
Abstract
Urological calculus is a common disease in urology. Urological calculi are generally more common in adults but have become more common in children in recent years. Most existing studies focus on the prevention of urinary calculi in adults; there are relatively few articles on calculi in children. Reported preventive measures are not comprehensive enough, while the latest research progress has not been updated. The pathogenesis and preventive measures associated with urinary calculi have been the focus of research, but many preventive measures still need further clarification. This article reviews the progress on preventive measures for urinary calculi in children.
Introduction
The prevalence of urinary calculi in children is increasing year on year, with an average annual increase of 4–6%.1–3 This may be related to diet, 4 environment, 5 genetic inheritance,6,7 drugs, 8 etc. A study found that between 1993 and 2008, the number of children admitted to the emergency department for kidney stones increased by 86%; 9 25–50% of children had recurrence of kidney stones after the first kidney stone and approximately 70% of children developed recurrent stones between childhood and adulthood.10,11 Children and adults differ, chiefly in terms of metabolism, diet, weight, body surface area ratio, and behavioral cognition, which leads to differences in stone prevention. 12
Most kidney stones in children are calcium-based;13,14 other types of stones are rare. Besides specific lithogenic causes, secondary causes (such as drug induction, intestinal malabsorption, primary hyperparathyroidism, renal tubular acidosis, or infection) can also lead to stone formation. As a result, when treating secondary stones, we should pay more attention to their etiology. There are many dietary risk factors for the formation of idiopathic urinary stones as the composition of the urine is largely determined by diet. 15 In addition, daily liquid intake and ambient temperature are closely-related to urine metabolic concentration, which are also important influencing factors for stone-formation in children.
At present, urinary calculi are mainly prevented by increasing the concentration of various substances in the urine that inhibit the formation of calculi and reducing the concentration of various substances in urine that promote their formation. The end result is to prevent calcium salt precipitation in the formation of calculi. Research on the prevention of children’s calculi has always been a topic of considerable interest, but the field has suffered from several problems, including incomplete reports and old studies. The purpose of this review is to summarize the current literature and latest studies focused on the prevention of children’s urinary calculi. The aim is provide more complete data on their prevention and to discuss the future research directions.
Search strategy
We searched PubMed, Embase, and the Cochrane Library from their inceptions to August 2020 for published articles in English on urinary calculi and prevention in children from 0 to 18 years old. Based on review of the titles and abstracts, 108 of the 655 articles were potentially relevant to the prevention of nephrolithiasis in children. We summarized this literature and draw on studies performed in adult populations to expand areas where sufficiently high-quality research has not been carried out on children.
Dietary interventions
Low sodium diet
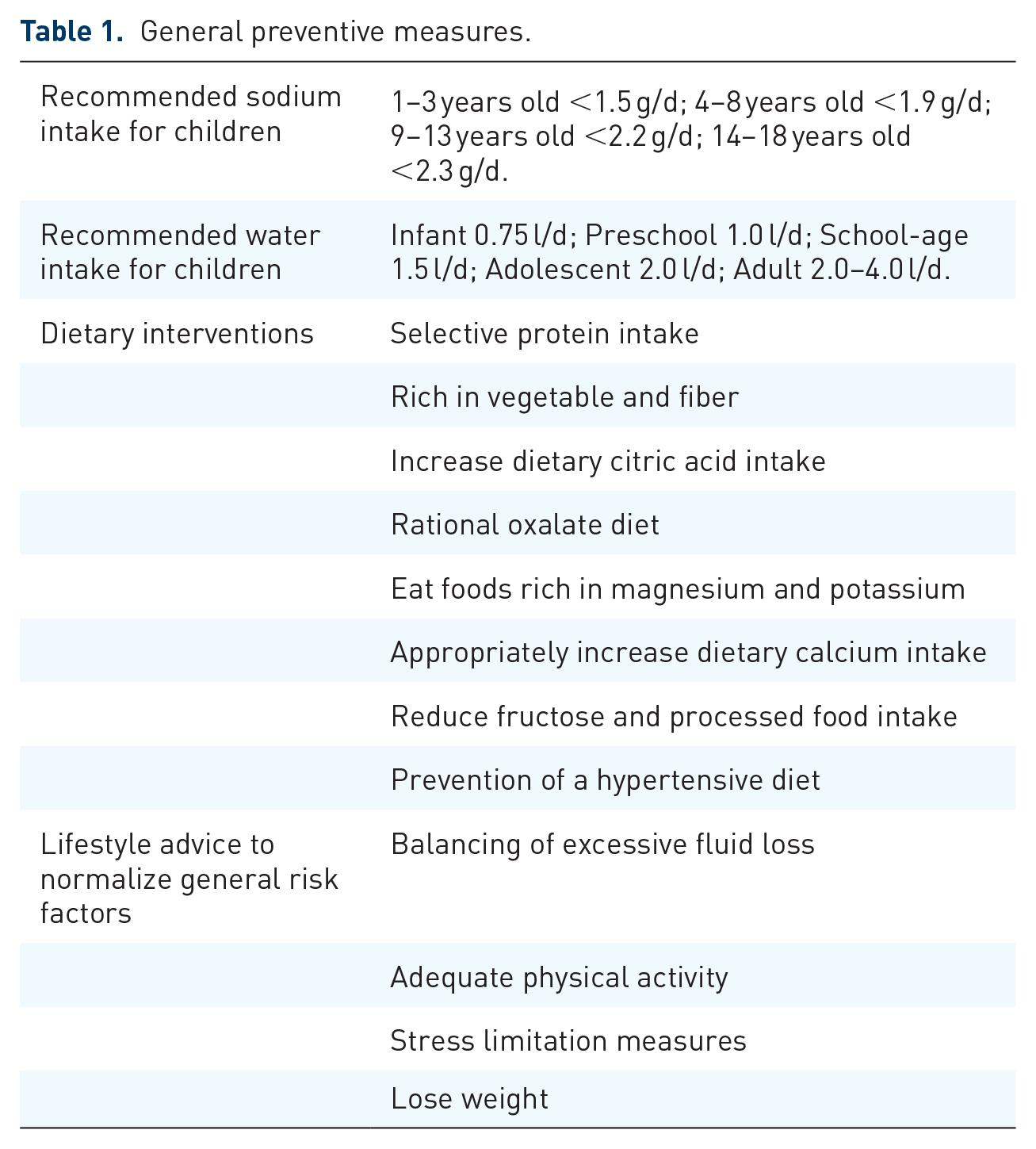
Studies have shown that a low sodium diet can reduce stone recurrence and urinary calcium excretion in patients with kidney stones. High sodium intake can promote the enhancement of sodium and calcium exchange in renal tubules, leading to hypercalciuria and promoting stone recurrence.16,17 The current medical recommendations for sodium intake in children are shown in Table 1.18,19 The recommended sodium intake can effectively prevent the recurrence of calculi in children with high calcinuria.
General preventive measures.
Appropriately increase dietary calcium intake
There are conflicting views on the effect of a calcium diet on stones. Previously, a high calcium diet was said to increase the risk of stones, while subsequent studies found that a high calcium diet reduced the risk of stones compared with a low calcium diet.20,21 The latter finding may be related to the combination of calcium and oxalic acid in the intestine that reduces the absorption of intestinal oxalic acid and reduces urinary oxalic acid excretion. Calcium is especially important to children’s growth and development, so dietary calcium intake should not be restricted. The current recommendation is to target the recommended daily intake of dietary calcium for the age group. 22
Eat foods rich in magnesium and potassium
Magnesium can inhibit the formation of crystals and stones. Low magnesium urine was found in 7–9% of children with urinary calculi.23,24 Magnesium can inhibit the formation of crystals and stones. Hypomagnesemia refers to a urine magnesium excretion rate less than 88 mg/1.73 m²/24 h. 25 For children with hypomagnesemia, a high magnesium diet helps prevent stone formation. Potassium also has a protective effect on stone formation, as reduced potassium intake increases calcium excretion and reabsorption of citric acid. 26 As a result, increasing dietary potassium intake is also beneficial. Foods’s rich in magnesium include millet, corn, soybeans, black beans, seaweed, carambola, and longan; foods rich in potassium include seaweed, banana, pumpkin, potatoes, and mushrooms.
Rational dietary oxalate intake
Hyperoxaluria is identified in 3–30% of children with urinary calculi.10,23,24,27,28 Hyperoxaluria is defined as urinary oxalate excretion exceeding 52 mg/1.73 m²/24 h.29,30 The role of hyperoxaluria in promoting urinary stone formation has been confirmed.10,24,28 For children with hyperoxaluria, restriction of dietary oxalate intake can be effective only if genetic primary hyperoxaluria has been excluded, as the metabolic disorders leading to excessive oxalate production far outweigh any dietary contribution. 31 However, many healthy foods (such as beans, animal offal, seafood, spinach, and grapes) are high in oxalate. Not eating these foods is not conducive to healthy childhood growth and development. Therefore, a low oxalate diet is recommended only for children with hyperoxaluria. Studies have found that there are great differences in the reported oxalic acid content of the same foods, 32 so we cannot give an exact intake standard, which may be related to the different sources of oxalate.
Increase dietary citrate intake
Hypocitraturia is common in children with calculi.10,23,24 Normal citrate excretion is related to age and sex. We can usually define hypocitraturia as less than 300 mg/1.73 m2/24 hours for girls and 180 milligrams/1.73 m2/24 hours for boys. 33 The presence of citrate in the urine binds free calcium, preventing it from forming crystals and stones and alkalinizing the urine. Hypocitraturia may be due to insufficient dietary citrate intake, or it may be the result of renal tubular acidosis or other forms of metabolic acidosis. For patients with severe hypocitraturia, evaluation for metabolic acidosis should be carried out. In addition to the treatment of the primary disease, dietary citrate intake should be increased. 34 For example, citrus fruits and juice have the most abundant citrate content. For children with hypocitraturia, it is recommended that they eat less animal protein and more fruit.
Selective protein intake
Protein may increase the risk of urinary calculi through the metabolism of sulfur-containing amino acids. 15 The risk of stone recurrence is increased due to increased net acid production and low citric acid. 20 At the same time, a diet containing animal protein rich in purines can lead to hyperuricemia, which is defined as uric acid excretion exceeding 815 mg/1.73 m²/24 h. 35 However, uric acid stones are common in adults but quite rare in children. This may be because children tend to have a higher urine pH than adults and low urine pH is more conducive to the formation of uric acid stones. Protein intake is essential for children’s growth and development. According to one study, compared with the lowest protein intaking males, men with the highest protein intake had a statistically significant 33% increased risk of stone formation, but the link was not consistent in women. This may be associated with protein sources. Red meat and poultry consumption may increase the risk of developing stones, while fish and animal consumption may be protective. 20 For high uric acid, low citrate content of children with stones, it is recommended to eat more fish and vegetable protein, and less animal protein, to prevent stones.
Reduce fructose and processed food intake
Children today are eating more processed foods (bread, chocolate, biscuits, fruit juices, fizzy drinks, etc.), while their milk intake has decreased and their intake of sugar-sweetened beverages has increased. Research shows that the sugar content of refined processed food is 8 times that of unprocessed food and 5 times that of the unprocessed food and ingredients combined.36,37 Fructose is found in most sugary foods and beverages. Studies have confirmed that high fructose intake increases the risk of stone development by 27–37%, which may be related to hypercalciuria, hyperoxaluria, hyperuricemia, and acidic urine. 38 Although fruit also contains fructose, the citric acid it provides can act as a protectant; as a result, fruit intake is beneficial in preventing stone formation. More research is needed to determine whether excessive consumption of processed foods, which tend to be high in sugar, sodium, and phosphorous preservatives may increase the risk of urinary stones.
Increase fluid intake
Adequate daily fluid intake is a key principle in stone prevention; primarily, this is achieved by reducing the concentration and saturation of the metabolites that form stones. Urine volume and urinary osmotic pressure are indicators of fluid intake, reflecting the extent to which a patient need to ingest fluids. Table 2 outlines the recommended water intake for children with urinary stone disease; children should calculate their fluid intake according to their body weight. 34 It is important to emphasize that not all fluids are useful for stone prevention. Water is usually the preferred fluid. As a result, simply increasing fluid intake alone is not necessarily effective for stone prevention, while individual differences do exist.
Characteristics and dosage of commonly used drugs for stone prevention.

bw, body weight.
Lose weight
Obesity has not yet been found to have an exact relationship with the causes of stone formation in children,54,55 but it has become a direct factor in adult stony formation.56,57 Studies have shown that, compared with children of normal weight with calculi, overweight or obese children with calculi have lower urine volumes and higher levels of uric acid. 58 As living standards improve, the levels of childhood obesity have become increasingly serious; this is consistent with the increasing prevalence of urinary stones in children. We can conjecture that being obese or overweight are also risk factors for stone formation in children. In short, losing weight is helpful for stone prevention.
Prevention of a hypertensive diet
Diets that prevent hypertension are encouraged to include low salt, low-fat dairy products, fish, whole grains, legumes, fruits, and vegetables. In theory, the benefits of such a diet for stone patients is related to their increased urinary citrate, adequate calcium intake, and reduced intake of red meat and fructose; potential risks also include increased intake of oxalate and vitamin C. 59 Previous studies have shown that there is a direct relationship between urinary calculus and blood pressure in children. 60 As a result, an antihypertensive diet is beneficial to prevent calculi in children.
Drug intervention
Supplement citrate
Oral citrate therapy increases the level of citric acid in the urine, which binds to calcium and inhibits crystallization, thereby reducing stone formation, as has been demonstrated clinically (Table 2).39,61 Given the adverse reactions and effects associated with this approach, the most commonly used intervention in clinical practice is sodium potassium hydrogen citrate. The efficacy of potassium citrate in the prevention of urinary calculi caused by hypocitraturia has been confirmed in children. 62
Thiazide diuretics
Thiazides enhance calcium reabsorption in the distal and proximal tubules and remain the first-line treatment for patients with hypercalciuria and recurrent calcium stones or high-risk first-time calculi.33,40,50 Most randomized controlled trials examining the effect of thiazide or thiazide diuretics on stone recurrence have shown significant beneficial effects, including both patients with and without hypercalciuria. Some scholars undertook a retrospective study of 28 children with idiopathic hypercalciuria and demonstrated that hydrochloric acid hydrochlorothiazide treatment can effectively reduce calcium in urine. 26 Thiazides are generally well tolerated in children; symptoms such as dizziness and low blood pressure are rare, although hypokalemia may occur. At present, commonly used thiazide diuretics include chlorothiazide ketone and hydrochloric acid hydrogen chlorothiazide. It is worth noting that a meta-analysis of 8 randomized controlled trials showed that the long-term use of thiazide diuretics for the prevention of stone recurrence is not recommended due to poor compliance, multiple side effects, and economic burden. 63 This also suggests that the long-term prophylactic use of hydrochlorothiazide is not recommended for children with non hypercalciuria or high-risk recurrent calcium stones in the prevention of calculus in children. At the same time, attention should be given to the occurrence of adverse events when taking this drug in children with hypercalciuria, recurrent calcium stones, or high-risk first calculi.
Other drugs
Allopurinol can reduce the recurrence rate of calcium oxalate stones in patients with excessive uric acid and normal urinary calcium, which may be related to its antioxidant effect that reduces calcium stone formation. 52 However uric acid stones are rare in children. For suspected primary hyperoxaluria, pyridoxine can be empirically administered. Tiopronin and penicillamine can increase the solubility of cystine. Potassium-preserving diuretics (such as amiloride) promote calcium reabsorption (Table 2). Magnesium salts and phosphates, which theoretically prevent stones, are no longer used clinically.
Intervention for environmental temperature and geographical factors
Elevated ambient temperature and different geographical factors are related to stone formation. Elevated temperature will increase surface evaporation, decrease urine volume, increase supersaturation, and increase the risk of lithogenesis.33,58 Some studies have speculated that the prevalence of calculi will increase by 10% in the future due to global warming. 5 In many developing countries, dehydration, fever, and chronic diarrhea caused by hot and dry climates are the main causes of stone disease.5,64 In Northern India and other parts of the world, such as Florida and the Ukraine, the lack of Oxalobacter formigenes (O formigenes), an intestinal oxalate-degrading bacteria, can cause absorptive hyperoxaluria, which increases the risk of developing calcium oxalate stones. 65 For the prevention of stones caused by environmental and geographical factors, targeted interventions should be carried out for specific reasons. For example, in high-temperature areas, adequate daily drinking water should be guaranteed, attention should be given to sunscreen use, and more fruits and vegetables should be eaten. For children in areas where O formigenes is scarce, oral supplementation with oxalate bacilli can be used. In short, targeted interventions should be carried out according to particular environmental and geographical factors.
Prevention of hereditary and secondary calculi
Kidney stones in children are partly genetic; it has been reported that 30–80% of patients may report a family history of calculi.66,67 Hereditary kidney stones have many causes, such as adenine phosphoribosyltransferase deficiency, Dent’s disease, cystinuria, familial hypomagnesemia with hypercalciuria, nephrocalcinosis, and single gene mutations, mainly due to rare renal tubular lesions or metabolic disorders. At an early age, if not adequately diagnosed and treated, patients are at high risk of developing progressive chronic kidney disease.68–70 At least 30 disease-causing single mutations were found to lead to a single gene form of the condition via autosomal recessive inheritance, autosomal dominant inheritance, and X-linked transmission. Fourteen single genes cause 15% of renal calculi or renal calcium syndrome cases. 71 Although single gene detection technology is still developing, early diagnosis of single gene calculi is still difficult. It is worth noting that recent studies have found that the diagnosis of the etiology of hereditary renal stones is significantly delayed. Studies have found that the mean age at diagnosis of hereditary renal stones is 28.6 years old; cystinuria is the most common cause, while primary hyperoxaluria is the most serious disease. 72 Hereditary kidney stones should be diagnosed and treated early. Dietary intervention will reduce the occurrence of surgery and stone recurrence.
The prevention of secondary kidney stones is based on intervention against the primary causes, such as drugs (atazanavir, ceftriaxone, vitamin D, vitamin C, carbonic anhydrase inhibitor, etc.), intestinal malabsorption, or infection.73,74 Thorough medical history and clinical testing are the only means to identify the cause of secondary kidney stones. Treating the etiology and giving the above preventive measures can effectively reduce the recurrence of calculi.
Conclusions and prospects
This review has comprehensively covered diet, drugs, environment, genetics, and primary diseases to offer intervention measures against recurrent urinary calculi in children. Most of the previous studies were conducted in adults, but this paper is a summary of the current research on the prevention and treatment of pediatric stones. Most children’s stones can be found; the effect of stone prevention can be achieved by eating more foods that inhibit the formation of stones and eating less of foods that promote the formation of stones. Drug treatment based on the results of urine metabolism can also achieve good results. Preventive measures based on environmental factors can effectively prevent calculi. Early diagnosis, early treatment, and targeted prevention should form the mainstay of approaches to hereditary kidney stones. The key to secondary calculi is active treatment of the primary disease. At the same time, there are some problems that have not been solved; relevant literature is scarce, impairing the health of children. For example, exposure to antibiotics is becoming increasingly serious and the main antimicrobial ingredients have been found in stones. 8 How do antibiotics affect the formation of stones? What is the relationship between rising global temperatures and stones? How can hereditary kidney stones be diagnosed and treated as early as possible? These may be the future direction of pediatric stone prevention research.
Footnotes
Author contributions
JZ: manuscript writing; ZH: manuscript writing and manuscript editing; TY: articles collection and review; GW: reviewed and revised the manuscript; HG: articles collection; PL: articles collection; YZ: articles collection; YZ: project development; JL: reviewed and revised the manuscript.
Contributed equally to this work: Jiao Zhong and Ziye Huang
All authors approved the final manuscript
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Grant No. 2019FE001(-149) and No.202001AY070001-062 from Yunnan Provincial Science and Technology Department/Kunming Medical University Joint Project of Basic Research, and Grant No. H-2017045 from Yunnan Medical Science Specialist Training Project.