
Abstract
Cytomegalovirus (CMV), an AIDS defining disease, has a high seroprevalence in the general population, while symptomatic infections occur mostly in immunocompromised individuals. Symptomatic CMV infections commonly include pneumonia, encephalitis, retinitis and colitis, while urinary tract involvement is a rare entity. We present a rare case of massive macroscopic haematuria due to CMV haemorrhagic cystitis in a 29-year-old woman in her second trimester of pregnancy. She was treated with intravenous Ganciclovir after initial resuscitation, and her symptoms promptly resolved. Timely diagnosis and treatment of symptomatic CMV infection is necessary to prevent associated morbidity, and this is especially significant during pregnancy in order to prevent foetal transmission. Both our patient and her baby remained symptom free at the 6-month follow-up post-delivery. Clinicians should have a high index of suspicion to biopsy the bladder urothelium of at-risk patients who present with haemorrhagic cystitis and have non-specific cystoscopy findings as histopathological analysis is the mainstay of diagnosing CMV-cystitis.
Introduction
Human cytomegalovirus (CMV) constitutes one of the members of the β-herpes virus subgroups and is one of the largest human herpesviruses at 230 kb, with a double-stranded DNA viral structure. 1 CMV is a common viral pathogen with an estimated seroprevalence of 45–100% in the general population. 2 The severity of the disease caused by the pathogen is usually determined by the host’s immune status. It ranges from being largely benign in the immunocompetent host to causing significant morbidity and mortality in immunocompromised patients. Immunosuppressed haemopoietic cell transplant or solid organ transplant recipients and individuals with severe HIV/AIDS (CD4+ count < 50 cells/mm3; HIV viral load > 100,000 copies/ml) are most at risk. The introduction of antiretroviral therapy has seen a significant decline in active CMV disease in the HIV/AIDS population. 1 After the primary infection, the virus remains latent in most cases. 3 However, significant mortality and morbidity associated with pneumonia, encephalitis, retinitis, myocarditis, gastritis, oesophagitis or colitis may ensue in the immunocompromised patient. 4 While ocular, gastrointestinal and neurological manifestations of CMV are well documented, urinary tract involvement, such as cystitis, is rare and has mainly been limited to isolated case reports. CMV infection during pregnancy brings with it another dimension where two individuals could be affected with the possibility of transplacental transmission from the mother to the foetus.
We present a rare case of CMV infection in pregnancy, causing haemorrhagic cystitis. This is the first reported case of CMV-induced haemorrhagic cystitis in pregnancy, as far as we are aware.
Case presentation
A 29-year-old woman, 22 weeks pregnant, was referred to our unit by our obstetric colleagues with a 1-day history of severe macroscopic haematuria. Further medical history noted that she had been diagnosed with HIV 2 months prior with a CD4+ count of 38 cells/mm3 and an HIV viral load of 1259 copies/ml at diagnosis. She had been initiated on antiretroviral therapy and has been compliant with treatment since. Her pregnancy has been uncomplicated to date. On initial examination, she was acutely ill, pale, tachycardic and tachypnoeic with a blood pressure of 112/71 mmHg. Her haemoglobin level was 6.2 g/dl. The rest of her examination, including a pelvic exam, was unremarkable. The bedside kidney-ureter-bladder (KUB) ultrasound was unremarkable, apart from a diffusely thickened bladder wall. A live, intrauterine singleton pregnancy with a gestation of 22 weeks was confirmed by transabdominal ultrasound.
She was admitted for intravenous fluid, and blood product resuscitation and continuous bladder irrigation were initiated.
A subsequent rigid cystoscopy demonstrated multiple areas of oedematous and erythematous bladder urothelium with areas of normal mucosa in between (Figure 1). Multiple bladder biopsies were performed using a cold cup biopsy forceps, and urine was sent for cytological analysis and microscopy and culture.

Cystoscopic images demonstrate a white mucosal plaque adjacent to the left ureteric orifice (a) as well as multiple areas of oedematous bladder urothelium with hyperaemia and non-specific changes (b–d).
Histopathological analysis of the bladder biopsy demonstrated multiple urothelial mucosal fragments infiltrated by a prominent mixed inflammatory population comprising neutrophils, lymphocytes, plasma cells and eosinophils and involving most of the fragments (Figure 2). In addition, multiple scattered cells throughout the fragments exhibited a viral cytopathy by way of enlarged nuclei with ill-defined basophilic to amphophilic intranuclear inclusions and paler amphophilic but similar large intracytoplasmic inclusions (Figure 2). These findings were morphologically consistent with a CMV infection and associated subacute cystitis, which was subsequently confirmed with positive CMV immunohistochemical stains (Figure 2). Her serum CMV viral load count was 113,383 IU/ml.
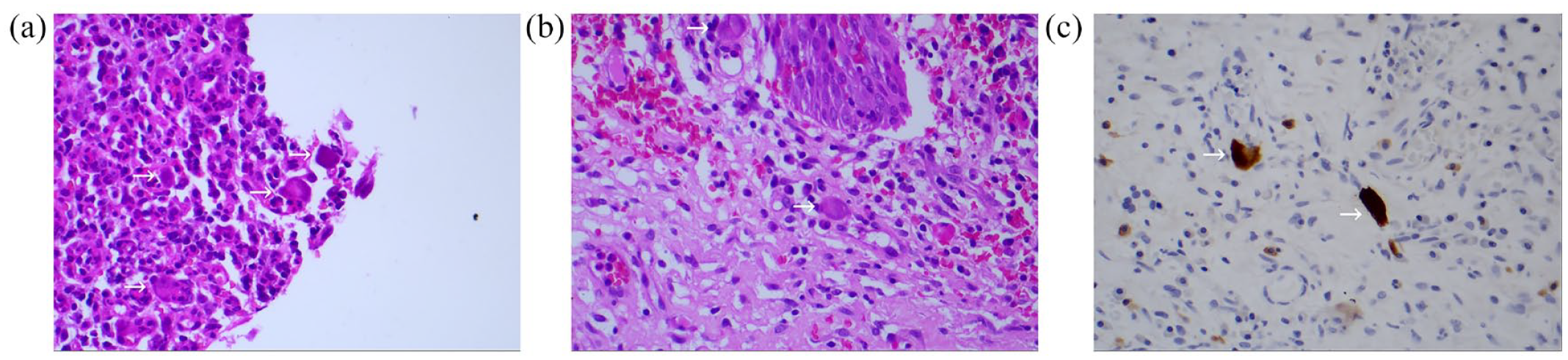
Histopathological analysis showing (a) multiple CMV-infected cells with amphophilic intracytoplasmic and intranuclear inclusions (H&E: 100×), with associated marked mixed inflammatory infiltrate in the background lamina propria, (b) CMV-infected cells with enlarged nuclei with ill-defined basophilic to amphophilic intranuclear and intracytoplasmic inclusions (H&E: 400×) and (c) positive immunohistochemistry in CMV-infected cells (H&E: 400×).
After a multidisciplinary team discussion with the patient regarding the benefits and risks of treatment, a combined decision was made to initiate antiviral therapy. She was commenced on 12 hourly intravenous Ganciclovir at a dose of 5 mg/kg for 14 days. It was decided not to continue her on an oral maintenance therapy in order to limit foetal exposure to the drug. Her haematuria promptly resolved after the initiation of antiviral therapy, and she was discharged after completing her course of antiviral treatment. Her pregnancy continued uncomplicated, and she delivered a healthy male infant at 38 weeks of gestation. The newborn was asymptomatic at birth, and viral polymerase chain reaction (PCR), audiology assessment, cranial ultrasound and neurodevelopmental assessment were reassuring. Six months post-partum, both the mother and infant are well with no signs or symptoms of active CMV disease or any signs of congenital CMV infection.
Discussion
Our reported case highlights a rare cause of haemorrhagic cystitis in a patient with AIDS with the added complexity that the patient was in her second trimester of pregnancy. Prevalence of CMV infection is around 0.5–1% of all live births, varying with geographic region. 5 Clinicians should be aware of CMV as a potential rare cause for haemorrhagic cystitis especially in immunocompromised patients because both the diagnosis and the decisions surrounding the treatment can be challenging. Adeno-, BK polyoma- and Epstein-Barr viruses are more common causes of viral haemorrhagic cystitis, particularly in post-transplant cases. 6 When CMV-induced haemorrhagic cystitis presents during pregnancy, as seen in our case, those decisions may have implications on the outcome of both the mother and the foetus.
Symptoms that may indicate bladder involvement may include haematuria (macroscopic or microscopic), dysuria, frequency or lower-abdominal pain. 6 There are no pathognomonic clinical findings, and clinicians should have a high index of suspicion to further investigate patients at risk.
Diagnosing CMV cystitis can often be difficult. Abnormal cystoscopic findings include hyperaemic, oedematous or inflamed urothelium, haemorrhagic inflammation or ulcerative bladder mucosal lesions.7–9 However, these findings are non-specific, and endoscopists should have a low threshold to biopsy abnormal-looking areas, especially in a severely immunocompromised patient. Some authors have suggested that deeper biopsies, which include the muscularis layer, might be necessary to confirm the diagnosis as CMV might only be detected in the muscle layer in certain cases. 10 The same non-specific findings may be seen on ureteroscopy if the ureter is involved, while retrograde pyelograms might reveal ureteral stenoses. 9 Severe CMV-related ureteritis may lead to ureteral necrosis and perforation. 11
The diagnostic value of CMV on histology is significant as other modalities such as serology or PCR analysis and detection in urine samples have limited specificity and cannot be used as a diagnostic tool in isolation.8,12 Histopathological features are characteristic and morphological findings can already suggest the diagnosis with confirmation via immunohistochemistry for CMV. The cardinal features of CMV infection include nuclear enlargement and cytomegaly of the infected cells. 8 Prominent large intranuclear and intracytoplasmic inclusions with a basophilic to amphophilic appearance are one of the pathognomonic findings.
Antiviral treatment with ganciclovir administered as a slow intravenous infusion or oral valganciclovir is the mainstay of treatment. Treatment recommendations for using these antiviral agents during pregnancy are scanty, as is information regarding their safety profile for the foetus. For this reason, the benefits of initiating antiviral therapy should be weighed up against the potential teratogenicity to the foetus. Deciding on the treatment duration is a further challenge in these patients. In tissue-invasive CMV infections, treatment is usually initiated as an induction phase for 14–21 days of antiviral therapy. This can be followed up with 1–3 months of oral valganciclovir as a maintenance phase at a lower dose to prevent relapse. Maintenance therapy, however, is not adopted universally, but should be considered in cases where there is an inadequate response to initial antiviral therapy. 13
Even though treatment of maternal CMV is not universally practised, more recently, some authors have reported benefits of treatment.14,15
Egloff et al., 15 in 2022, reported that the early treatment of pregnant women in the first and second trimesters is likely to reduce the risk of CMV transmission to the foetus [odds ratio (OR) = 0.40; 95% confidence interval [CI] 0.18–0.90, p = 0.03] with the greatest benefit seen when viraemia was positive. Considering our patient was symptomatic and had a very high CMV viral load, a joint decision was made at the multi-disciplinary team meeting to offer treatment. While the majority (90%) of newborns born to mothers with CMV remain largely asymptomatic at birth, approximately 10–15% of these asymptomatic babies may experience some degree of sensorineural hearing loss, which can be detected soon after birth or later in life.16,17 Diagnosis of congenital CMV in the first 3 weeks of life and early initiation of antivirals with oral valganciclovir for 6 months will reduce the risk of hearing loss caused by this infection. 17 Congenital CMV infection is symptomatic in about 10–15% of cases and is associated with problems with hearing, vision, nutrition, growth, cognition, learning, and motor/muscle tone and perinatal mortality of 10%. 18 Fortunately, the newborn in our case was asymptomatic at birth and viral PCR, audiology assessment, cranial ultrasound and neurodevelopmental assessment during the neonatal period were reassuring. Mothers who acquire CMV infection for the first time in pregnancy (primary infection) are associated with the most significant risk of in-utero transmission at 30–35%, 19 while non-primary infection have a significantly lower transmission rate at 1.4%. 20 Postnatal mother to child transmission through exposure to CMV-infected maternal blood or genital secretions during birth or breastfeeding is also possible but is generally not associated with adverse infant outcomes, except among very low-birthweight infants. 21
Conclusion
Although the prevalence of CMV is relatively common in the immunocompromised or immunosuppressed population, urinary tract manifestations of active CMV infection are rare. Our case highlights the necessity of clinicians to have a high index of suspicion for possible CMV-related cystitis or ureteritis in the case of unexplained haematuria, especially in the at-risk population group. Diagnosis with a formal cystoscopy and biopsy of bladder urothelium and prompt antiviral treatment is paramount, and even more so in the pregnant patient to prevent the devastating consequences for the infant. The decision to initiate treatment as well as the appropriate duration should be done by a multidisciplinary team and should take into account the benefits as well as the potential risks to both mother and foetus.