
Abstract
Objective
Pregnant patients with lymphangioleiomyomatosis (LAM) and renal angiomyolipomas (AMLs) require care for both renal AMLs and pulmonary dysfunction because AMLs can grow and rupture during pregnancy, potentially causing hemorrhagic shock and fetal death. This study examined whether prophylactic transcatheter arterial embolization (TAE) could prevent the pregnancy-associated growth and rupture of renal AMLs in patients with LAM.
Methods
This retrospective study included five women with 14 renal AMLs (initial diameter, ≥2 cm) first encountered between September 2010 and August 2015 who subsequently became pregnant. Seven tumors in five patients were embolized, and seven tumors in two patients were not treated. Changes in the volume of each tumor were evaluated.
Results
Untreated tumors were much more likely to grow than embolized tumors both during pregnancy (100% vs. 0%) and at the first follow-up visit after delivery (100% vs. 14%). One untreated hypervascular tumor grew rapidly during pregnancy to 409% of the pretreatment volume. No tumor ruptured.
Conclusions
Prophylactic pre-pregnancy TAE decreased the growth and bleeding of renal AMLs during pregnancy in patients with LAM. TAE can be recommended for hypervascular tumors before pregnancy regardless of the size of the aneurysm.
Introduction
The polycystic lung disease pulmonary lymphangioleiomyomatosis (LAM) occurs in approximately two to five women per million women of childbearing age, and the average age at onset is 30 years. 1 The disease is classified as sporadic LAM (S-LAM), which accounts for 80% of cases, or tuberous sclerosis complex (TSC)-associated LAM (TSC-LAM). 1 TSC is an autosomal dominant disorder characterized by systemic hamartomatous lesions. Patients with LAM often develop renal angiomyolipoma (AML) at a frequency of 85.7% among those with TSC-LAM and 17.4% among those with S-LAM. 2 Approximately 40% of patients with TSC have concurrent LAM, 3 and 40% to 80% of patients with TSC also have AML.4,5
Renal AMLs are hamartomas composed of adipose tissue, smooth muscle tissue, and blood vessels that often cause aneurysms. These lesions are common in 40- to 50-year-old women. Approximately 20% to 30% of renal AMLs occur in patients with TSC. 6 AMLs are more common in younger patients with TSC. In addition, AMLs in patients with TSCs are more frequently bilateral and multiple and they are more likely to rupture and cause bleeding than those in patients with sporadic AML.7–9 If a woman with renal AML becomes pregnant, the tumor may grow, leading to rupture of the intratumoral aneurysm, followed by intratumoral or retroperitoneal bleeding, hemorrhagic shock, and fetal death.10–14
Prophylactic treatment methods to prevent the growth and rupture of renal AMLs include transcatheter arterial embolization (TAE), surgery (partial or total nephrectomy), radiofrequency ablation, and (in cases of TSC-AML and S-LAM-AML) pharmacological treatment with a mammalian target of rapamycin (mTOR) inhibitor. 15 Of these treatment methods, TAE is also the first-line therapy for ruptured renal AMLs and the preferred management strategy for symptomatic tumors or tumors having intratumoral aneurysms with a high risk of rupture (i.e., aneurysms ≥5 mm in diameter).15–17
The technical success rate of TAE was 93.3% with no intraprocedural mortalities or fatal complications. 18 Post-procedural morbidities included non-target embolization (2.3%), respiratory complications (2.0%), abscess formation (1.6%), active retroperitoneal hemorrhage (1.0%), allergic reactions (0.6%), urinary retention (0.6%), urinary tract infections (0.3%), and renal spasm (0.3%). 18
Because of its high technical success rate, TAE is performed for sporadic AML with a good volume shrinkage rate of 77%. 19 However, the recurrence rate after TAE is at least 24% in patients with TSC, and there is a risk of renal dysfunction associated with repeated TAE. Thus, mTOR inhibitors should be the first choice for TSC-related angiomyolipomata. 20 TAE is the first-line therapy for ruptured renal AMLs, and it is also useful as a prophylactic treatment to avoid tumor bleeding.16,21 Case reports illustrated the utility of TAE for treating ruptured renal AMLs during pregnancy or childbirth,10,22,23 but whether pre-pregnancy TAE can prevent the pregnancy-associated growth and rupture of renal AMLs is unclear.
In this retrospective study, we have reported 14 cases of renal AML in five women that were ≥2 cm in diameter. Half of the AMLs were treated with prophylactic TAE before the women became pregnant, whereas the other half were not treated before or after the women became pregnant.
Materials and methods
The reporting of this study conforms to the STROBE guidelines. 24
Patients
The institutional review board of Juntendo University Hospital (Tokyo, Japan) approved this retrospective study (approval number: No. 17-117; approval date: 21 September 2017). However, the need for informed consent was waived, and we have de-identified all patient details. From September 2010 through August 2015, 35 patients with pulmonary LAM were monitored and treated via prophylactic TAE for renal AMLs in our department. All patients were women (mean age, 37 years; range, 21–55 years). After TAE, six patients (three with S-LAM and three with TSC-LAM) became pregnant and gave birth. Of these six patients, one did not undergo magnetic resonance imaging (MRI) during pregnancy, and she underwent her initial post-delivery MRI after mTOR inhibitor therapy. She was therefore excluded from the study. Ultimately, five patients (two with S-LAM and three with TSC-LAM) who underwent computed tomography (CT) or MRI before pregnancy (five patients), during pregnancy (four patients), and after delivery (five patients) were included in the study population. Fourteen tumors that were ≥2 cm in diameter on pre-embolization CT were considered clinically important (Table 1).
Tumor and patient characteristics and follow-up imaging of patients with renal AML.

GM, gestational months; CT, computed tomography; LK, left kidney; MRI, magnetic resonance imaging; RK, right kidney; S-LAM, sporadic lymphangioleiomyomatosis; TAE, transcatheter arterial embolization; T-LAM, tuberous sclerosis complex–associated lymphangioleiomyomatosis.
“Time” indicates the time relative to TAE.
TAE
Before TAE, all five patients underwent dynamic contrast-enhanced CT. The number and size of tumors, intratumoral aneurysm(s), and tumor vascularity were evaluated on the axial images of 5-mm slices. Tumors with aneurysms that were ≥5 mm in diameter underwent TAE in accordance with published guidelines for the management of renal AML with TSC. 17 However, in light of the experience of patient 4, for patient 5, we added a treatment indication for hypervascular renal AMLs that lacked aneurysms ≥5 mm in diameter; that is, tumors 13 and 14 were treated in addition to the tumor with a ≥5-mm aneurysm (no. 12). Finally, although each patient underwent TAE, seven target tumors in five patients were embolized, and seven target tumors in two patients were left untreated (Table 1).
TAE was performed selectively using gelatin sponges alone or together with microcoils for abnormal blood vessels and intratumoral aneurysms. All diagnostic angiography was performed using a 4-F catheter (TRJ; Terumo Co. Ltd., Tokyo, Japan). This was followed by the insertion of a 1.98-F or 1.8-F microcatheter (Masters PARKWAY SOFT Microcatheter; Asahi Intecc Co Ltd, Aichi, Japan) for superselective embolization of the tumor-feeding arteries. Embolization of all tumors and intratumoral aneurysms was performed by injecting 1- or 2-mm-diameter multiporous gelatin sponge particles (GSPs, Gelpart; Nippon Kayaku Co Ltd, Tokyo, Japan). In all procedures, additional various combinations of detachable microcoils (Guglielmi, diameter, 2–12 mm; length, 2–30 cm; Stryker Corp, Kalamazoo, MI, USA), pushable microcoils (Tornado, diameter, 3–5 mm; length, 2 cm; Cook, Inc, Bloomington, IN, USA), straight coils (Hilal, length, 1–2 cm; William Cook Europe ApS, Bjaeverskov, Denmark), or multiple curled Hilal coils (diameter, 2 mm; length, 2 cm; William Cook Europe ApS) were placed in the aneurysms and the distal portions of their feeding arteries after embolization with the sponge particles. After TAE, angiography was performed to confirm the disappearance of intratumoral aneurysms and blood flow in the target tumors. All TAE sessions were completed uneventfully, and no complication excluding post-embolization syndrome occurred.
Follow-up of target tumors
The observation period lasted until the first post-delivery radiological follow-up. The tumors were evaluated by CT or MRI before pregnancy, and the tumors and aneurysms were evaluated during pregnancy and at the first post-delivery follow-up via non-contrast MRI and non-contrast MR angiography using the time–spatial labeling inversion pulse method.
Synapse Vincent Software (Fujifilm, Tokyo, Japan) was used to calculate tumor volumes on CT or MR images. Briefly, axial enhanced CT images or axial T2-weighted MR images were loaded into the software, tumor margins were delineated, and tumor volumes were calculated automatically. For each of the 14 tumors, the volume calculated on CT images obtained before the patient underwent TAE was defined as the original volume. The volume calculated on CT or MRI performed after the patient underwent TAE but before pregnancy was defined as the volume before pregnancy. Tumor volumes during pregnancy and after delivery were also obtained. The volume of each tumor at each follow-up visit was recorded as a percentage relative to its original volume. The courses of treated and untreated tumors were evaluated. If treated tumors grew during post-embolization follow-up, we calculated the regrowth rate as the percentage of volume change relative to the tumor volume at the preceding time point.
Statistical analysis
Continuous data that were normally distributed are presented as the mean ± standard deviation. Data that were not normally distributed are presented as the median and interquartile range. Fisher’s exact test was performed. P < 0.05 (two-sided) was considered statistically significant. Statistical analyses were performed by using PASW Statistics for Windows, version 18.0 (IBM, Armonk, NY, USA).
Genetic counseling
Because TSC is an autosomal dominant disorder, it requires patients to undergo careful genetic counseling regarding pregnancy. In this study, all patients with TSC had mild disease without intellectual impairment. Patients received a sufficient explanation and achieved an understanding of the heritability of the disease before making decisions regarding pregnancy.
Results
At the time of TAE, the mean age of the five women was 35 ± 3 years. For all 14 renal AMLs, the mean tumor volume before TAE was 47.5 mL (range, 20–125 mL). The mean elapsed time from treatment to pregnancy was 22 months (range, 11–47 months). Information about the post-embolization radiological examinations performed before pregnancy, during pregnancy, and after delivery is presented in Table 1.
For the seven embolized tumors, the original volume was 208 ± 186 mL. After embolization, the relative tumor volumes before pregnancy, during pregnancy, and at the first post-delivery follow-up were 52 ± 23% (range, 28%–84%), 45 ± 20% (range, 29%–82%), and 42 ± 24% (range, 14%–84%), respectively. No tumors increased in volume during pregnancy, and only one of the seven treated tumors (14%) had increased in volume at the first follow-up after delivery compared with the tumor volume before pregnancy (Figure 1). No tumor displayed an increase in volume relative to the pre-embolization tumor volume during the observation period (Figure 1). Figure 2 presents the post-embolization follow-up images of one embolized tumor that shrank both during pregnancy and after delivery.

Volumes of seven renal angiomyolipomas subjected to transcatheter arterial embolization before pregnancy. Tumor volume was measured before transcatheter arterial embolization (original), before pregnancy, during pregnancy, and after delivery. Four tumors (nos. 2, 4, 12, and 13) rebounded slowly after shrinking, but none of them regrew to be larger than the pre-embolization volume. The relative volume is the percent tumor volume at the time point of interest relative to the original volume.

Post-embolization follow-up of tumor no. 1 (arrows) in patient 1 with sporadic lymphangioleiomyomatosis. (a) Coronal image from contrast-enhanced computed tomography performed after embolization but before pregnancy. (b) Coronal T2-weighted magnetic resonance image during pregnancy and (c) Coronal T2-weighted magnetic resonance image obtained at the first follow-up after delivery. Compared with its size before pregnancy (relative volume, 47%), the tumor volume was lower both during pregnancy (relative volume, 29%) and after delivery (relative volume, 14%). The relative volume is the percent tumor volume at the time point of interest relative to the original volume.
For the seven untreated tumors, the original mean tumor volume was 22 mL (range, 15–57 mL). The relative tumor volumes before pregnancy, during pregnancy, and at the first post-delivery follow-up were 109 ± 13% (range, 95%–129%), 120% (interquartile range, 102%–409%), and 145 ± 22% (range, 109%–171%), respectively (Figure 3). Follow-up images during pregnancy were available for six tumors, all of which increased in volume. In addition, all seven tumors were larger at the first follow-up after delivery than before pregnancy. In particular, one tumor (no. 6; Figure 4) grew more rapidly during pregnancy (relative volume, 409%) than the other six tumors, for which the relative volumes ranged from 102% to 140% (Figure 2). However, the volume of tumor no. 6 was smaller at the first follow-up after delivery (relative volume, 109%) than during pregnancy (Figure 4). Relative to the volume before pregnancy, tumor volume increases were more frequent among untreated tumors than among treated tumors both during pregnancy (100% vs. 0%, P = 0.002) and at the first follow-up after delivery (100% vs. 14%, P = 0.005).

Volumes of seven untreated renal angiomyolipomas. Tumor volume was measured at baseline (original), before pregnancy, during pregnancy, and after delivery. Tumor no. 6 grew rapidly during pregnancy (relative volume, 409%) and shrank after delivery (relative volume, 109%). The remaining six tumors grew more slowly throughout pregnancy and after delivery. The relative volume is the percent tumor volume at the time point of interest relative to the original volume.
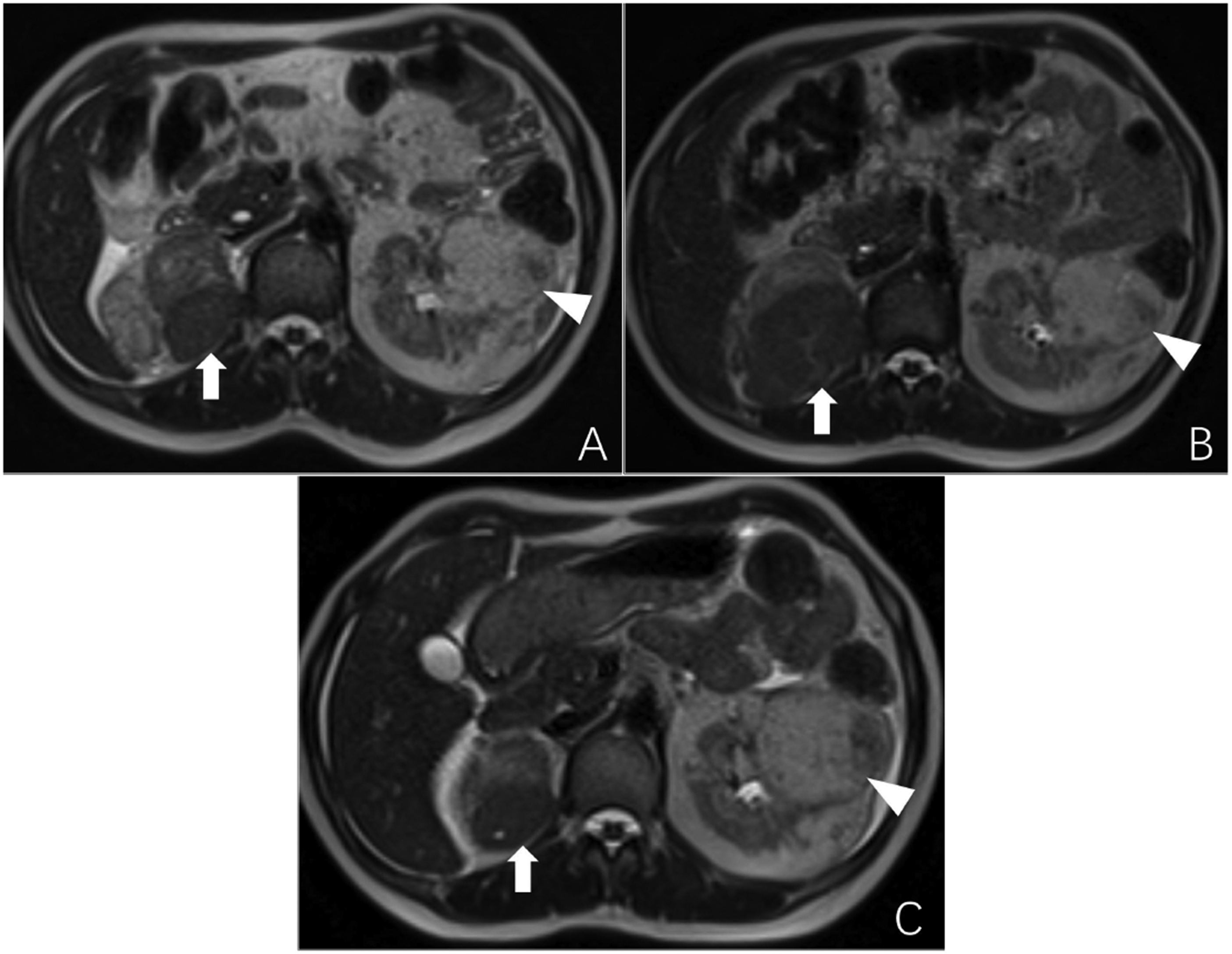
Follow-up of untreated tumors no. 6 (arrows) and no. 9 (arrowheads) in patient 4, who had tuberous sclerosis complex–associated lymphangioleiomyomatosis. Images are axial T2-weighted images from magnetic resonance imaging performed (a) before pregnancy, (b) during pregnancy and (c) at the first follow-up after childbirth. The tumor in the right kidney (no. 6) was rich in muscle tissue on magnetic resonance imaging, and it grew rapidly during pregnancy (relative tumor volume, 409%) and shrank after childbirth (relative volume, 109%). The tumor in the left kidney (no. 9) was rich in fat tissue, and it grew more slowly than tumor no. 6 during pregnancy (relative volume, 114%). The relative volume is the percent tumor volume at the time point of interest, relative to the original volume.
Discussion
Renal AMLs can grow and subsequently rupture during pregnancy. This problem is believed to be associated with several factors, including the increased circulating plasma volume that accompanies pregnancy, pressure from the uterus, elevated blood pressure, estrogen-induced smooth muscle proliferation and positivity for hormonal receptors (estrogen receptor-β; 100%, estrogen receptor-α; 28%, progesterone receptor; 38% and aromatase; 10%).22,25–27 Follow-up observation, emergency TAE, and nephrectomy have been reported as treatments for hemorrhagic renal AMLs in pregnancy, and the choice of treatment varies by case.14,22,28 Prophylactic TAE before pregnancy had not been reported previously, but it appeared likely to be effective for decreasing the risk of tumor growth and rupture during pregnancy.
Among 14 tumors in five women with concurrent S-LAM or TSC-LAM, we performed prophylactic TAE for seven renal AMLs that had intratumoral aneurysms of ≥5 mm in diameter or that were hypervascular. We then monitored the seven treated and seven untreated renal AMLs for changes in size during pregnancy and after delivery. Embolized tumors were significantly less likely than untreated tumors to increase in volume versus pre-pregnancy both during pregnancy (0% vs. 100%) and after delivery (14% vs. 100%). In addition, no embolized tumor regrew to larger than its pre-embolization volume. Furthermore, no treated tumors ruptured through pregnancy, and all patients gave birth without problems. Therefore, we consider TAE effective as a prophylactic treatment for renal AMLs to slow or prevent tumor growth and rupture during pregnancy.
A comparison of tumor volumes before or during pregnancy and after delivery revealed that four treated tumors (nos. 2, 4, 12, and 13; Figure 1) regrew after delivery (range of regrowth, 2%–17%). Three of these tumors were in patients who had concurrent TSC-LAM (Table 1). The underlying reason for this regrowth may have been the abundant blood flow in AMLs associated with TSC-LAM. These increases in tumor volume were small compared with the pre-embolization tumor volume, and they did not appear to cause serious clinical problems.
Multiporous GSPs (followed by metallic coils in all cases) were used for tumor vessel embolization. Among the many embolic agents, multiporous GSPs yield the lowest complication rates when used in renal tumor embolization.29,30 Multiporous GSPs in pure contrast materials are easily recognized fluoroscopically during superselective embolization because there is no dilution of the contrast materials. Therefore, reflux of particles into the normal renal parenchyma (non-target embolization) can be avoided, and treatment can be achieved without renal dysfunction. Multiporous GSPs produce embolization results similar to those produced by other embolic agents such as microspheres and ethanol.
Patient 4 had seven renal AMLs that affected both kidneys (Table 1). Two of these tumors (nos. 5 and 6) were hypervascular with multiple aneurysms on pre-embolization contrast-enhanced CT. In accordance with the guidelines, 17 we performed TAE only for tumor no. 5, which had an aneurysm of ≥5 mm in diameter. Despite its high vascularity and abundant small arteries on renal angiography, tumor no. 6 was not embolized because of its small size and the lack of an aneurysm ≥5 mm in diameter. During pregnancy, the treated tumor (no. 5) shrank (relative volume, 36%); in contrast, the untreated tumor (no. 6) grew exuberantly during pregnancy (relative volume, 409%) but shrank again (to 109% of post-embolization volume) after delivery (Figures 2 and 4). This tumor contained almost no fat on MRI and CT, but it had a rich blood flow on contrast-enhanced CT and angiography. The increase in tumor blood flow during pregnancy was likely responsible for the increase in the size of the mass, and we infer that lesions with copious blood flow and well-developed abnormal blood vessels are likely to grow markedly and rapidly during pregnancy.
As we mentioned previously, patients with TSC often have multiple renal AMLs that tend to grow, indicating that the presence of TSC is a risk factor for tumor enlargement during pregnancy. In light of the experience with patient 4, in patient 5 (who also had TSC-LAM), we treated two hypervascular tumors (nos. 13 and 14) that had many tumor vessels but no intratumoral aneurysms. Consequently, both of these tumors decreased in volume during pregnancy, and safe delivery was achieved.
Our results suggest that hypervascular tumors are likely to grow during pregnancy and shrink after delivery and that prophylactic TAE of these tumors can prevent tumor growth and rupture and thus ensure safe delivery. Therefore, prophylactic TAE may be recommended for all hypervascular tumors in women considering pregnancy regardless of the size of the aneurysm. In this study, we were unable to compare renal AMLs between S-LAM and TSC-LAM because of the small sample size. However, because AMLs have a stronger tendency to grow and to develop intratumoral abnormal blood vessels in patients with TSC than in patients without TSC,7–9 we believe that renal AMLs in patients with TSC require increased attention and potentially require more frequent follow-up.
Cases of pregnancy with ruptured renal AMLs are uncommon. However, pregnancy in individuals whose AML is not followed is dangerous because potential rupture of a renal AML can increase the risk of both maternal and fetal death. Therefore, physicians caring for female patients who are in their reproductive years and who have renal AML should ask these patients about their pregnancy and delivery plans to ensure that treatments maximize the likelihood of safe delivery. Few of the case reports on the embolotherapy of renal AMLs that have ruptured during pregnancy included patients with TSC,10–14 likely because few reports overall have been published, few patients have been diagnosed with TSC, and some patients with TSC have not been diagnosed. Moreover, few patients with TSC become pregnant.
The limitations of the current study include the small number of cases and the brief follow-up period. Future studies and randomized trials will require more patients and longer follow-up periods.
In conclusion, for patients with concurrent TSC-LAM or S-LAM, TAE is a useful treatment method to prevent renal AMLs from growing and potentially rupturing during pregnancy. Because hypervascular tumors may be particularly likely to grow during pregnancy, prophylactic TAE should be recommended to all hypervascular tumors regardless of size.
Footnotes
Acknowledgement
We thank Mao Hayashi for editing a draft of the manuscript.
Author contributions
RK and KS contributed to the study conception and design. XZ and YK conducted the statistical analyses. HT and DY contributed to manuscript writing. All authors contributed to data interpretation, revised the manuscript critically for important intellectual content, and approved the final version of the manuscript for submission.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.