range, 3–6) was generated based on high or low CRP, procalcitonin, and albumin concentrations. Patients were divided into two groups: low-risk (≤4 points) and high-risk (>4 points), according to total score. The primary outcome was defined as all-cause mortality rate at long-term follow-up.
Results
Out of 204 patients in total, the high-risk group (n = 29) had higher procalcitonin and CRP levels versus the low-risk group (n = 175), but lower albumin level versus the low-risk group (2.7 ± 0.5 versus 3.5 ± 0.6 g/dl). Matching based on propensity scores showed a higher mortality rate in high-risk versus low-risk patients (76% versus 44%, respectively). In multivariate analysis after matching, the high-risk group was associated with increased long-term mortality (adjusted hazard ratio 2.87, 95% confidence interval 1.32, 6.26).
Introduction
Infective endocarditis is a serious disease that is associated with high mortality and morbidity rates. 1 Risk factors for poor prognosis include older age, the presence of a prosthetic valve, diabetes mellitus, and other comorbidities. 1 Additionally, the presence of heart failure at the time of hospital admission, peri-annular complications, and infection with Staphylococcus aureus is associated with a worse outcome. 2 Patients with infective endocarditis need to receive prompt and appropriate medical treatment to improve their chances of recovery.
Inflammatory biomarkers, such as white blood cell (WBC) count, C-reactive protein (CRP), and procalcitonin, may provide insight into the underlying biological process and severity of infective endocarditis. The CRP-to-albumin ratio is a newly discovered marker of inflammation that is useful in evaluating and monitoring inflammatory conditions. 3 While there is a fair amount of research on the short-term prognosis of infective endocarditis based on these biomarkers, there are limited data on the long-term impact of these parameters on mortality in patients with infective endocarditis.3–7
Therefore, the present study aimed to investigate the prognostic value of using a combination of procalcitonin, CRP, and albumin as markers in the long-term follow-up of patients with infective endocarditis.
Patients and methods
Study population
This retrospective, single-center study was conducted at Izmir Katip Celebi University, Atatürk Training and Research Hospital in Turkey. All patients who had an episode of infective endocarditis (index episode) at hospital between February 2008 and December 2021, and who had a last follow-up in December 2022, were consecutively enrolled. Patients with hematological disease, chronic liver disease, or missing laboratory data were excluded from the study. The study adhered to the Declaration of Helsinki and was approved by the Medical Ethics Committee of Izmir Katip Çelebi University, Atatürk Training and Research Hospital (Approval No. 28.02.2023/0092). The requirement for informed consent was waived due to the retrospective study design. All patient details were de-identified and the reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 8
Data collection
Patients’ medical records were reviewed to collect information on risk factors for infective endocarditis, clinical features, imaging data, complications, need for surgery, fatal outcome, and discharge status. Blood samples were obtained within 24 h of hospital admission, and before starting antibiotic therapy, to measure inflammatory biomarkers, perform blood cultures, and test antibiotic susceptibility. Patients were managed according to current guidelines and recommendations for the treatment of infective endocarditis.
Definitions
Infective endocarditis was defined based on the modified Duke criteria. 9 Heart failure was defined as a presentation with at least 2 out of 3 of the following: New York Heart Association (NYHA) class III–IV, acute decompensation on chest X-ray or echocardiogram, and new peripheral edema. Stroke was defined as clinical or radiographical abnormalities consistent with acute stroke and included both the clinical presentation during treatment, and surgery-related stroke. Peripheral embolization was diagnosed with clinical findings and nuclear or radiographical imaging abnormalities consistent with embolization, excluding strokes such as skin and eye fundus. Chronic kidney disease (CKD) was defined as an estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2, which was calculated using the Modification of Diet in Renal Disease (MDRD) study formula. 10 Treatment strategies were divided into two groups: medical therapy and combined medical-surgical therapy. The outcome was defined as all-cause mortality at long-term follow-up.
Procalcitonin, CRP, and albumin levels, measured within 24 h of hospital admission, were dichotomized as high or low, and used to generate a risk score system, as follows. A high procalcitonin level was defined as a value in the third tertile (>12.95 ng/L), and a low procalcitonin level was defined as a value in the lower 2 tertiles (≤12.95 ng/L). A high CRP was defined as a value in the third tertile (>165 mg/L), and a low CRP was defined as a value in the lower 2 tertiles (≤165 mg/L). A low albumin level was defined as a value in the first tertile (< 2.93 g/dl) and a high albumin level was defined as a value in the higher 2 tertiles (≥2.93 g/dl). High procalcitonin and CRP values were assigned 2 points each, and low values for these parameters were assigned 1 point. A low albumin value was assigned 2 points, and a high albumin value was assigned 1 point. The sum of points for each patient (total score range, 3–6) was used to assigned each patient to either a low-risk group (score ≤ 4 points) or a high-risk group (score > 4 points). For example, a patient with CRP of 80 mg/L (=1 point), procalcitonin of 14 ng/L (=2 points), and albumin of 2.3 g/dl (=2 points) has a total score of 5, and would be placed in the high-risk group.
Statistical analyses
Continuous variables are presented as mean ± SD or median (interquartile range) and categorical variables are presented as n (%) patient prevalence. Either Student's t-test or Mann–Whitney U-test was used to compare continuous values between the two groups, as appropriate, and χ2-test was used to compare categorical variables. A multiple imputation approach was used to handle missing procalcitonin values before analysis. A propensity score was estimated to create a matched dataset (low-risk versus high-risk) and covariates, including CKD, cancer, hemodialysis, pacemaker, WBC, and eGFR were considered for balance between low-risk and high-risk groups. Univariate and multivariate Cox regression analyses were performed to search for predictors of long-term mortality. Two-sided P-values < 0.05 were considered statistically significant. All statistical analyses were performed with IBM SPSS Statistics software, version 25 (IBM Corp; Armonk, NY, USA) and R software (www.R-project.org).
Power analysis
Considering total mortality rates, the study needed to recruit 12 participants for the high-risk group and 72 participants for the low-risk group, to have 80% power with a 5% type 1 error level. The power of the study increased to 99.2% with the selection of 174 low-risk and 29 high-risk patients with 5% type 1 error level.
Results
Initially, 270 patients with infective endocarditis were included in this study. A total of 57 patients died in the hospital, one patient had hematological disease, two patients had chronic liver disease and six patients had missing data at follow-up. Thus, the final study population comprised 204 patients, divided into two groups based on their risk scores: low-risk group (n = 175) and high-risk group (n = 29). Of these, 25 patients (12.25%) had a missing value for procalcitonin levels. The median follow-up duration for this study population was 3.04 (0.93–7.18) years. Demographic and clinical data for the study population are summarized in Table 1. There were no between-group differences regarding histories of diabetes mellitus or cancer. However, the rate of CKD was higher in the high-risk group than in the low-risk group (16/29 [55%] versus 29/175 [17%], respectively, P < 0.001). Pacemaker infective endocarditis was also more common in the low-risk group compared with high-risk group (48/175 [27%] versus 3/29 [10%], P = 0.049). Treatment strategies were similar between the two groups. The rate of culture-negative infective endocarditis was 77/204 patients (37.7%) overall (27.6% in the high-risk group and 39.4% in the low-risk group).
Baseline characteristics of 204 patients with infective endocarditis assigned to high-risk and low-risk groups according to a procalcitonin plus C-reactive protein plus albumin score system, before matching.

Data presented as mean ± SD or n (%) prevalence.
NS, no statistically significant between-group difference (P > 0.05; Student's t-test, Mann–Whitney U-test, or χ2-test).
Regarding laboratory parameters, CRP, procalcitonin and albumin differed between the two groups (all P < 0.001; Table 2). In addition, WBC count was higher in the high-risk group than in the low-risk group (17.2 [15.4–24.5] versus 13.0 [10.5–17.3], P < 0.001; Table 2).
Laboratory findings of 204 patients with infective endocarditis assigned to high-risk and low-risk groups according to a procalcitonin plus C-reactive protein plus albumin score system, before matching.

Data presented as median (interquartile range) or mean ± SD.
WBC, white blood cell; eGFR, estimated glomerular filtration rate; CRP, c-reactive protein; LVEF, left ventricular ejection fraction; LDL, low-density lipoprotein; HDL, high-density lipoprotein; BMI, body mass index.
NS, no statistically significant between-group difference (P > 0.05; Student's t-test, Mann–Whitney U-test, or χ2-test).
Matching based on propensity scores produced 25 patients in each group (Table 3 and 4) and showed a high mortality rate in the high-risk group (19/25 [76%] versus 11/25 [44%], P = 0.021; Table 3 and Figure 1). Kaplan-Meier event-free survival curves showed that patients in the high-risk group had a lower survival rate compared with those in the low-risk group (Figure 2). The cumulative incidence of long-term mortality according to patients’ risk group is presented in Figure 3. In a multivariate analysis of the matched patients, the high-risk group was associated with higher long-term mortality (hazard ratio [HR] 2.87, 95% confidence interval [CI] 1.32, 6.26; P = 0.008; Figure 4). Age was also found to be an independent predictor of mortality (HR –1.04, 95% CI 1.01, 1.07; P = 0.005; Figure 4).
Baseline characteristics of 50 patients with infective endocarditis assigned to high-risk and low-risk groups according to a procalcitonin plus C-reactive protein plus albumin score system, after matching.

Data presented as mean ± SD or n (%) prevalence.
NS, no statistically significant between-group difference (P > 0.05; Student's t-test, Mann–Whitney U-test, or χ2-test).
Laboratory findings in 50 patients with infective endocarditis assigned to high-risk and low-risk groups according to a procalcitonin plus C-reactive protein plus albumin score system, after matching.

Data presented as median (interquartile range) or mean ± SD.
WBC, white blood cell; eGFR, estimated glomerular filtration rate; CRP, c-reactive protein; LVEF, left ventricular ejection fraction; LDL, low-density lipoprotein; HDL, high-density lipoprotein; BMI, body mass index.
NS, no statistically significant between-group difference (P > 0.05; Student's t-test, Mann–Whitney U-test, or χ2-test).

Long-term mortality rates in 50 patients with infective endocarditis assigned to high-risk and low-risk groups according to a procalcitonin plus C-reactive protein plus albumin score system.

Kaplan-Meier event-free survival curves for 50 patients with infective endocarditis assigned to high-risk and low-risk groups according to a procalcitonin plus C-reactive protein plus albumin score system.
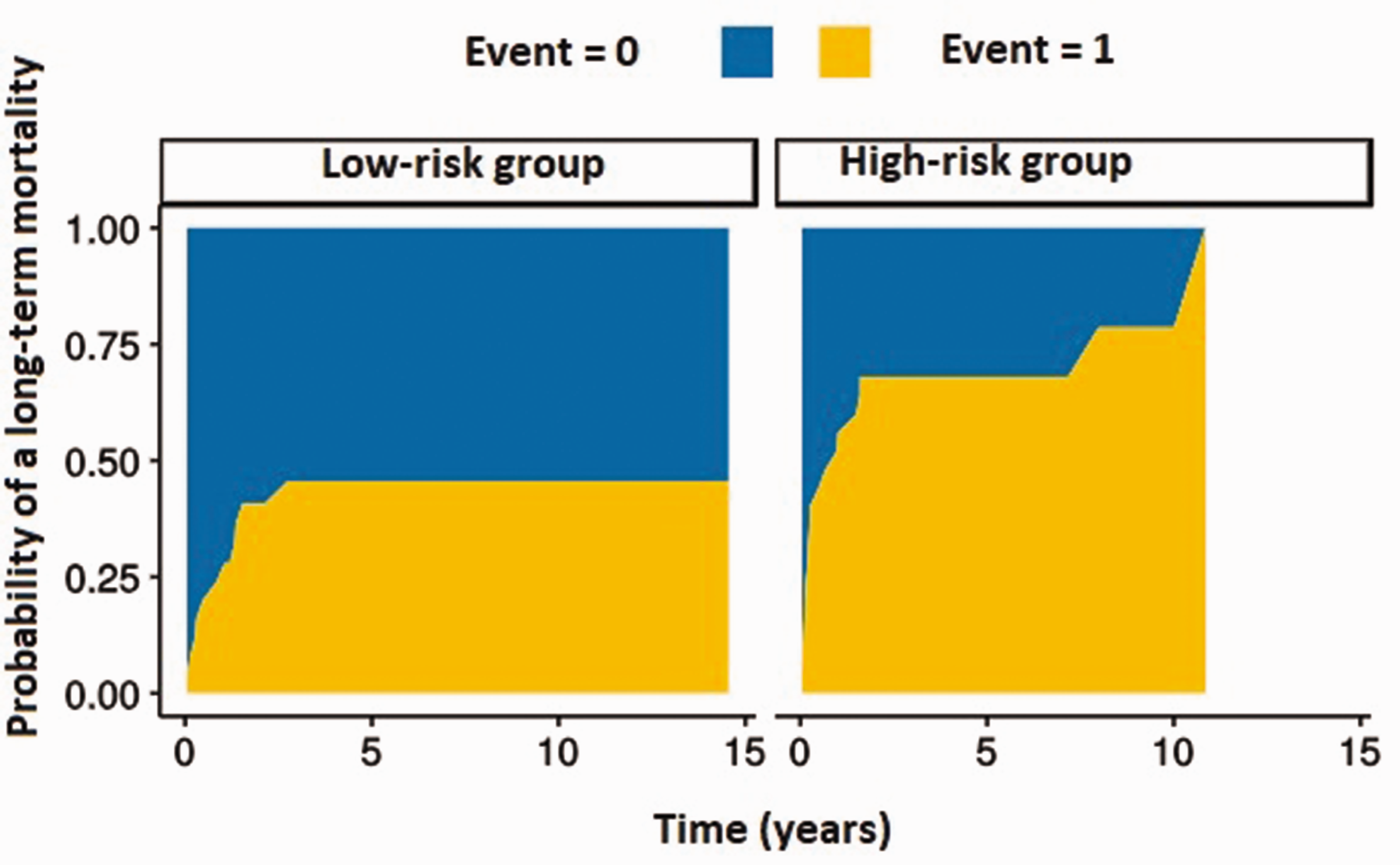
Cumulative incidence of long-term mortality in 50 patients with infective endocarditis assigned to high-risk and low-risk groups according to a procalcitonin plus C-reactive protein plus albumin score system.
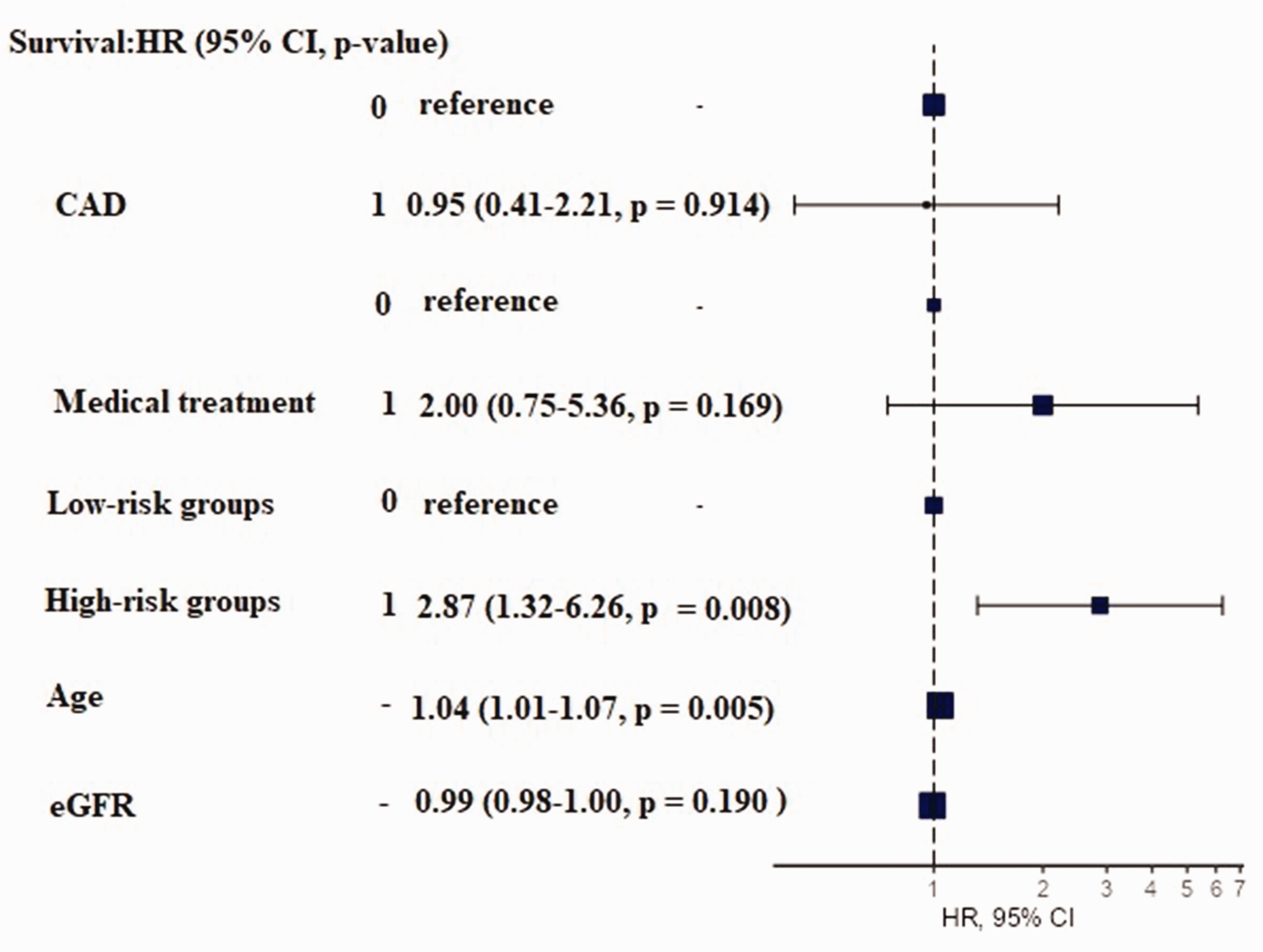
Long-term mortality predictors in 50 matched patients with infective endocarditis assigned to high-risk and low-risk groups according to a procalcitonin plus C-reactive protein plus albumin score system. HR, hazard ratio; CI, confidence interval; CAD, coronary artery disease; eGFR, estimated glomerular filtration rate.
Discussion
To the best of our knowledge, there are no previously published data on the combined impact of procalcitonin, CRP and albumin on long-term mortality in patients with infective endocarditis. In the present study, these combined parameters were found to be independent predictors of long-term mortality in patients with infective endocarditis. In the present study population, as levels of CRP and procalcitonin increased, the albumin level was found to decrease, and the mortality rate increased. The authors conclude that procalcitonin, CRP and albumin combined may be used to predict mortality risk in patients with infective endocarditis.
Inflammation plays a central role in the infective endocarditis process. Procalcitonin is a useful biomarker in the diagnosis of clinically significant infection and sepsis, particularly in the context of infective endocarditis, and its diagnostic value in predicting Staphylococcus aureus as a causative microorganism in patients with infective endocarditis has been shown in previous studies.3–5,7 Studies have found that procalcitonin is associated with in-hospital mortality in patients with infective endocarditis,5,7 and the combined use of procalcitonin with other inflammatory biomarkers, such as WBC and CRP can improve the accuracy of predicting in-hospital mortality. 7 There are no previously published data on the impact of procalcitonin on long-term mortality in patients with infective endocarditis, but in the present study, procalcitonin, combined with CRP and albumin, was found to predict long-term mortality in this patient group.
C-reactive protein is produced by the liver in response to inflammation, and is commonly used as a marker of inflammation.11,12 Elevated CRP levels have been associated with increased mortality and poor outcomes in patients with infective endocarditis, but there are limited data on the prognostic significance of CRP in these patients.5–7,13 CRP levels, measured at the time of admission, during the first week of treatment, and preoperatively, are shown to be associated with increased in-hospital, 30-day, and long-term mortality in patients with infective endocarditis. 6 Similarly, admission CRP, combined with procalcitonin and albumin, was shown to predict long-term mortality in patients with infective endocarditis in the present study.
Albumin is an acute-phase protein that plays important roles, such as anti-inflammatory, antioxidant, and anti-platelet functions,14,15 and low levels of albumin are associated with the development of inflammatory conditions and malnutrition.16,17 Increased inflammation can decrease albumin synthesis and increase catabolism, 18 which may affect its prognostic utility. 19 Albumin also promotes the formation of anti-inflammatory mediators, such as lipoxins, resolvins, and protectins.18,20 Low albumin levels are associated with increased mortality in critically ill patients, particularly those who have infective endocarditis. 3 The present study also found that albumin, combined with CRP and procalcitonin, was a predictor of long-term mortality.
The present study results suggest that using a combination of procalcitonin, albumin, and CRP may provide an accurate assessment of a patient's inflammatory and nutritional status in cases of infective endocarditis compared with using any one marker alone. The CRP-to-albumin ratio is associated with increased in-hospital mortality in patients with infective endocarditis, and high levels of inflammatory biomarkers on admission have been linked to a higher risk of in-hospital mortality in these patients.3,7 Additionally, the combination of CRP and albumin has also been associated with 90-day mortality in patients with systemic lupus erythematosus with serious infections. 21 The present study also showed that a combination of procalcitonin, CRP, and albumin was associated with long-term mortality in patients with infective endocarditis.
In the present study, a 1-year mortality rate of 22% and 5-year mortality of 44.6% was shown, which was similar to those reported by a previous study (1-year mortality of 22.7% and 5-year mortality of 37.5%). 22 In a study published by Tahon et al., 23 the 1-year and 5-year mortality rates were found to be 28.9% and 44.8%, respectively, and the 1-year survival rate in the ESC-EORP EURO-ENDO registry was reported as 23.1%, 24 which were also similar to the present study. Medical treatment without surgery has been associated with high 1-year mortality in patients with infective endocarditis.10,24 However, in the present study, medical treatment alone was not found to be significantly associated with long-term mortality in multivariable analysis. Culture-negative infective endocarditis has been shown to be associated with higher long-term mortality in patients treated with medical therapy alone. 24 The rate of culture-negative infective endocarditis was higher compared with the previous report (37.7% overall versus 16.8%). 24 Age is reported to be an independent risk factor for long-term mortality in patients with infective endocarditis. 10 Similarly, age was found to be related to mortality in the present study.
The present study results may be limited by several factors. First, the study was conducted at a single center with a relatively small number of patients, which may not be generalized to other populations. The retrospective study design may have led to selection bias. Additionally, the study only used a single baseline measurement of biomarkers, which may not have fully captured the dynamic nature of the disease, and patients may not have been at the same stage of infection when the biomarkers were measured. Finally, the study did not standardize antibiotic and surgical therapy approaches, which may have confounded the results. Thus, multicenter studies are needed to validate the present findings.
Infective endocarditis is related to severe complications and high mortality; however, knowledge of the predictive factors for prognosis, including short-term and long-term mortality of infective endocarditis, remains poor. High-risk patients in the present study displayed a high long-term mortality rate. Future studies need to be larger and focus on the mechanism behind the reduced long-term survival in high-risk patients with infective endocarditis. Only new and high-quality evidence will let us establish accurate and reliable clinical practice guidelines for infective endocarditis management.
Conclusion
The presented study found that a high score for combined procalcitonin, CRP, and albumin was associated with poor prognosis in patients with infective endocarditis at long-term follow-up.
Supplemental Material
sj-xlsx-1-imr-10.1177_03000605231208910 - Supplemental material for Combining C-reactive protein, procalcitonin, and serum albumin to predict long-term mortality in patients with infective endocarditis
Supplemental material, sj-xlsx-1-imr-10.1177_03000605231208910 for Combining C-reactive protein, procalcitonin, and serum albumin to predict long-term mortality in patients with infective endocarditis by Banu Karaca, Fatma Esin, Muhammet Mücahit Tiryaki, Gökhun Akkan and Tuncay Kiris in Journal of International Medical Research
Supplemental Material
sj-xlsx-2-imr-10.1177_03000605231208910 - Supplemental material for Combining C-reactive protein, procalcitonin, and serum albumin to predict long-term mortality in patients with infective endocarditis
Supplemental material, sj-xlsx-2-imr-10.1177_03000605231208910 for Combining C-reactive protein, procalcitonin, and serum albumin to predict long-term mortality in patients with infective endocarditis by Banu Karaca, Fatma Esin, Muhammet Mücahit Tiryaki, Gökhun Akkan and Tuncay Kiris in Journal of International Medical Research
Footnotes
Author contributions
All authors contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by BK, TK, FE, and MMT. The primary draft of the manuscript was written by BK, TK, and FE. Writing-review and editing of the final version of the manuscript were carried out by TK, FE, GA, and MMT. BK added critical points to the study. All authors read and approved the final manuscript.
Data accessibility
The data supporting this study's findings have been added as supplementary material
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.