
Abstract
Cystitis cystica et glandularis (CCEG) is widely believed to be innocuous and self-limiting. We report a case of a 32-year-old male patient who was found to have gross bilateral hydroureter and hydronephrosis and an estimated glomerular filtration rate of 3 ml/min/1.73 m2. Cystoscopy revealed extensive cystic and nodular lesions involving most of the bladder urothelium, which proved to be CCEG on histopathological analysis. Retrograde and anterograde stents could not be inserted due to obstruction of the ureters at the level of the vesicoureteric junction. Percutaneous nephrostomies were subsequently inserted. Although there was evidence of improvement of the CCEG on follow-up cystoscopy, no improvement of renal function, despite decompression with percutaneous nephrostomies, was seen. He was subsequently placed on the waiting list for a renal transplant. We believe this to be the only known case reported of florid CCEG obstructing the upper urinary tracts bilaterally, causing irreversible renal injury.
Keywords
Introduction
Cystitis cystica (CC) and cystitis glandularis (CG) are benign, proliferative conditions of the bladder mucosa usually present in a setting of chronic mucosal irritation or inflammation. These lesions are commonly identified in the bladder, with a prevalence of 60–70% of cases in various autopsy studies. 1 Although they may occur in isolation, they often coexist and the condition is then referred to as cystitis cystica et glandularis (CCEG). 2 Although regarded as innocuous and self-limiting in the vast majority of cases, CCEG may obstruct the ureteral openings and cause renal dysfunction. 3 We report what we believe to be the only known case in the literature of florid CCEG obstructing the upper urinary tracts bilaterally, causing irreversible renal injury.
Case presentation
A 32-year-old human immunodeficiency virus (HIV)-negative male patient was referred to our unit with a 2-week history of bilateral flank pain and nausea. He was found to have gross bilateral hydroureter and hydronephrosis and a blood serum urea level of 87.5 mmol/l, creatinine 1840 μmol/l and an estimated glomerular filtration rate of 3 ml/min/1.73 m2. No significant post micturition residual bladder volume that would suggest a bladder outlet obstruction was noted on ultrasound. The history was further unremarkable, with no prior hematuria, lower urinary tract symptoms, surgical procedures, urolithiasis, or previous urinary tract infections. The clinical examination found him afebrile and normotensive with mild bilateral loin tenderness. Specimens for urinalysis and culture revealed no evidence of urinary tract infection, tuberculosis or schistosomiasis.
Urgent hemodialysis was commenced, and a cystoscopy noted extensive cystic and nodular lesions involving most of the bladder urothelium, but especially prominent at the trigone and bladder neck. The ureteric orifices could not be visualized, and retrograde stenting proved impossible. Biopsies of the abnormal bladder urothelium noted multiple foci of CCEG (Figure 1) and no evidence of dysplasia, malignancy, tuberculosis, or schistosomiasis.
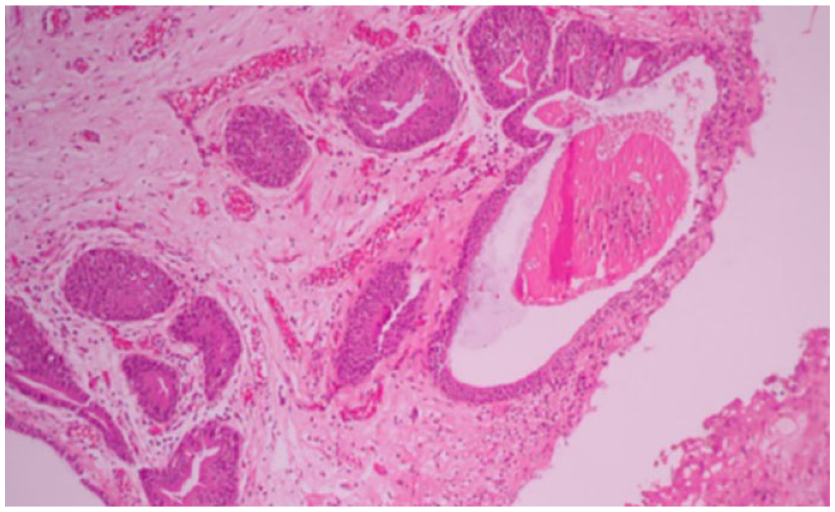
Photomicrograph of bladder biopsy showing superficial nests of urothelial mucosa with cystic change in the background of chronic inflammation.
Bilateral percutaneous nephrostomies were inserted forthwith, and bilateral anterograde pyelography revealed distended ureters with complete obstruction at the level of both vesicoureteral junctions (Figure 2). No filling defects suggestive of concomitant ureteritis cystica were noted. At this stage, our management plan was to continue dialysis with the bilateral percutaneous nephrostomies in situ and allow time for the CCEG, generally regarded as self-limiting, to resolve. Computed tomography (CT) cystogram showed a good capacity bladder, with no evidence of pelvic lipomatosis (Figure 3).

Anterograde study at the time of cystoscopy showing complete bilateral vesicoureteric junction obstruction with no contrast passing from the ureter into the bladder.

CT cystogram showing a good capacity bladder with no evidence of pelvic lipomatosis.
Repeat cystoscopy 6 weeks later did show a marked improvement, with bladder lesions now limited only to the bladder neck and trigone. Careful resection of the remaining lesions on the trigone exposed slit-like ureteric orifices (Figure 4), but unfortunately, these orifices could not be catheterised. Repeat anterograde pyelography showed no resolution of the complete obstruction at the lower extent of both ureters.
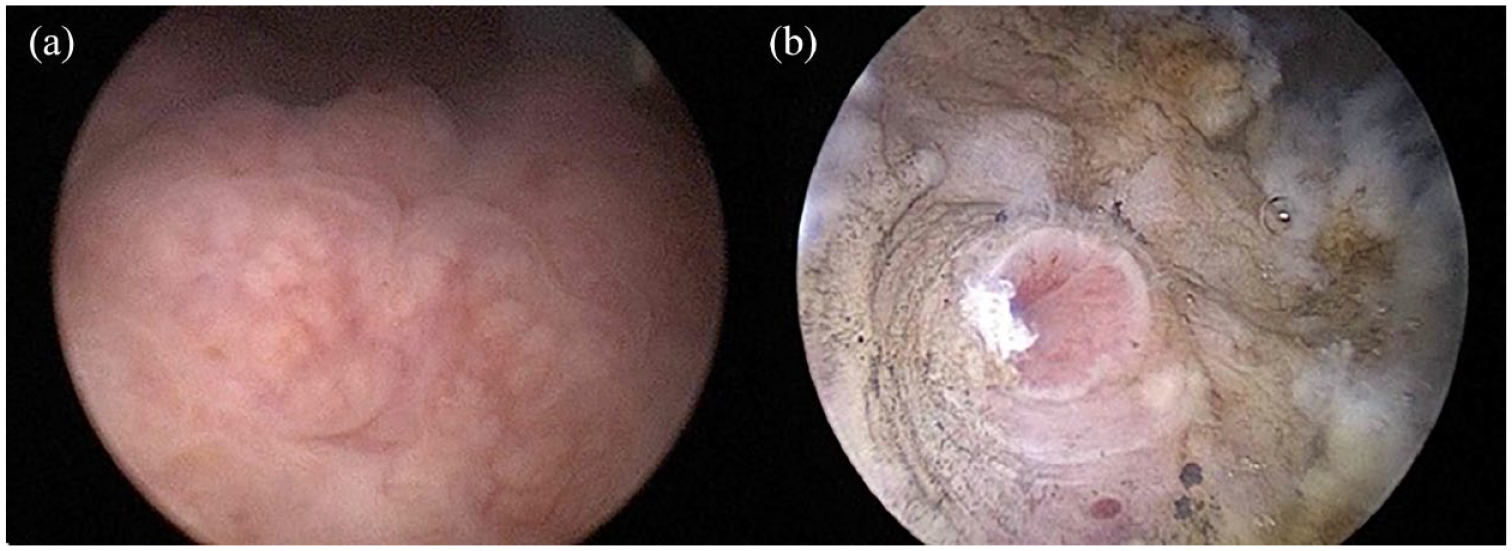
Cystoscopic view showing nodular lesion over the right ureteric orifice (a) with the slit-like right ureteric orifice visible after careful transurethral resection of the bladder lesion (b).
The patient’s serum renal function showed no improvement despite the decompressing effect of the bilateral percutaneous nephrostomies. Seeing that follow-up cystoscopy showed resolution of the macroscopic cystic and nodular lesions in the bladder and no lesions requiring re-resection, a multidisciplinary decision was made to continue hemodialysis and place our patient on a waiting list for a renal transplant.
Discussion
CCEG is a benign, proliferative lesion of the bladder mucosa characterized by the von Brunn’s nests growing into the lamina propria become cystically dilated (CC) and metaplastically changing into goblet cells within the mucosa and submucosa of urinary bladder epithelium (CG). 1 All three conditions commonly coexist and can be identified in various settings, including normal bladder mucosa, inflammatory diseases, and carcinoma. 4 The exact pathophysiology is not known but is most likely related to chronic irritation of the bladder mucosa with activation of the humoral immune defence response, 5 and tends to be associated with recurrent urinary tract infections, chronic bladder outlet obstruction, 6 neurogenic bladder, bladder calculi, or catheterization. 7 Interestingly, pelvic lipomatosis – a rare proliferative condition that causes increased deposition of fat around the bladder, rectum and prostate – is associated with CG, which is found in up to 75% of patients with pelvic lipomatosis. 8
The majority of patients are asymptomatic, and the lesions are usually seen incidentally during cystoscopy. In symptomatic patients, hematuria, irritative lower urinary tract symptoms, and, rarely, upper urinary tract obstruction is the most common presenting complaint, as was our patient’s case. Cystoscopically, florid CCEG often appears as submucosal nodules. 7 Our case is a rare case of extensive CCEG causing a prolonged bilateral ureteric obstruction resulting in end-stage renal failure, requiring renal transplant – the first known case in the English literature. Other documented cases of CCEG causing obstruction, albeit without causing irreversible renal injury, have been reported. Zhu et al. described a patient with CCEG causing unilateral ureteric obstruction and acute azotaemia (creatinine, 231 μmol/l) in whom no underlying cause for CCEG was identified. The patient required resection of the 4 cm bladder mass before renal function returned to baseline. 3 Demirer et al. described a case of CCEG causing bilateral ureterovesical obstruction leading to renal colic, bilateral ureterohydronephrosis, and hematuria, which was managed by transurethral resection. 9
The association between CCEG and adenocarcinoma of the bladder, first reported in 1950, is controversial. 10 More recently, Yi et al. retrospectively evaluated 166 patients with CG, and concluded that isolated CG does not increase the risk of carcinoma of the bladder. 11 Therefore, follow up in the form of repeated cystoscopies is not warranted. However, in the presence of dysplasia, long-term clinical follow up with cystoscopies is warranted. 12 Fortunately, in our patient, there was no evidence of dysplasia on histopathological analysis.
A variety of definitive treatment options are available that range from conservative to aggressive. Firstly, identifying, treating, and eliminating the underlying predisposing source of chronic bladder irritation is the most crucial aspect of management. This includes eradicating urinary tract infections with appropriate antibiotic treatment, replacing chronic indwelling catheters with clean intermittent catheterization, or treating bladder calculi. Symptomatic patients presenting with bladder outlet obstruction, recurrent hematuria, or obstruction of the ureteric orifices should be managed with transurethral resection. 5 Success with these conservative measures is more appropriate for small, focal lesions. 13 In patients experiencing debilitating symptoms, more invasive and aggressive surgical options will need to be considered. Patients with decreased bladder capacity may benefit from a bladder augmentation, and, in patients with persistent ureteral obstruction, ureteral reimplantation is indicated. 13 Radical cystectomy with an orthotopic neobladder is the most aggressive yet successful surgery performed in highly selected cases. 14 Unfortunately, in our case, although the CCEG had improved significantly, the long-standing bilateral ureteric obstruction had caused irreversible renal failure.
Conclusion
Although CCEG is regarded as a common benign self-limiting condition requiring minimal intervention in most cases, it may, very rarely, obstruct the upper urinary tracts. We present the first described case in which CCEG caused bilateral ureteric obstruction and irreversible renal damage. Furthermore, given that there may be a risk of invasive carcinoma, in cases of CCEG with dysplasia, questions arise about how benign this condition is, whether it needs to be monitored more closely, and what the optimal duration of follow up should be.
Footnotes
Author contributions
KB and JJ reviewed the literature and drafted the manuscript. JL and KK reviewed and edited the manuscript. All authors issued final approval for the version to be submitted for publication.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for the anonymised information and the accompanying images to be published in this article.