
Abstract
The aim of this study was to discuss the clinical significance of perirenal puncture and drainage with urokinase treatment of perirenal hematoma complicated by infection following surgery for upper urinary tract calculi. Two cases of perirenal hematoma complicated by infection following surgery for upper urinary tract calculi in 2017, and later received perirenal puncture and drainage of perirenal hematoma with urokinase treatment were selected. Puncture and drainage of perirenal hematoma with urokinase treatment were performed without the occurrence of severe complications such as sepsis, septic shock, or secondary bleeding. Both the renal morphology and functions were well restored. Puncture and drainage with urokinase treatment had definite efficacy in the treatment of perirenal hematoma complicated by infection.
Keywords
Perirenal hematoma is a lesion formed by renal cortical hemorrhage in the perirenal region due to trauma or iatrogenic injury. Most of the patients have abdominal and back pain, and a few have gross hematuria. About 11% of the patients suffer from peritoneal hematoma caused by severe hemorrhage, which further leads to hemorrhagic shock. 1 Some studies have reported the use of percutaneous perirenal puncture and drainage with urokinase treatment for perirenal hematoma without infection. However, whether this combined treatment can be applied to perirenal hematoma complicated by infection is still controversy. Here we reported two cases of perirenal hematoma complicated by infection due to iatrogenic injury, and obtained satisfactory effect via perirenal puncture and drainage with urokinase treatment.
Case description
Two patients suffered from renal calculi with urinary tract infection and right multiple renal calculi with hydronephrosis, respectively. Both patients had signed informed consent and suffered from low back pain after double-channel percutaneous nephrolithotomy (PCNL) or ureteroscopy. B-mode ultrasound and CTU (computerized tomography urogram) showed huge subcapsular hematoma. Later, they presented with septic shock and perirenal hematoma. The patient’s condition was improved after imipenem-based anti-infective therapy and correction of shock. As the hematoma was largely liquefied, the patient then received perirenal drainage of hematoma. Septic shock recurred after de-escalation therapy, and the patient’s condition was improved after another imipenem-based anti-infective therapy. Earlier drainage of hematoma was prioritized so as to avoid infection caused by perirenal hematoma. The following treatment was used as described by Ma et al.: 2 After the body temperature stabilized for 3 days, the patient received daily ultrasound physiotherapy plus low-pressure injection of urokinase 50,000 U + gentamicin 160,000 U (in 10-ml normal saline via the perirenal drainage tube) in addition to antibiotics. The perirenal drainage tube was clipped every day for 6 h and then reopened. The patient was reexamined by CT scan 1 week later, which revealed perirenal hematoma was significantly decreased. Septic shock did not recur after de-escalation therapy. No drained liquid was observed in the perirenal drainage tube for 5 days, and the drainage tube was then removed. The patients presented no renal atrophy, renal insufficiency, or hypertension of the affected kidney during follow-up (Figures 1–5).

Preoperative CT.

CT on the day of hemorrhage.

CT 2 weeks after hemorrhage.
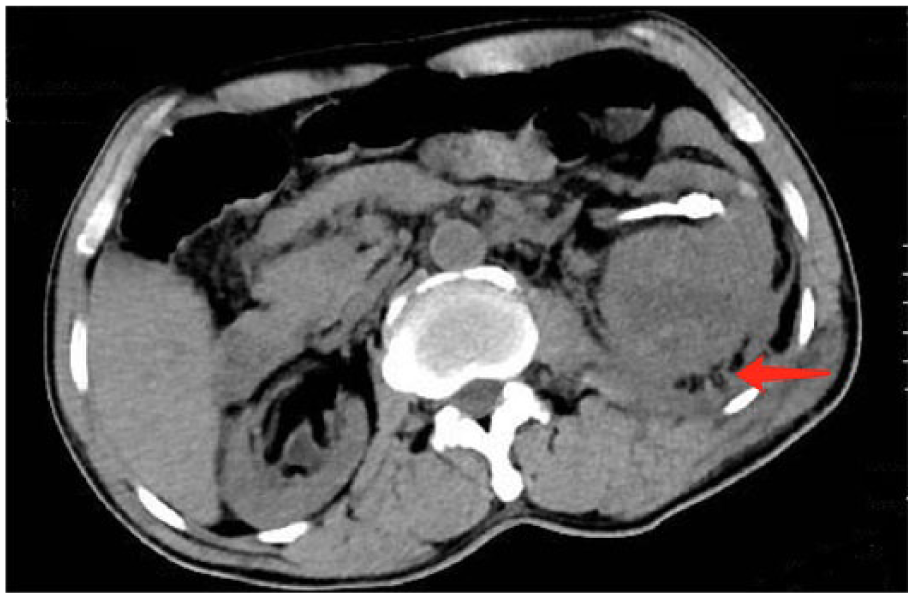
CT after perirenal drainage.
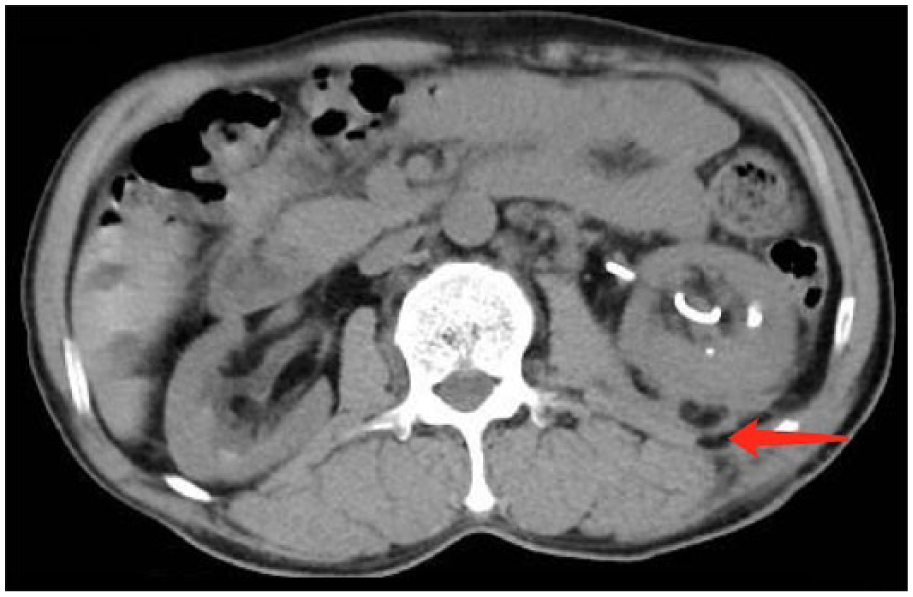
CT after urokinase treatment.
Discussion
Urinary tract calculus is the most common disease treated at the urinary surgery department. PCNL, ureteroscopy, and flexible ureteroscopy lithotripsy are common treatments. Although endoscopy has the benefits of small invasiveness in treating urinary tract calculi, it may cause hemorrhage, infections, injury to the surrounding organs, or even loss of the affected kidney, among other complications. Hemorrhage is the most common complication, 3 and postoperative perirenal hematoma and urinary extravasation may also happen.
Perirenal hematoma is a rare complication following endoscopic procedures for upper urinary tract calculi. 4 The timing and approach to treat perirenal hematoma complicated by infection after endoscopic procedures for upper urinary tract calculi have long been the major challenges in urinary surgery.
Urokinase is a protease extracted from fresh human urine, whose injection via the perirenal drainage tube can timely dissolve and drain the perirenal blood clots. Sterile condition, use of gentamicin, drainage tube position, the risk of rehemorrhage, the concentration and duration of urokinase, and ultrasound physiotherapy should be considered during injection for perirenal hematoma combined with infection.
Internal and external drainage is the necessary treatment for larger perirenal hematoma complicated by infection. Low-pressure perfusion of urokinase under the systemic and local use of antibiotics will not increase the risk of infection spread or rehemorrhage during perirenal puncture and drainage of perirenal hematoma complicated by infection. This combined treatment reduced the time of kidney compression by hematoma, shortened the length of stay in hospital, and decreased associated complications. Limited by sample size, the clinical value of this combined treatment remains to be further discussed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The scheme was authorized by the Ethics Committee of Affiliated Hospital of Zunyi Medical University.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Verbal consent was obtained from the patients for this study.