
Abstract
Background:
Primary adenocarcinoma of the bladder (ACB) is a rare malignant tumor of the bladder with limited understanding of its incidence and prognosis.
Methods:
Patients diagnosed with ACB between 2004 and 2015 were obtained from the SEER database. The incidence changes of ACB patients between 1975 and 2016 were detected by Joinpoint software. Nomograms were constructed based on the results of multivariate Cox regression analysis to predict overall survival (OS) and cancer-specific survival (CSS) in patients with ACB, and the constructed nomograms were validated.
Results:
The incidence of ACB was trending down from 1991 to 2016. A total of 1039 patients were included in the study and randomly assigned to the training cohort (727) and validation cohort (312). In the training cohort, multivariate Cox regression showed that age, marital status, primary site, histology type, grade, AJCC stage, T stage, SEER stage, surgery, radiotherapy, and chemotherapy were independent prognostic factors for OS, whereas these were age, marital status, primary site, histology type, grade, AJCC stage, T/N stage, SEER stage, surgery, and radiotherapy for CSS. Based on the above Cox regression results, we constructed prognostic nomograms for OS and CSS in ACB patients. The C-index of the nomogram OS was 0.773 and the C-index of CSS was 0.785, which was significantly better than the C-index of the TNM staging prediction model. The area under the curve (AUC) and net benefit of the prediction model were higher than those of the TNM staging system. In addition, the calibration curves were very close to the ideal curve, suggesting appreciable reliability of the nomograms.
Conclusion:
The incidence of ACB patients showed a decreasing trend in the past 25 years. We constructed a clinically useful prognostic nomogram for calculating OS and CSS of ACB patients, which can provide a personalized risk assessment for ACB patient survival.
Introduction
Bladder cancer comprises 81,190 cancer cases and 17,240 deaths in the United States each year. 1 As a subtype of non-urothelial carcinoma, primary adenocarcinoma of bladder (ACB) is a rare malignancy with a poor prognosis, and is estimated to account for 0.5–2% of all bladder malignancies. 2 Some studies suggested that non-urothelial subtypes have lower survival rates than urothelial carcinoma, and that the former will be diagnosed in more advanced stages and be more aggressive.3–5 Surgical resection has been the standard treatment for ACB, but the 5-year survival rate of 11–61% is unsatisfactory.3,6–8
Due to the rarity of ACB, the identification and clinical management of the disease relies on retrospective reviews and case reports, and there is no consensus on its survival prognosis, but there have been several studies revolving around possible factors and measures.9–11 One study involving 185 cases of ACB showed that tumor stage, grade, and lymph node involvement were the only significant prognostic factors. 12 Furthermore, Zaghloul et al. 13 reported adeno-subclassification was associated with the prognostic outcomes of ACB. Currently, the Tumor-Node-Metastasis (TNM) staging system devised by the American Joint Committee on Cancer (AJCC) is a globally recognized method for predicting patient prognosis. However, the TNM system ignores other possible factors, such as demographic information and treatment, which may be strongly associated with the survival outcomes, although some of these factors have not been thoroughly studied. In addition, the current AJCC system only serves to classify patients into groups, rather than predicting individualized survival probability. In conclusion, clinicians are in need of a convenient, comprehensive, and accurate prognostic model.
As a graphical tool for statistical analysis, nomogram can improve the accuracy of predicting prognosis.14,15 Because the nomogram takes into account a variety of important clinical and pathological factors, generating individualized survival probability results at specific time points, it has been shown to be more accurate than risk group allocation models and staging systems as a reliable tool for prognosis, guidance, and treatment.16–18
Currently, there are no validated prognostic models for patients with ACB, although this is one of the most lethal histological types of bladder cancer. The aim of this study was to establish nomograms to predict the prognostic outcome of patients with ACB based on important clinicopathologic parameters, demographic information, and treatments.
Patients and methods
Study population
In this study, all data of patients were obtained from the Surveillance, Epidemiology, and End Results (SEER) database between 1975 and 2016, which collects and publishes data including cancer incidence and mortality from 18 cancer registries that cover approximately 28% of the population of the United States. 19 The study cohort consists of patients who met the following criteria: (1) age greater than 18 years; (2) positive histology; (3) histological type limited to primary adenocarcinomas of bladder (ICD-O-3 codes: 8140/3, 8260/3, 8310/3, 8323/3, 8480/3, 8490/3); (4) active follow-up with complete date; (5) clear TNM staging. We excluded patients with unknown survival time, multiple tumors, Ta, Tis, and T0 stages. After selection, 1039 constructive patients were enrolled in the cohort (Figure 1).

Flow chart of this study.
Study variables and outcome
The variables analyzed in this study were age at diagnosis, sex, marital status, race, primary site, histology, grade, pathological stage (AJCC stage, T stage, N stage, M stage, and SEER stage), surgery of the primary tumor, chemotherapy, and radiotherapy. We regrouped some variables: age at diagnosis was grouped as “<68,” “68–79,” and “>79” using X-tile software (Figure S1); patients whose marital status was “Single,” “Divorced,” “Separated,” “Widowed,” or “Unmarried or Domestic Partner” were regrouped as “Unmarried”; and patients whose race was recorded as American Indian/Alaska Native or Asian/Pacific Islander were grouped as “Other” racial categories. The gross pathologic types of ACB include six types: “Adenocarcinoma, NOS,” “Mucinous adenocarcinoma,” “Signet cell carcinoma,” “Clear cell adenocarcinoma,” “Papillary adenocarcinoma,” and “Mixed subtype adenocarcinoma.” The surgical treatment variable was grouped into “Surgery, NOS,” “Partial cystectomy,” “Radical cystectomy,” and “No/Unknown.” The chemotherapy and radiotherapy variable were grouped into “Yes or No/Unknown.” Additionally, T stage was regrouped into T1, T2, T3, T4, and Unknown, N stage was regrouped into N0, N1, N2, N3, and Unknown, M stage was regrouped into M0, M1, and Unknown. The primary endpoints of the study were overall survival (OS) and cancer-specific survival (CSS). Survival time was calculated from the date of diagnosis to death or last follow-up. Frequency and proportion were reported for each variable analyzed in this study.
Statistical analysis
The incidence of ACB patients between 1975 and 2016 was analyzed using Joinpoint software (Version 4.8.0.1), and the incidence rate is expressed as the annual percentage change (APC) and the 95% confidence interval (CI). Using RStudio software (Version 1.2.5033), all patients were randomized into a training set and validation set in a 7:3 ratio. In the training set, univariate Cox regression analysis was used to verify whether the association between each variable and OS and CSS was significant. After excluding the non-significant variables, multivariate Cox regression analysis was then used to calculate the association between each variable and OS and CSS to find independent risk factors. The measure of association was presented in the form of hazard ratio (HR) and 95% CI. Nomograms in this study were created using information obtained from multivariate Cox regression analysis. Receiver operating characteristic (ROC) curves, concordance index (C-index), decision curve analysis (DCA) curves, and internal validation were used to assess the predictive performance of nomograms. The area under the ROC curve is represented by AUC and the C-index assessment was performed using RStudio software. Calibration curves of the nomograms were applied to evaluate the consistency between predicted survival and observed survival bootstraps with 1000 resamples were used for the validation. 20
In the RStudio software, analysis and validation were performed using survival, rms, Hmisc, lattice, Formula, ggplot2, rmda, pROC, and timeROC packages. All statistical tests were considered statistically significant at p < 0.05.
Results
Incidence trends of ACB patients
Figure 2 shows the change in the incidence of ACB between 1975 and 2016. We found that in all populations, the incidence of ACB increased from 1975 to 1991 (1975–1986 APC = 0.47; 1986–1991 APC = 3.34) and decreased from 1991 to 2016 (1991–2009 APC = −0.58; 2009–2016 APC = −2.82). In addition, the incidence in males was generally consistent with the overall trend (Figure 2b), while the incidence of females declined annually over the past 40 years (Figure 2c).

Incidence of adenocarcinoma of the bladder (ACB) patients from 1975 to 2016. In all populations. (a) The incidence of ACB increased from 1975 to 1991 and decreased from 1991 to 2016. Incidence in male patients (b) was generally consistent with the overall trend; the incidence of female patients (c) declined annually over the past 40 years.
Patients’ baseline characteristics
According to the inclusion criteria, we selected a total of 1039 patients in this study, including 727 in the training set and 312 in the validation set. The demographic, tumor, and treatment characteristics of the cohort are listed in Table 1. In general, the majority of patients were white (806, 77.6%) married (512, 49.3%), and younger than 68 years old (603, 58%), male (635, 61.1%), with grade III (348, 33.5%). With regard to therapy, most patients have partial cystectomy (665, 64.0%), without chemotherapy (725, 69.8%), or radiation (891, 85.8%).
Baseline demographic and clinical characteristics.

AJCC, American Joint Committee on Cancer; NOS, not otherwise specified; SEER, Surveillance, Epidemiology, and End Results.
Univariable and multivariable Cox regression in the cohort
We used univariate and multivariate Cox regression to analyze the relationship between these selected characteristics and OS or CSS. As shown in Table 2, in the training set, multivariate Cox regression showed that age, marital status, primary site, histology type, grade, AJCC stage, T stage, SEER stage, surgery, radiotherapy, and chemotherapy were independent prognostic factors for OS. Age, marital status, primary site, histology type, grade, AJCC stage, T stage, N stage, SEER stage, surgery and chemotherapy were independent prognostic factors for CSS (Table 3).
Univariate and multivariate analysis of overall survival (OS) rates in training set.
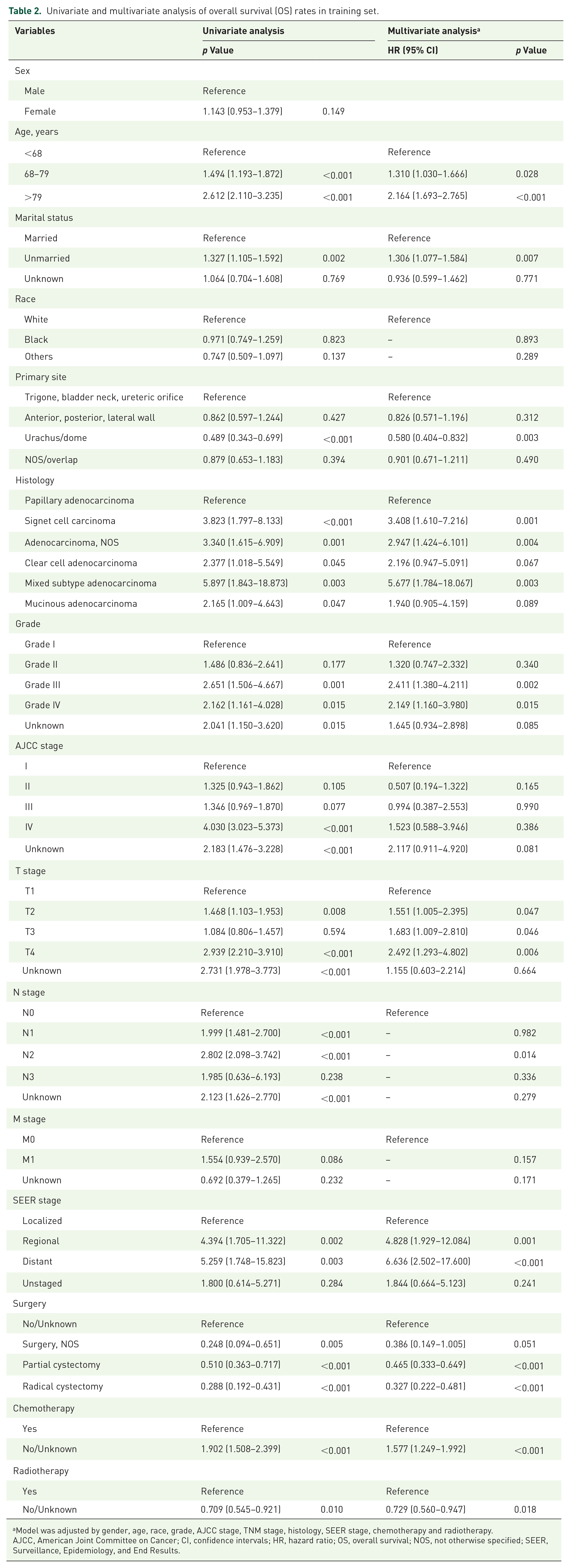
Model was adjusted by gender, age, race, grade, AJCC stage, TNM stage, histology, SEER stage, chemotherapy and radiotherapy.
AJCC, American Joint Committee on Cancer; CI, confidence intervals; HR, hazard ratio; OS, overall survival; NOS, not otherwise specified; SEER, Surveillance, Epidemiology, and End Results.
Univariate and multivariate analysis of cancer-specific survival (CSS) rates in training set.

Model was adjusted by gender, age, race, grade, AJCC stage, TNM stage, histology, SEER stage, chemotherapy and radiotherapy.
AJCC, American Joint Committee on Cancer; CI, confidence intervals; CSS, cancer-specific survival; HR, hazard ratio; NOS, not otherwise specified; SEER, Surveillance, Epidemiology, and End Results.
According to Tables 2 and 3, prognostic outcomes and mortality risk of patients can be intuitively evaluated. For example, older patients may have higher possibilities to experience worse OS and CSS outcomes. Similarly, single patients with histology of papillary adenocarcinoma are more likely to have poor prognoses. As for therapy, a “surgery, NOS” cystectomy with chemotherapy may help patients to get an advantageous consequence for both OS and CSS, as other studies reported.
Prognostic nomograms for OS and CSS and validations
All independent risk factors in the multivariate Cox regression analyses were taken into consideration in nomograms for 3- and 5-year OS and CSS, as shown in Figure 3. We found that SEER stage contributes the most to OS and CSS. According to the HR, each variable was assigned a point. The total points for each variable are then summed and positioned on the total points table to obtain the probability of 3 and 5 years of OS and CSS. For example, with the nomogram for OS, one can conclude that if a 70-year-old married man with primary site of bladder neck, grade III, T2, III for AJCC stage, Regional of SEER stage, papillary adenocarcinoma has taken partial cystectomy, chemotherapy without radiotherapy, he would score about 290 points, which means that this patient has approximately 40% possibility of survival in the third year and approximately 30% possibility of survival in the fifth year.

Prognostic nomogram of (a) overall survival (OS) and (b) cancer-specific survival (CSS) in patients with adenocarcinoma of the bladder.
Subsequently, we tested the predictive ability of the nomograms using the C-index, ROC curves and DCA curves. We found that the predictive ability of the nomogram was better than the TNM stage in both the training and validation sets (Table 4 and Figure 4). In addition, the nomograms were also able to predict 3-year and 5-year OS and CSS better, and the AUCs of the nomograms were greater than 0.8, suggesting that the nomograms had good predictive ability (Figure 5). Moreover, we used calibration curves to detect comparisons between the predicted and actual survival times of the nomograms. The calibration curve in Figure 6 is very close to the ideal curve, showing good agreement between the predictions of the nomograms and the actual observations in the training and validation sets, suggesting appreciable reliability of the nomograms.
Comparison of C-indexes and AUC between the nomogram and SEER stage in patients with adenocarcinoma of the bladder.

AUC, area under the curve; CI, confidence interval; HR, hazard ratio; SEER, Surveillance, Epidemiology, and End Results.
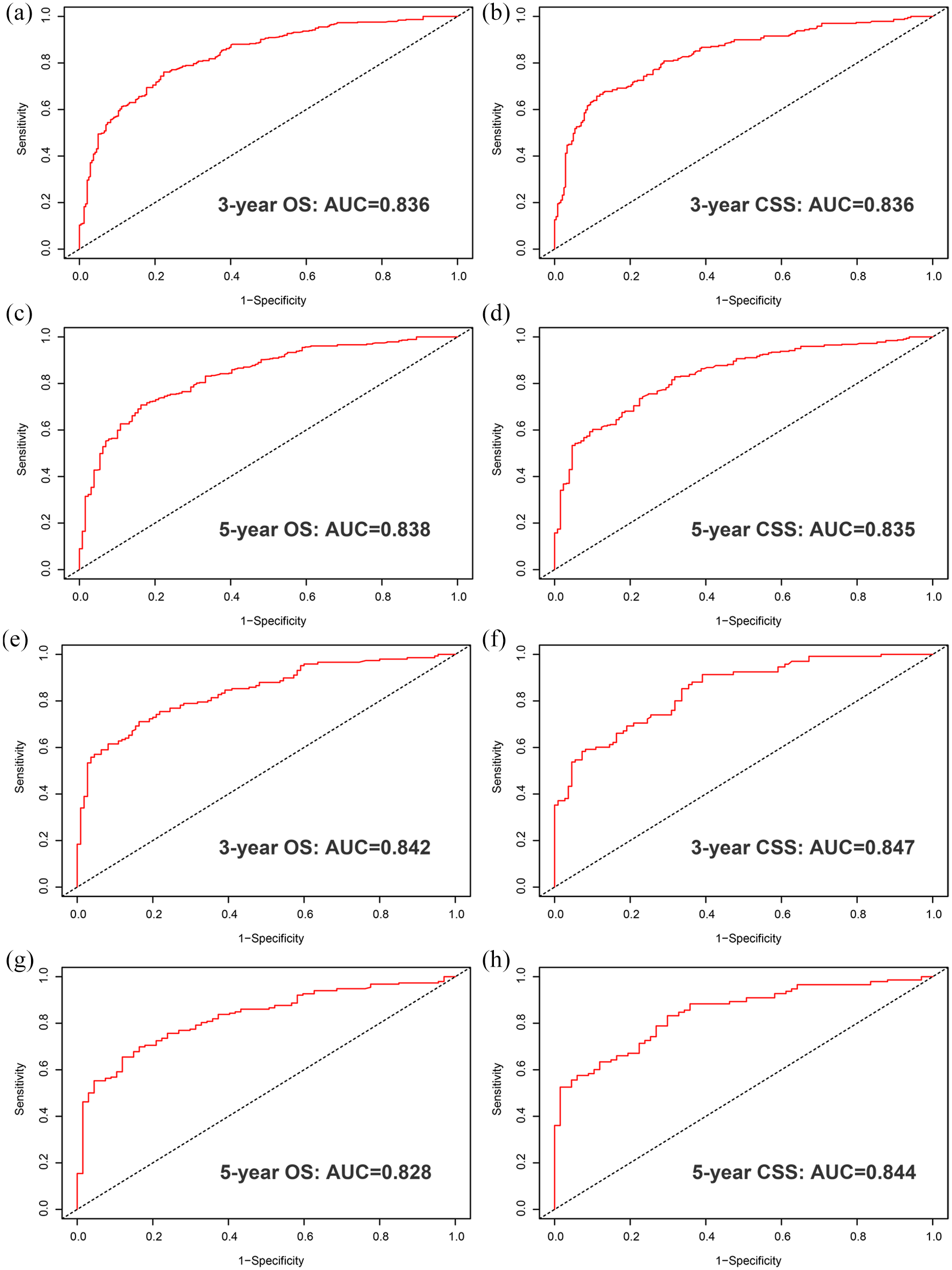
The receiver operating characteristic (ROC) curves evaluates the predictive ability of the nomogram: (a) 3-year overall survival (OS) rates in the training set; (b) 3-year cancer-specific survival (CSS) rates the training set; (c) 5-year OS rates the training set; (d) 5-year CSS rates the training set; (e) 3-year OS rates in the validation set; (f) 3-year CSS rates the validation set; (g) 5-year OS rates the validation set; (h) 5-year CSS rates the validation set.

The receiver operating characteristic (ROC) curves and decision curve analysis (DCA) evaluates the predictive ability of the nomogram: (a) overall survival (OS) rates in the training set; (b) cancer-specific survival (CSS) rates in the training set; (c) DCA curves in the training set; (d) DCA curves in the training set; (e) OS in the validation set; (f) CSS in the validation set; (g) DCA curves in the validation set; (h) DCA curves in the validation set.
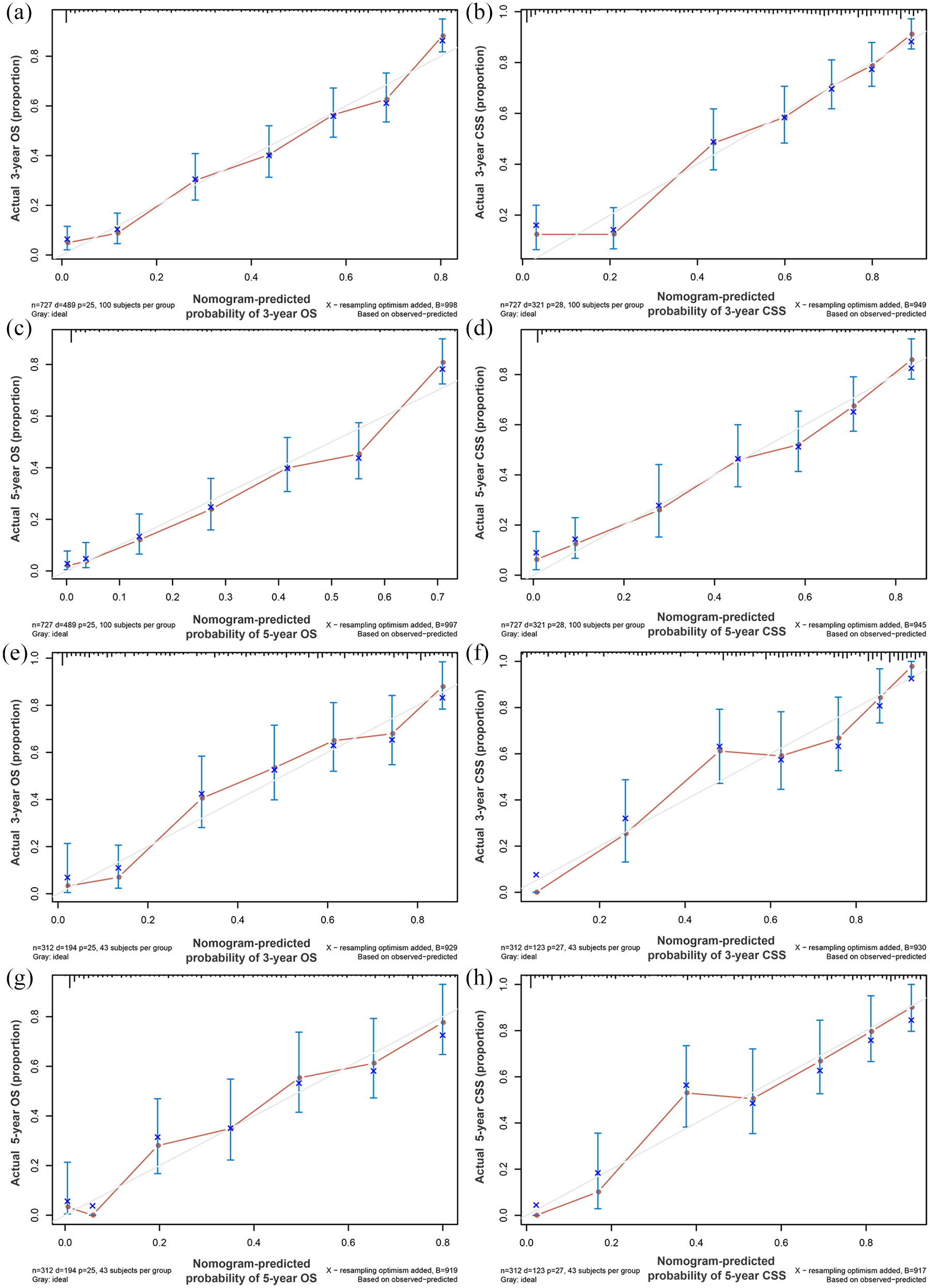
Calibration plot of the nomogram for predicting 3- and 5-year overall survival (OS) and cancer-specific survival (CSS): (a) 3-year OS rates in the training set; (b) 3-year CSS rates the training set; (c) 5-year OS rates in the training set; (d) 5-year CSS rates in the training set; (e) 3-year OS rates in the validation set; (f) 3-year CSS rates in the validation set; (g) 5-year OS rates in the validation set; (h) 5-year CSS rates in the validation set.
Discussion
In this study, we found that the incidence of ACB patients showed a decreasing trend in the past 25 years. Using the large cohort of ACB patients from the SEER dataset, two novel comprehensive nomograms were established to predict individual OS and CSS outcomes in patients with rare primary ACB. When properly used in training and validation sets, the nomogram showed satisfactory accuracy and robustness, indicating good clinical applicability for this rare genitourinary tumor.
Unlike urothelial bladder cancer, primary ACB has several particularities that should be noted. First, the low prevalence leads to a vague understanding of ACB 2 and limited experience with chemotherapy or radiotherapy. 11 El-Mekresh et al. 12 reviewed 185 patients with primary ACB and showed an overall 5-year disease-free survival rate of 55%. As for treatment, the management of primary ACB involves a multimodal approach. There are no standard guidelines for ACB, nor are there multicenter randomized controlled trials available to guide treatment decisions. Therefore, patient survival may be significantly affected by their treatment options.
Due to the rarity of primary ACB, there are no staging systems or predictive models specifically designed or widely accepted for it to date. Currently, the AJCC staging system for urothelial cancers based on T, N, and M information has also been applied to ACB. However, Natale et al. 21 reviewed 2305 patients with primary ACB from 1973 to 2015 and showed that gender, stage, grade, primary tumor location, and histological subtype have independent prognostic value. In addition, the AJCC staging system, which relies solely on pathological features, has a limited impact on the prognosis of ACB because it does not consider the impact of various treatments on the survival of patients.
The prognostic nomogram is a visualization of a complex statistical model used to predict individual survival outcomes. Prognostic nomograms have been widely used in clinical practice due to their high accuracy and comprehensibility.17,22,23 For bladder malignancies, a series of nomograms has been developed for patients with urothelial bladder cancer.24–26 Our study was based on extensive ACB data to develop a reliable prognostic prediction model for patients with primary ACB. This might be considered an update and expansion of the previously published studies that also used population-based data, but instead establishes a reliable prognostic prediction model for patients with primary ACB. 21
Numerous studies proved that female patients were associated with higher cancer-specific mortality in urothelial bladder cancer.27–29 The role of gender in predicting prognosis of ACB patients seemed to be completely different from that of patients with primary small-cell carcinoma (SCC) of the bladder. Such disparity might be a reflection of differences between ACB and SCC in genetic, hormonal, societal, and environmental factors, which all had significant impact on gender-related cancer prognosis.30,31 Moreover, this is the first time that marital status was introduced to primary ACB’s prognostic nomogram. This study indicates that marriage can bring prognostic differences, so this is worthy of more attention as marriage may include complicated mechanisms that improve OS.
The recommended nomogram included three treatment factors: radical cystectomy, chemotherapy, and radiotherapy, which perform well in predicting the survival outcomes of ACB patients. Among all therapies, radical cystectomy remains the standard of treatment for ACB, and chemotherapy as adjuvant or neoadjuvant therapy appears to remain the primary treatment for patients with ACB. The 2019 National Comprehensive Cancer Center Network guidelines for patients with advanced or metastatic ACB recommend chemotherapy. However, some study protocols showed poor response rates in ACB.32,33 It has been found that this and postoperative radiotherapy may have a role in improving disease-free survival, especially in the early stages. 12 From our study, we found that radiotherapy appears to be a completely independent prognostic factor for OS, rather than CSS, and that patients who received radiotherapy had a higher overall mortality rate compared with those who did not, a result similar to that of Natale et al. 21 We suspect that for some patients, it is too late for cystectomy, or the body is unable to tolerate anesthesia, and these patients simply choose to preserve their bladder and receive radiotherapy, thereby increasing overall mortality.
Generally speaking, the new nomograms in our research are innovative in several ways. First, we created OS and CSS prognostic nomograms for patients with ACB, making personalized prognostic prediction possible. Second, we found that the current AJCC stage or TNM stage of bladder cancer is actually less appropriate for primary ACB. Therefore, we established a new aggregation-based nomograms system and further demonstrated that the newly established nomograms can easily stratify patients into different risk strata. Finally, and most importantly, we used DCA curve, a relatively new method of analyzing net benefit; we applied it to our nomograms and found that the new nomograms have broader clinical applicability than the current TNM staging.
However, there are still several limitations. First of all, our analysis is based on the SEER database, which lacks some accurate information. For example, assigning two categories to chemotherapy (“No/Unknown” or “Yes”) may lead to limitations in the completeness of the variables and might cause other relevant bias. Second, the SEER database does not include the socioeconomic status of individuals, 34 such as education level and household income level, which may also be related to the prognosis of bladder cancer patients. 35 As for the establishment of nomograms, improving the accuracy of the model sometimes comes at the cost of increased complexity. It is not easy to strike a balance between comprehensibility and comprehensiveness. This is a common problem when developing new nomograms. Furthermore, although the C-index of the two nomograms is greater than 0.7, it shows that the accuracy of OS and CSS is indeed very high, but not perfect. The quality and quantity of data and the reliability of the algorithm can still be improved, and the nomograms would need to be tested in other cohorts. In addition, the study was conducted retrospectively, and there may be selection bias.
Conclusions
Over the past 25 years, the incidence of patients with primary ACB has shown a decreasing trend. Based on the results of multivariate Cox regression analysis, we constructed a clinically useful prognostic nomogram for assessing OS and CSS in patients with ACB, superior to the traditional TNM staging system, which provides personalized risk assessment for ACB patient survival.
Supplemental Material
sj-tif-1-tau-10.1177_17562872211018006 – Supplemental material for Trends of incidence and prognosis of primary adenocarcinoma of the bladder
Supplemental material, sj-tif-1-tau-10.1177_17562872211018006 for Trends of incidence and prognosis of primary adenocarcinoma of the bladder by Haowen Lu, Weidong Zhu, Weipu Mao, Feng Zu, Yali Wang, Wenchao Li, Bin Xu, Lihua Zhang and Ming Chen in Therapeutic Advances in Urology
Footnotes
Acknowledgements
The authors are grateful for the invaluable support and useful discussions with other members of the urological department.
Author contributions
Conception and design: HL, WM, MC, LZ, and BX; Administrative support: WZ, WM, and BX; Provision of study materials or patients: HL and YW; Collection and assembly of data: HL, WM, and YW; Data analysis and interpretation: HL, WZ, WM, and FZ; Manuscript writing: HL, WC, WM, and WL. Final approval of manuscript: All authors.
Availability of data
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant numbers 81572517 and 81872089), Natural Science Foundation of Jiangsu Province (grant number BK20161434), Jiangsu Provincial Medical Innovation Team (grant number CXTDA2017025), Jiangsu Provincial Medical Talent (grant number ZDRCA2016080), and the Scientific Research Foundation of Graduate School of Southeast University (grant number YBPY2173).
Ethical approval
The SEER database consists of de-identified information that is freely available within the public domain, so ethical approval was not required.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.