
Abstract
Pulmonary lymphangioleiomyomatosis (LAM), a rare, progressive disease predominantly affecting the lungs of women of reproductive age, is often associated with renal angiomyolipoma (AML). We report the case of a 29-year-old female patient who presented to our obstetrics department at 37 weeks’ gestation, complaining of abdominal pain, and constipation. Ultrasound noted a viable singleton with a large left-sided abdominal mass. After undergoing a caesarean section, she was referred to our urology department to assess her flank mass further. Computed tomography demonstrated a large, exophytic left renal mass measuring 22 cm x 16 cm x 13 cm, suggestive of an AML and numerous bilateral pulmonary cysts. A diagnosis of LAM and associated unilateral giant renal AML was made. As soon as she had fully recovered from her caesarean section, we removed the huge AML via a standard left-sided open nephrectomy without incident. We report this rare case of giant AML associated with LAM and review the literature about the association of these two conditions.
Keywords
Introduction
Pulmonary lymphangioleiomyomatosis (LAM) is a rare, progressive, systemic disease of unknown aetiology, predominantly affecting women of reproductive age. 1 The proliferation of abnormal, smooth muscle-like LAM cells in the lung results in degenerative cystic changes within pulmonary tissue. 2 Although LAM itself is a rare condition, it is often associated with renal AML. We report a case of a 29-year-old lady with LAM and an associated giant AML and review the literature about the association of these two conditions.
Case presentation
A 29-year-old female arrived unbooked at our obstetric department at 37 weeks of gestation, complaining of severe constipation and abdominal pain. Ultrasound noted a viable singleton mature foetus in the breech position and a large left-sided flank mass of uncertain origin. Cardiotocography revealed no abnormality, and informed consent was obtained for a caesarean section. Her postoperative course proved uneventful, and she was referred to our urology department to investigate her flank mass further. Her medical history was unremarkable, and she claimed to have felt so throughout her pregnancy. Vital signs were normal, while abdominal examination noted a large, firm, smooth flank mass extending across the midline and caudally beyond the umbilicus. Routine serum analysis found her haemoglobin, white cell count, and platelet count normal and noted normal renal function.
Computed tomography (CT) confirmed the presence of a large, exophytic mass measuring 22 cm x 16 cm x 13 cm arising from the left kidney, with features characteristic of an angiomyolipoma (Figure 1), and noted a normal right kidney and incidentally, numerous bilateral pulmonary cysts. No pneumothorax or suggestion of chylothorax was evident (Figure 2). The CT findings were suggestive of tuberous sclerosis complex (TSC), but a detailed physical examination, fundoscopy, magnetic resonance imaging (MRI) of the brain and cardiac echocardiography failed to reveal a third feature that would have confirmed a diagnosis of TSC. A diagnosis of LAM with an associated large left-sided renal AML was made.

Coronal (a) and axial (b) computed tomography view of the abdomen demonstrating a large angiomyolipoma of the left kidney with a large intratumoural aneurysm within.
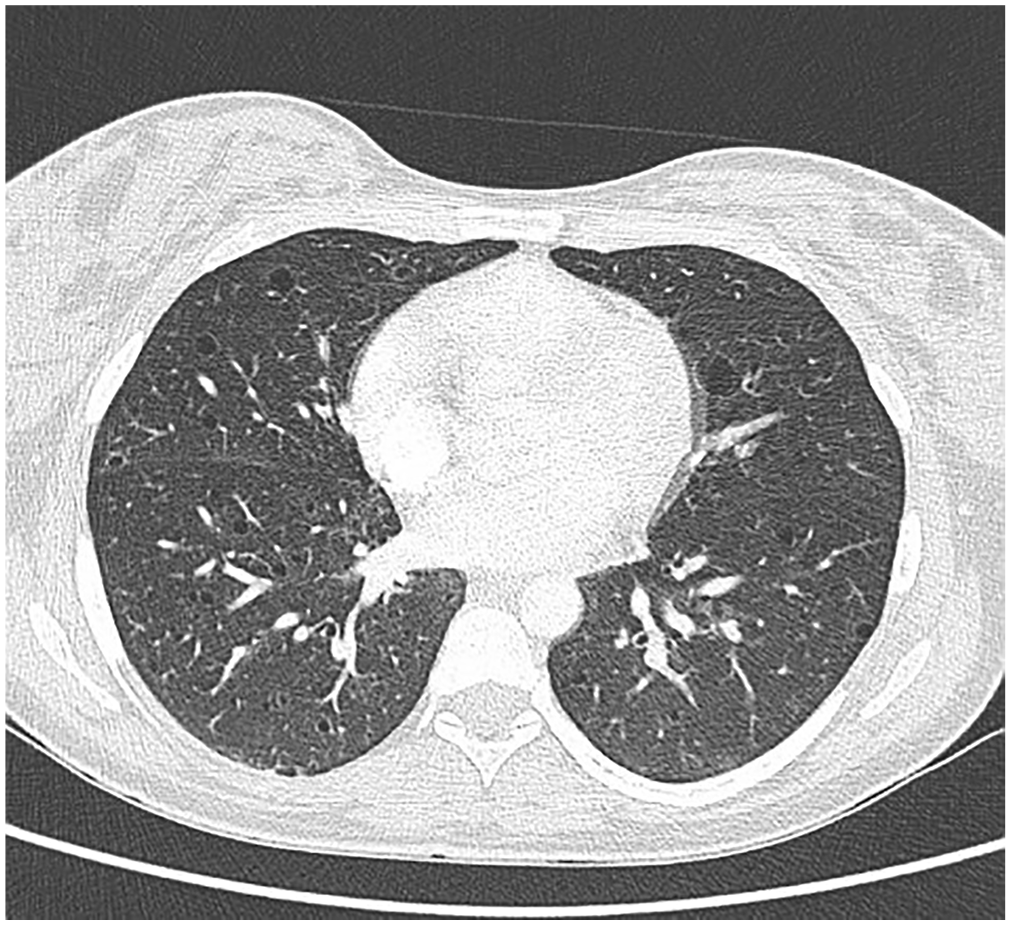
Computed tomography of the chest showing numerous thin-walled, smooth, round pulmonary cysts of varying sizes across both lung fields.
Although our patient had remained asymptomatic throughout her pregnancy, the risk of sudden haemorrhage from her huge left-sided AML remained ever-present. Therefore, as soon as she had recovered from her caesarean section, informed consent was obtained to proceed to a left nephrectomy which was subsequently performed via an anterior subcostal approach.
Macroscopically, a large encapsulated tumour measuring 20 cm x 16 cm x 9 cm was seen arising from the lower pole of the left kidney (Figure 3). The weight of the specimen was 1680 g. The cut surface of the tumour was predominantly fatty (90%). Scattered small ectatic vessels associated with pale nodules were scattered throughout. Microscopic examination confirmed the classic triphasic morphology of an angiomyolipoma (Figure 4). Spindled, cytologically bland myoid cells were arranged haphazardly and in short fascicles with admixed mature adipose tissue. Medium-sized tortuous vessels with thick muscular coats were haphazardly scattered throughout the tumour. In areas, the spindled cells appeared to radiate off the abnormal vessels. There was a minor epithelioid component comprising < 20% of the tumour volume. No features suggestive of the epithelioid variant of AML was identified, and no significant cytonuclear atypia, increased mitotic activity or necrosis was detected. Our patient’s postoperative course proved uneventful. She was discharged on the fourth day and remained well and asymptomatic at follow-up four weeks later. It was arranged that her pulmonary status continues to be monitored by our cardiothoracic colleagues.
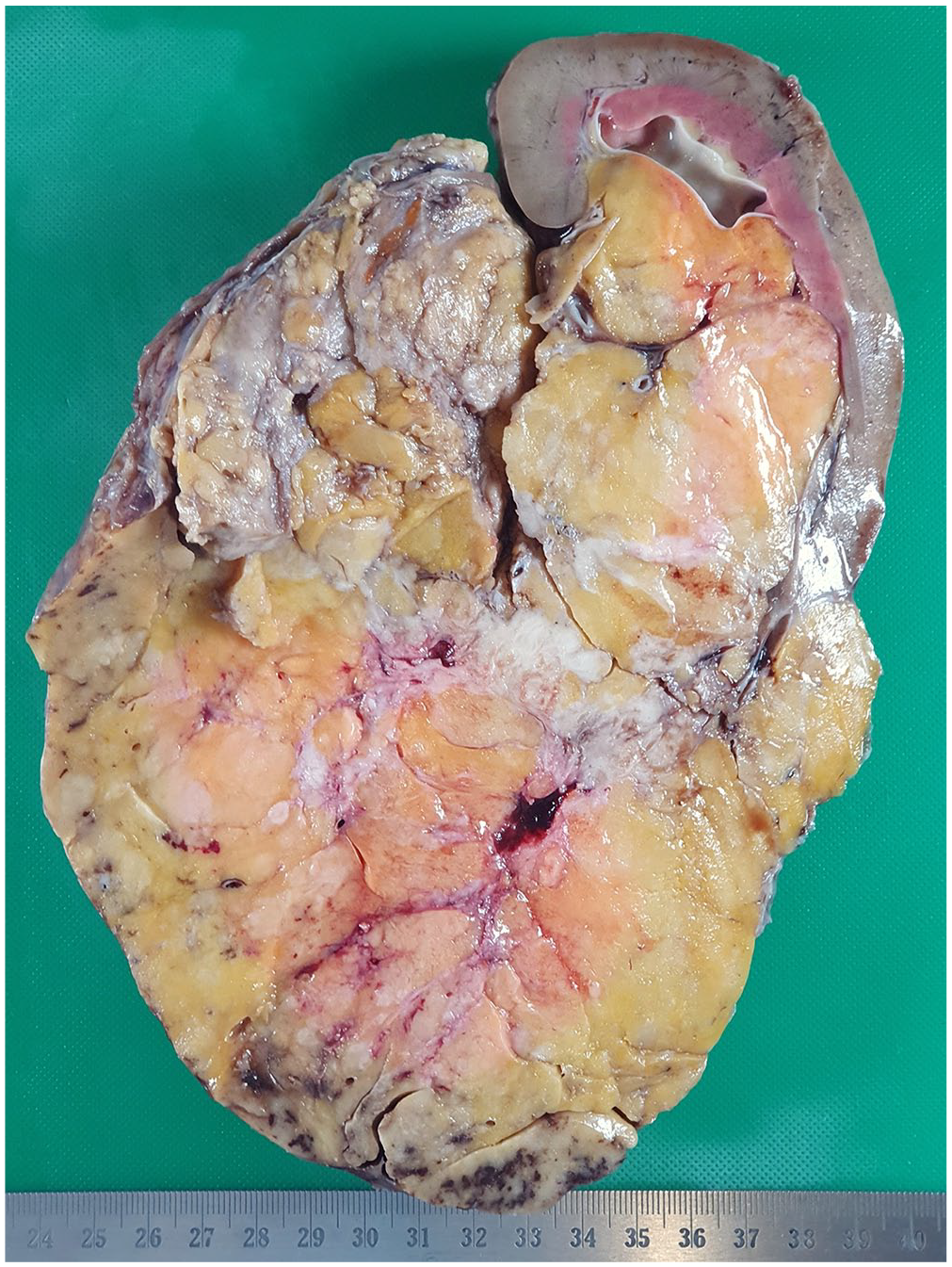
Cut section demonstrated a large circumscribed lower pole tumour involving the renal sinus. The predominant component was fat, with small paler areas representing muscle scattered through.
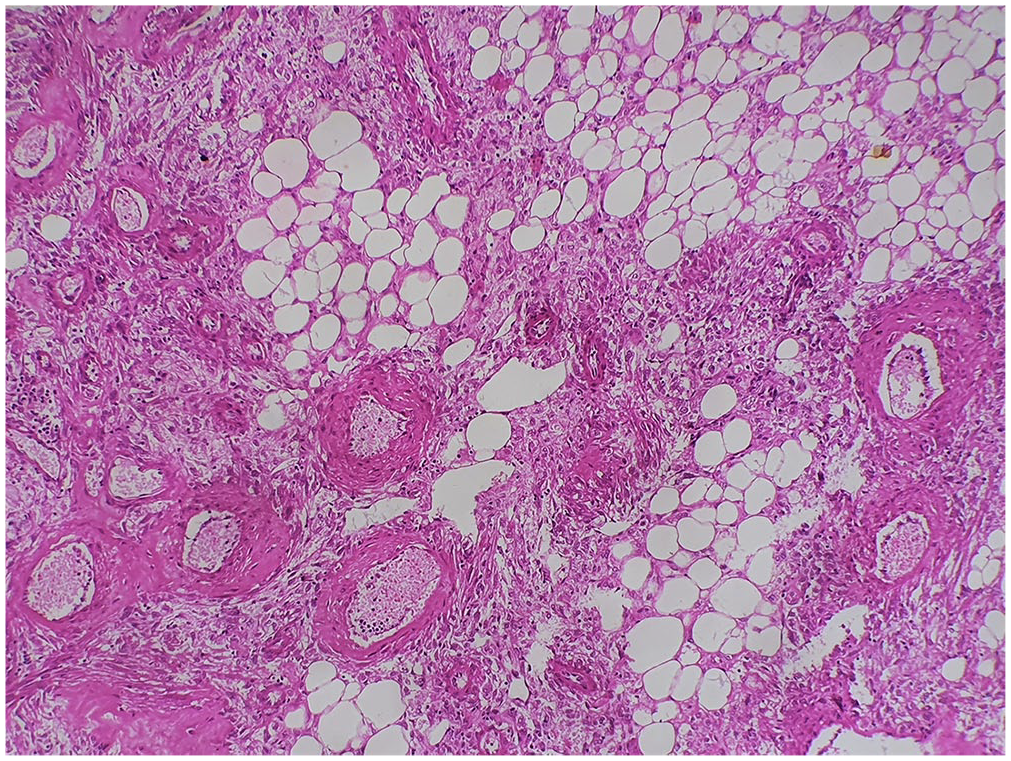
Histology showed the classic triphasic appearance comprising abnormal blood vessels with radiating epithelioid to spindled myoid cells and interspersed fat (H&E, x 100).
Discussion
Renal AML is an uncommon benign mesenchymal tumour with a reported incidence varying between 0.02% and 0.3% in patients without tuberosclerosis complex. 3 The majority (80%) of cases are isolated and occur sporadically, most commonly occurring in middle-aged women. The remaining 20% of AMLs develop in association with tuberosclerosis complex (TSC) or sporadic pulmonary lymphangioleiomyomatosis (LAM). 4 Although LAM and AML (both major features of TSC) were present in our patient, TSC was excluded under the revised criteria for the clinical diagnosis of TSC, which require that a third clinical feature be present. 5 No such additional feature was found on clinical examination and fundoscopy, and an MRI brain and cardiac echocardiography were normal. The diagnosis of LAM was based on the characteristic CT appearance of multiple bilateral pulmonary cysts in association with the presence of a unilateral left-sided renal AML. Where the diagnosis is less obvious, a transbronchial lung biopsy can help confirm the presence of pulmonary LAM. 6 LAM is a rare, systemic disorder of unknown aetiology, principally affecting women of reproductive age, 1 in which there is a patchy proliferation of abnormal, smooth muscle cells (known as LAM cells) in the pulmonary interstitium and along axial lymphatics of the thorax and abdomen. The prevalence of this rare multisystem disorder is around one per million in the United Kingdom, France, and the United States. 7 Our patient had no LAM symptoms and remained asymptomatic while under our care. Renal AMLs (commonly associated with TSC) are also the commonest extrapulmonary manifestation of LAM in 30% of patients 1 LAM- associated AMLs are usually unilateral and asymptomatic. When symptomatic, patients report a palpable mass, flank pain or haematuria.3,8 As the lesion grows, large lesions may encroach insidiously on the normal renal parenchyma causing renal failure and compress the gastrointestinal tract causing gastrointestinal symptoms. 9 Spontaneous retroperitoneal haemorrhage can be a catastrophic complication of AML, presenting with acute flank pain, a flank mass, and hypovolemic shock (Lenk’s triad.) 10 Our patient factors predisposing to AML rupture included the huge size of her tumour and pregnancy, which is associated with an increased maternal blood volume and elevated intraabdominal pressure. Despite the added risks of rupture of her AML, our patient remained remarkably asymptomatic and incident-free while seeking no medical care during her pregnancy and then undergoing a caesarean section and left nephrectomy in quick succession!
Most renal AMLs are detected incidentally in asymptomatic patients. A conservative approach to management has traditionally been adopted for patients with tumours < 4 cm, but contemporary evidence suggests that this cut off size may result in overtreatment in patients with asymptomatic tumours > 4 cm and intratumoural aneurysm size appears to be a stronger predictor for spontaneous rupture. Yamakado et al. evaluated this relationship between tumour size, aneurysm formation, and spontaneous rupture in renal AMLs. When a tumour size of > 4 cm and aneurysm size of > 5 mm were used as a predictor of rupture, the specificity was reported as 38% and 86% respectively. 11
Therapeutic interventions have been reserved for symptomatic tumours, and every attempt should be made to preserve as much renal tissue as possible by selective arterial embolization or partial nephrectomy. Giant AMLs, however, are best treated by nephrectomy because of the increased risk of rupture and the paucity of renal units available for embolization in the affected kidney.
The pulmonary function has been shown to decline during pregnancy in patients with LAM. Although our patient had no LAM symptoms during her recent pregnancy, we warned her of the risk of potential lung damage during future pregnancies.
The management of LAM symptoms is mainly supportive. Beta-2-agonists will help if there is an airflow obstruction. 7 while patients with recurrent pneumothorax and pleural effusion can be offered pleurodesis. 6 The mammalian target of rapamycin (mTOR) inhibitor, Sirolimus, is the first drug to be approved for the treatment of LAM by the United States Federal Drug Association (FDA) and has been shown to improve pulmonary function, oxygen levels, exercise capacity, and quality of life in patients with LAM. 12 Lung transplantation is an option to be considered for patients with the end-stage pulmonary disease. 6
Conclusion
LAM, a rare chronic systemic disease of unknown aetiology that occurs mainly in young women and primarily affects the lung, is commonly associated with unilateral, solitary AML. Therefore young women who present with a unilateral AML should be screened by high-resolution computed tomography to exclude pulmonary LAM.
The early diagnosis of pulmonary LAM is important because the mTOR inhibitor Sirolimus has been shown to slow down disease progression or improve lung function in symptomatic patients.
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethics approval for reporting individual case reports.
Informed consent
Written informed consent was obtained from the patient for the anonymised information and the accompanying images to be published in this article.