
Abstract
Objective
There has not been a study that analyzed the composition of urinary stones from patients in the eastern Shandong region of China. Thus, we explored the composition of urinary stones in the eastern Shandong region of China and discuss the clinical significance of the findings.
Methods
A total of 3684 urinary calculi from the eastern Shandong region were collected in our study. Compositions of the stones were analyzed using an Automatic Infrared Spectrum Analysis System (type LIIR-20). The results were verified through manual analysis of the spectrograms, which was accompanied by polarizing microscopy and chemical analysis if necessary.
Results
Among the 3684 specimens, there were 1767 single-component stones and 1917 mixed-component stones. According to the main components of the stones, the stones were divided into the following types: calcium oxalate monohydrate stones (1779, 48.3%), anhydrous uric acid stones (1105, 30.0%), carbonate apatite stones (590, 16.0%), ammonium magnesium phosphate hexahydrate stones (143, 3.9%), calcium oxalate dihydrate stones (36, 1.0%), and cystine stones (31, 0.8%).
Conclusions
There was a relatively high rate of uric acid stones in patients from the eastern Shandong region of China.
Keywords
Introduction
Urinary calculi are one of the major urological diseases and they have the characteristics of high recurrence rates and impaired kidney function.1–3 Analyzing the composition of urinary stones in a region is of great significance for the diagnosis, treatment, and prevention of calculi. Currently, infrared spectroscopy is the standard method used to analyze urinary stone components. 4 Infrared spectroscopy can be used to analyze the crystal composition and non-crystal components of stones with fast detection speed and fewer required specimens. We collected 3684 stone specimens from April 2015 to March 2019 and analyzed their composition using an Automatic Infrared Spectrum Analysis System (type LIIR-20).
Materials and methods
This research study was approved by the Ethics Committee of Yantai Yuhuangding Hospital, and we obtained informed consent from all patients. Additionally, our study was registered. Compositions of stones were analyzed using an Automatic Infrared Spectrum Analysis System (type LIIR-20), and the main components of the stones were recorded. According to the European Society of Urology guidelines, 3 the stone components were divided into the following categories: calcium oxalate monohydrate, anhydrous uric acid, carbonate apatite, ammonium magnesium phosphate hexahydrate, calcium oxalate dihydrate, cystine, and ammonium urate. First, the stones were washed with water and placed in an oven at 70°C–100°C to dry. The stone powder (1 mg) was mixed with dry potassium bromide (200 mg), and then the mixture was ground with an agate mortar. We then baked the mixture for 10–30 minutes, took it out and pressed it to make a translucent sheet, which was quickly placed in the infrared spectrometer for scanning. Finally, the computer drew a spectrum and automatically analyzed the stone composition. The results were verified through a manual analysis of the spectrogram, which was accompanied by polarizing microscopy and chemical analysis when necessary.
Results
This study included a total of 3684 stone specimens, including those discharged by the patients themselves and stones removed by surgery. There were 2103 male and 1581 female patients, and their ages ranged from 2 to 82 years. The average age of the male subjects was 37.3 ± 16.9 years and the average age of female subjects was 42.3±15.6 years. There were 2512 (68.2%) patients with kidney stones, 1133 cases (30.8%) with ureteral stones, and 39 cases (1.1%) with bladder stones.
Among the 3684 specimens, there were 1767 single-component stones and 1917 mixed-component stones. Based on the main stone component, the following stone types were recorded: calcium oxalate monohydrate stones (1779, 48.3%), anhydrous uric acid stones (1105, 30.0%), carbonate apatite stones (590, 16.0%), ammonium magnesium phosphate hexahydrate stones (143, 3.9%), calcium oxalate dihydrate stones (36, 1.0%), and cystine stones (31, 0.8%). A representative spectrogram of each type of stone is shown in Figure 1. Most of the mixed stones contained calcium, primarily calcium oxalate stones and carbonate apatite stones (Table 1). The results of our study showed that the calcium oxalate stones were the most frequent, followed by uric acid stones, carbonate apatite stones, infectious stones, and cystine stones.
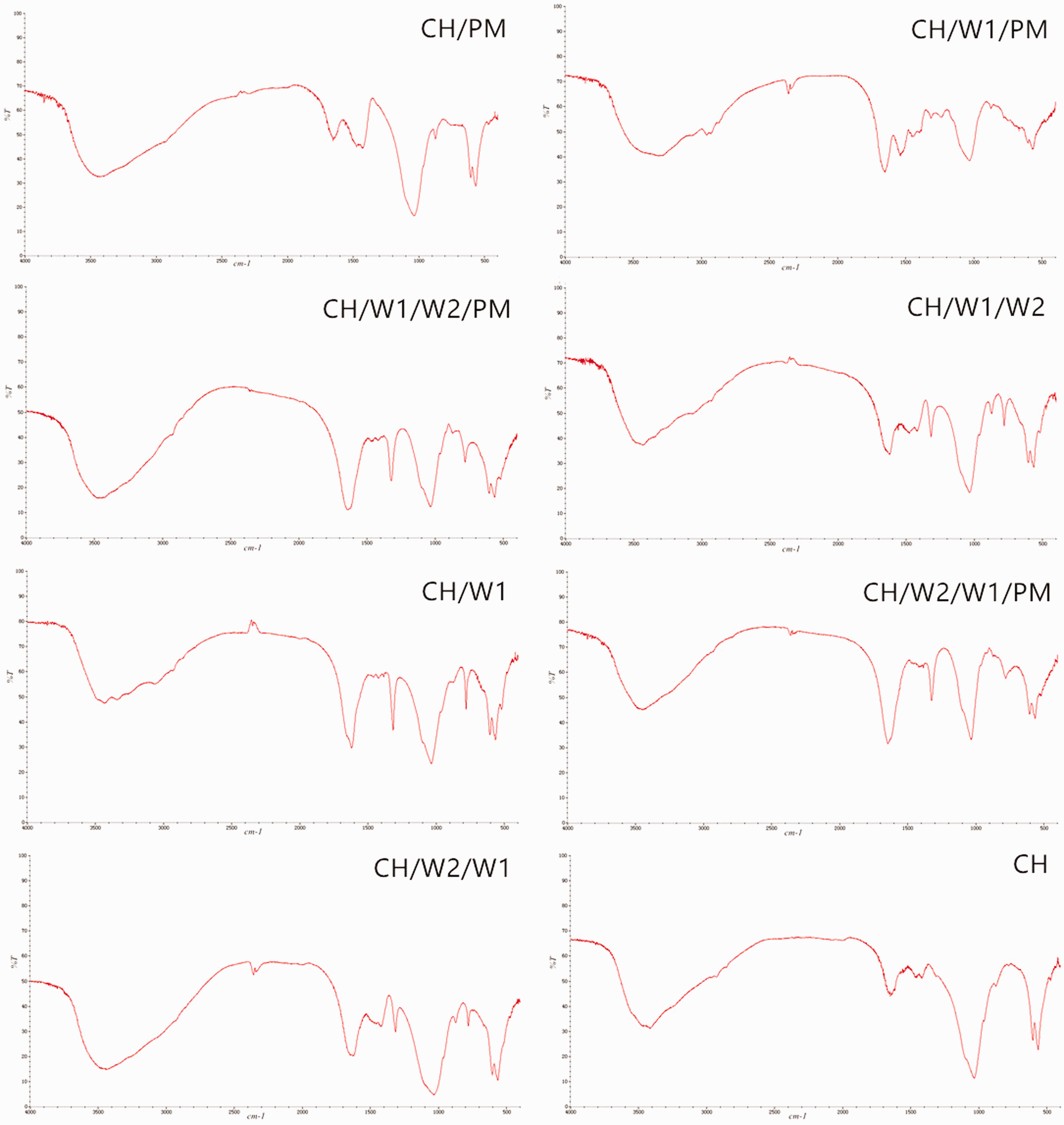
A representative spectrogram of each type of stone. T, transmittance.

A representative spectrogram of each type of stone. T, transmittance.

A representative spectrogram of each type of stone. T, transmittance.
Composition of urinary tract stones in the eastern Shandong region of China.

W1: calcium oxalate monohydrate; U: anhydrous uric acid; CH: carbonate apatite; PM: ammonium magnesium phosphate hexahydrate; W2: calcium oxalate dehydrates; CYS: cysteine; UA: ammonium urate.
Discussion
Schubert et al. 5 reported that chemical assays were the primary method of analyzing stone composition before the 1980s, accounting for 87% of studies, while infrared spectroscopy and X-ray diffraction methods accounted for only 8% and 5%, respectively. However, infrared spectroscopy has now become the primary method for analyzing stone components. 6 Infrared spectroscopy is a qualitative and quantitative method of analyzing substances and can determine molecular structures by the infrared spectra of samples, which has the advantages of accuracy, speed, and comprehensiveness.
The results of our automatic infrared spectrum analysis system showed that calcium oxalate stones were the most frequently detected, followed by uric acid stones, carbonate apatite stones, infectious stones, and cystine stones. Among the results, the proportion of calcium oxalate stones was the highest, which was similar to analyses in Northern, Eastern, Central, Southern, and Southwest China. 7 However, the detection rate of uric acid stones in the eastern Shandong region area was relatively high, which was quite different from the other regions. Previous studies have shown that diets with high meat intake and low vegetable intake are more likely to cause uric acid crystallization in the urine, which promotes the formation of uric acid stones. 8 Reduced vegetable intake also leaded to a decrease in oxalic acid excretion in the urine. 9 Thus, we conclude that the high proportion of uric acid stones may be related to the eating habits of residents of the eastern Shandong region. Foods such as animal protein and seafood account for a large proportion of the daily diet, which contains abundant purines and phosphorus. Moreover, many people in this region have a drinking habit. However, understanding the specific reasons will require further long-term research and analysis.
Similar to the results of other analyses,2,10 a male predominance was also found in our report. The proportion of male patients was higher than that of females, which may be related to dietary habits and sex hormone levels. 11 Our report also showed that stones with mixed components were more common than single-component stones. Most of the mixed stones contained calcium, primarily calcium oxalate and carbonate apatite; calcium-free stones were relatively rare. The content of calcium oxalate or calcium phosphate in stones was related to metabolic abnormalities. The formation of such stones is affected by many factors. Identifying the primary causes of stone formation requires a comparison of stone composition with both dietary habits and urine biochemistry.
The results of this study showed that the automatic infrared spectrum analysis system for urinary stones was accurate, automatic, and fast, providing high value and significance for the analysis of the causes of urinary stones. The stone compositions of patients from the eastern Shandong region of China had commonalities with other areas. According to the geographical environment of the eastern Shandong region, the eating habits and living standards of the residents combined with the analysis of stone compositions, the following suggestions and treatments are proposed for patients. (1) Patients with uric acid stones should appropriately limit the intake of foods containing purines, such as seafood, meat, animal offal, beer, bean products, mushrooms, and peas. (2) Patients with calcium oxalate stones should limit their high-protein diet and drinking, and try to reduce the intake of foods high in calcium oxalate, such as spinach, tomatoes, and beans. Additionally, these patients should eat more fiber-based foods to reduce the saturation of calcium salts, reduce the formation of calcium salts, and thus stone formation. (3) Patients with calcium phosphate stones should control urinary tract infections, eat more acidic foods, such as grains and peanuts, while also eating meat and peanuts in moderation. (4) Patients with cystine stones should eat more citrus or juice. They should also consider oral drugs that can generate alkaline urine, such as sodium bicarbonate and potassium citrate. (5) Mixed stones of various components can be simultaneously prevented according to the above recommendations. (6) All patients with urinary stones should drink more water, ensure that their daily urine volume is above 2000 mL, and regularly undergo imaging examinations as well as examinations for related metabolic indicators to actively prevent and reduce the recurrence of urinary stones.
Conclusions
There was a relatively high abundance of uric acid stones in patients from the eastern Shandong region of China.
List of abbreviations
W1: calcium oxalate monohydrate; U: anhydrous uric acid; CH: carbonate apatite; PM: ammonium magnesium phosphate hexahydrate; W2: calcium oxalate dihydrates; CYS: cystine; UA: ammonium urate.
Footnotes
Acknowledgements:
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Funding
This research received funding from Natural Science Foundation of Shandong Province (ZR2019MH132) and Yantai Key Research and Development Project (Grant 2019MSGY135).
Authors' contributions
CHL is the corresponding author for the article. XBZ is the first author, and JJM is co-first author. CHL designed the research, interpreted the data, and revised the paper. XBZ, JJM, and NW performed data extraction and drafted the paper. All authors have read and approved the final manuscript.
Ethics approval and consent to participate
All patients in this study provided written informed consent before treatment. All procedures used in this study were performed in accordance with the principles of the Research Ethics Committee of the Affiliated Yantai Yuhuangding Hospital of Qingdao University and with the 1964 Helsinki Declaration and its subsequent amendments.
Consent for publication
Not applicable.
Availability of data and material
The datasets used and/or analyzed in this study are available from the corresponding author upon reasonable request.