
Abstract
Purpose:
The lack of available guidelines for the management of prostatic abscess (PA) results in inconsistencies in its management. The most commonly used management modalities were conservative treatment with parenteral antibiotics alone, transrectal ultrasound-guided (TRUS) needle aspiration, or transurethral deroofing (TUD).
The current study is a retrospective study and examines prostatic abscess cases treated by either one or more of the different modalities. We assess and compare presentation, diagnosis, management, and outcomes of prostatic abscess and we compare the outcomes of the three management modalities.
Methods:
We retrieved the records of all patients (n = 23) admitted to the Urology department at Al Wakra hospital with the computed tomography (CT) diagnosis of prostatic abscess from January 2013 to March 2018. Data collected included demographic, clinical, laboratory, and imaging findings, as well as management modality, duration of hospital stay, duration of follow up, outcome, and recurrence.
Results:
A total of nine (39.1%) patients had conservative treatment only; eight (34.8%) had TUD, and six (26.1%) had TRUS needle aspiration. The mean age was 52.7 years. Lower urinary tract symptoms and fever were the most common presentations (95.7% and 82.6%, respectively). CT scan of the abdomen and pelvis with contrast was undertaken for all patients and it showed that multiple abscesses were observed in 14 (60.9%) cases.
The overall mean hospital stay was 8.45 days (range 2–21 days). We observed no recurrences for patients treated conservatively or those who undertook TUD, but three patient (50%) recurrences were noted in TRUS aspiration patients. There was no mortality across the sample.
Conclusion:
Early diagnosis of prostatic abscess and prompt management may have decreased the morbidity and mortality. Conservative management can succeed in subcentimeter abscesses but TUD is the definite therapy for large and multiloculated abscess. TRUS aspiration does have a role in treatment, but it has higher recurrence and longer hospital stay.
Introduction
Prostatic abscess (PA) is a complication of acute bacterial prostatitis 1 or hematogenous spread of infection. 2 Mortality ranges from 1–16% 3 and high-risk groups include immune compromised and diabetic patients, those with chronic kidney disease or on hemodialysis, and patients with cirrhosis or indwelling catheter.4,5 The diagnosis of PA is challenging owing to its wide range of local and systemic signs and symptoms. Early diagnosis depends on a high index of suspicion, clinical and laboratory evidence of severe infection or sepsis, and is confirmed by either transrectal ultrasound, 6 computed tomography (CT) scan7,8 and in inconclusive cases, magnetic resonance imaging (MRI). 9 Treatment options include either solo conservative treatment or its combination 4 with surgical transrectal ultrasound-guided (TRUS) needle aspiration 10 or transurethral deroofing (TUD) of PA. 6 To date, no available international consensus guidelines for diagnosis and management of PA exists. 3
The lack of available guidelines for the management of PA results in inconsistencies in its management across centers and countries, and across the conservative medical or surgical treatment options. To the best of our knowledge, only two studies compared the conservative medical or surgical treatment modalities of PA.11,12 One study compared the two surgical treatments (TRUS versus TUD), 11 their use, and their outcomes. Likewise, only one study compared the three treatment modalities (conservative versus TRUS versus TUD), the use of each, and their outcomes. 12 This is despite the fact that PA is a potentially life threatening condition that could progress to sepsis and death if accurate diagnosis and appropriate treatment are delayed. 13
Given the lack of an evidence base to guide the diagnosis and choice of the three management modalities of PA, therefore, the current study examined 23 PA cases treated by either one or more of the different modalities. We compared the demographic (age), clinical [number/types of comorbidities, presenting symptoms, digital rectal examination (DRE) data], and culture (urine, blood) data, as well as inflammatory markers [white blood cells (WBC), C-reactive protein (CRP), procalcitonin], imaging (ultrasound, CT), urinary catheter data, duration of follow up, and outcomes [length of hospital stay (LOS), recurrence, mortality]. The aim was to assess the treatment options of PA considering the patient’s general condition and the particular features of the abscess. For each of the three management modalities of PA, the specific objectives were to:
(1) Assess and compare the demographic, clinical, culture, inflammatory markers, imaging, urinary catheter data, and duration of follow-up findings;
(2) Assess and compare the outcomes;
(3) Assess the predictors of hospital stay among patients.
Methods
Ethics and sample
The Medical Research Centre at Hamad Medical Corporation (HMC) approved this retrospective study (Protocol # MRC-01-18-167). We searched and retrieved the electronic medical records of all patients (n = 23) admitted to the urology department at Al Wakra hospital (Al Wakra city) with the CT diagnosis of prostatic abscess during the study period (January 2013–March 2018). Data collected included demographic (age), clinical (number and types of comorbidities, presenting symptoms, DRE), laboratory (WBC, CRP, procalcitonin, blood, urine cultures), and imaging (CT, transabdominal ultrasound) findings, as well as management modality, duration of hospital stay, duration of follow up, outcome, and recurrence.
Management modalities of prostatic abscess
Conservative treatment consisted of broad-spectrum parenteral antibiotics, followed by specific antibiotic/s based on culture and sensitivity results. 4
Needle aspiration consisted of TRUS needle aspiration in addition to broad spectrum parenteral antibiotics, followed by specific antibiotic/s based on culture and sensitivity results. 10
TUD consisted of TUD and drainage in addition to broad spectrum parenteral antibiotics, followed by specific antibiotic/s based on culture and sensitivity results. 6
Procedures
PA diagnosis was established based on clinical history, physical examination, and laboratory investigations, and CT scans confirmed the diagnosis. All patients were admitted, septic work ups were sent to the laboratory, and patients were started on empirical intravenous antibiotics as per our department’s protocol (100 mg piperacillin/12.5 mg tazobactam per kg body weight/every 8 h, and amikacin 15 mg/kg body weight daily with dose adjustment in patients with renal impairment). Based on the findings of the investigations and the patient’s general condition, triage of patients was undertaken. For stable patients with small abscess/es, antibiotics alone were administered; for those with large single PA or those who cannot tolerate anesthesia, TRUS needle aspiration was undertaken; and, for those with large, multiloculated PA, TUD was conducted. Patients with urine retention were kept on urethral catheter if it was already inserted in the emergency department, otherwise suprapubic catheter was inserted. TRUS aspiration was done under local or spinal anesthesia (subject to patient’s general condition),14,15 whereas TUD was undertaken under general or spinal anesthesia. 16
Daily follow up included assessment of vital signs and evaluation of the laboratory results including Complete Blood Count (CBC) and CRP. Urine and blood culture results were reviewed and antibiotics were adjusted according to the sensitivity findings. Patients were kept in hospital until afebrile for 48 h, their leukocytosis had normalized, and had a negative blood culture. For patients not responding to the initial management pathways described above, reimaging was undertaken (transabdominal ultrasound or CT scan) and management was further planned based on the findings. Patients were discharged on antibiotics for 4–6 weeks. Follow up at the clinic was after 2 weeks where laboratory investigations were done, either transabdominal or transrectal ultrasound imaging undertaken in order to ensure non recurrence of the PA, and the catheter was removed. The patient’s general condition, laboratory findings, and follow-up imaging were used as indicators of success of treatment.
Statistical analysis
Descriptive statistics were used to summarize and determine the sample characteristics and distribution of the parameters related to demographic, clinical, culture, inflammatory markers, imaging, urinary catheter data, and follow-up findings across the three management modalities. Quantitative data were reported as mean and standard deviation (SD); categorical data were summarized using frequencies and percentages.
Differences in quantitative outcome measures between the three treatment modalities were compared using one-way analysis of variance (ANOVA). Associations between two or more qualitative variables were assessed using chi-square (χ2) test or Fisher exact test as appropriate. Pearson’s correlations examined linear relationships between two or more quantitative variables. Multiple regression analysis assessed the impact of the different predictors and factors of hospital stay among prostatic abscess patients. All p values presented were two-tailed, and p values < 0.05 were considered as statistically significant. All statistical analyses were done using statistical packages SPSS 22.0 (SPSS Inc. Chicago, IL) and Epi-info (Centers for Disease Control and Prevention, Atlanta, GA) software.
Results
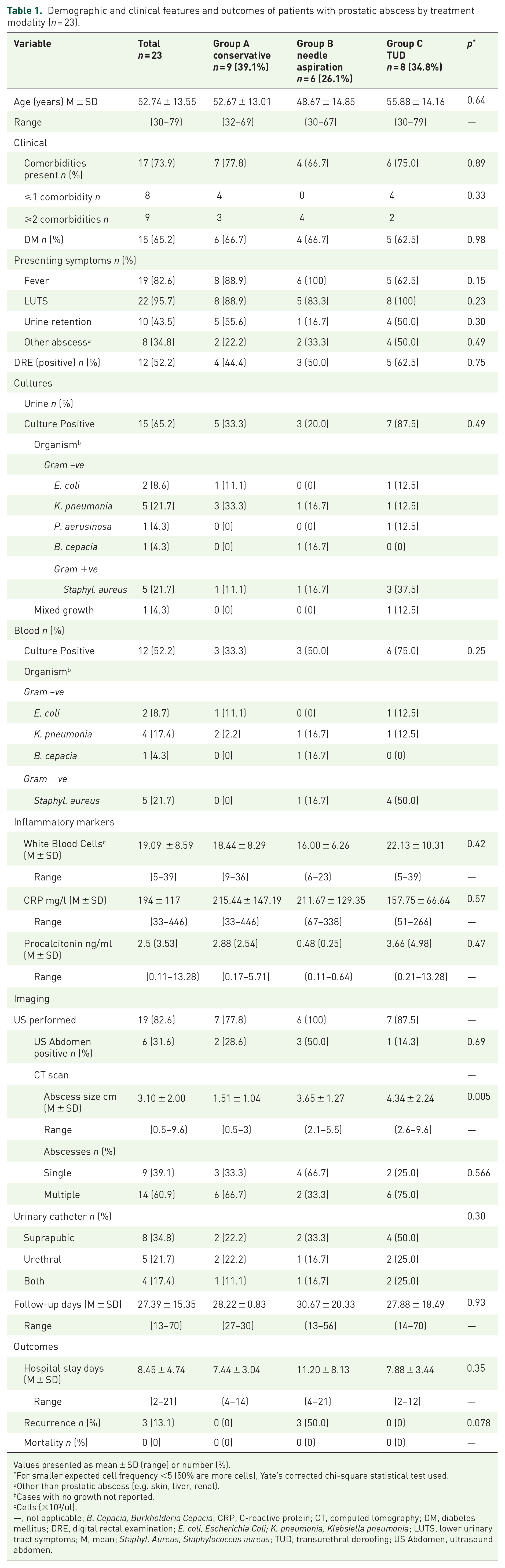
Table 1 shows the demographic and clinical features of patients with prostatic abscess (PA) by treatment modality. A total of nine (39.1%) patients had conservative treatment only, eight (34.8%) had TUD, and six (26.1%) had TRUS aspiration. Mean age at the time of diagnosis was 52.7 years, and 65.2% were diabetics. There were no significant differences in age and diabetic status across the three treatment modalities. Lower urinary tract symptoms and fever were the most common presentations (95.7% and 82.6%, respectively). Presenting symptoms were not significantly different across the three treatment modalities. DRE was positive in 52.2% of the patients and not significantly different across the treatment modalities.
Demographic and clinical features and outcomes of patients with prostatic abscess by treatment modality (n = 23).
Values presented as mean ± SD (range) or number (%).
For smaller expected cell frequency <5 (50% are more cells), Yate’s corrected chi-square statistical test used.
Other than prostatic abscess (e.g. skin, liver, renal).
Cases with no growth not reported.
Cells (×103/ul).
—, not applicable; B. Cepacia, Burkholderia Cepacia; CRP, C-reactive protein; CT, computed tomography; DM, diabetes mellitus; DRE, digital rectal examination; E. coli, Escherichia Coli; K. pneumonia, Klebsiella pneumonia; LUTS, lower urinary tract symptoms; M, mean; Staphyl. Aureus, Staphylococcus aureus; TUD, transurethral deroofing; US Abdomen, ultrasound abdomen.
With regards to microbiology, Table 1 depicts that 65.2% of patients had positive urine cultures, with gram negative bacteria identified more than gram positive bacteria. Blood cultures were positive in 52.2% of cases, and for laboratory inflammatory markers 86.9% had leukocytosis, all cases had elevated CRP, and 30.4% had high procalcitonin (data not presented).
In terms of imaging, transabdominal ultrasound was done for 19 patients, of which 31.6% were positive; CT scan abdomen and pelvis with contrast was undertaken for all patients and MRI pelvis was necessary for only four (17.40%) patients where CT scan findings were inconclusive (data not presented). Multiple abscesses were observed in 14 (60.9%) cases (mean PA size 3.1 cm). Two cases of multiple abscesses were treated by TRUS aspiration, in which there was one large abscess, surrounded by smaller, tiny abscesses. There were no significant differences in number of abscesses across three treatment modalities. Suprapubic catheter was inserted for eight (34.8%) patients, urethral catheter for five (21.7%), both catheters (sequential) for four (17.4%), and six (26.1%) patients required no catheter.
As for the outcomes, overall mean hospital stay was 8.45 days (range 2–21 days) with no significant differences across the three treatment modalities. We observed no recurrences for patients treated conservatively or those who undertook TUD. Recurrences were noted only in TRUS aspiration patients where three (50%) patients had recurrence and were effectively treated with TUD, which accounted for their prolonged hospital stay. There was no mortality across the sample.
The independent factors (abscess size, treatment modality, DM, and CRP) that could affect LOS were examined using multiple linear regression analysis. These variables were selected as predictors as they are clinically significant to practice and were also statistically significantly correlated with the LOS (data not presented). We found no meaningful independent factors that could predict LOS (Table 2).
Linear regression analysis: predictors of hospital stay among patients with prostatic abscess.
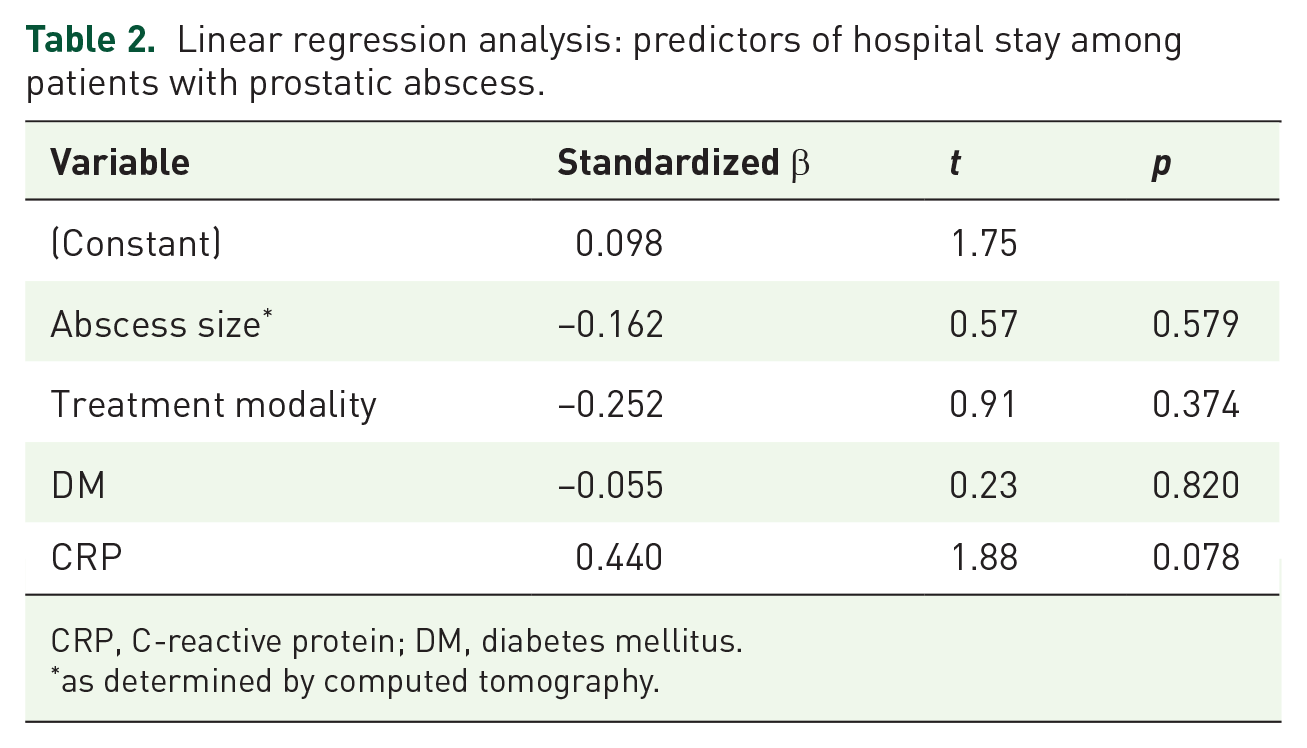
CRP, C-reactive protein; DM, diabetes mellitus.
as determined by computed tomography.
Discussion
Despite the fact that mortality from PA ranges between 1% and 16%, 3 to date, there exists no standardized clinical diagnostic criteria or international guidelines for treatment of PA. 17 Some research suggested an algorithm approach for treatment of PA. 3 To the best of our knowledge, only two studies compared the treatment modalities of PA, their use, and outcomes,11,12 where only one of them compared the three modalities. 12 The current study assessed and compared the three management modalities of PA in terms of their demographic, clinical, culture, inflammatory markers, imaging, urinary catheter data, duration of follow up, and outcomes (LOS, recurrence, mortality). The study also assessed the predictors of LOS of the three management modalities.
The presenting symptoms were classical and not significantly different across the three treatment modalities. Tender enlarged prostate with fluctuation upon DRE was noted in 52.2% of our cases, lower than others who reported 70%. 17 Overall mean hospital stay was 8.45 days (range 2–21), with no significant differences in mean hospital stay across the three treatment modalities. Recurrence was observed only in three out of the six TRUS aspiration patients, with no recurrence in patients who were managed conservatively or TUD patients. There was no mortality across the sample.
The most commonly used treatments of PA include parenteral broad-spectrum antibiotics with or without abscess drainage through ultrasound-guided needle aspiration of pus or TUD of abscess.3,11,12,18 No clear guidelines address how treatments are titrated to individual patients. One algorithm addressed the choice of management modality, 3 suggesting conservative treatment for PA < 1 cm, TRUS needle aspiration for PA > 1 cm, or failed conservative management, with TUD reserved for failed TRUS needle aspiration. Our triage and classification of patients is in partial agreement with such algorithm where we undertook conservative management for non-critically ill patients with few comorbidities who have small sized abscess/es. We conducted minimally invasive therapy with TRUS needle aspiration for single large PA or for patients who cannot tolerate anesthesia, and TUD was utilized for patients with multilocular large abscesses (either single or multiple). The advantage of such approach is that the patient’s general condition and stability are considered, as critically ill patients cannot tolerate any delays spent on conservative management. Likewise, for multi-locular PA patients, needle aspiration may not be effective as there is need to deroof the whole abscess.
In terms of modalities, a unique point of the current study is that about 40% of cases were successfully treated conservatively with intravenous antibiotics with or without suprapubic drainage as the PA was mostly subcentrimetric in size. Our 40% conservative treatment was higher than others who used conservative treatment in only 21% of their patients. 12 Perhaps our higher rate of conservative treatment can be attributed to early diagnosis and time start of the conservative management based on the high index of clinical suspicion by the available hospital urologist. In our sample, 34% of patients had TUD with or without resection of prostate for multilocular large abscesses. The remaining 26% had TRUS needle aspiration for patients with single abscess or those who could not tolerate anesthesia, of which three (50%) patients had recurrence of PA which was effectively managed by TUD. Others reported higher rates, where 44% of patients underwent TUD and 35% had TRUS needle aspiration. 12 Such differences are probably attributed to differences in patients’ profiles and size of abscesses, two features that contribute significantly to the choice of treatment modality in PA.
As for recurrences, we observed no recurrences for the nine conservatively managed patients, in agreement with others.2,12 We also observed no recurrences for the eight TUD patients, in support of other research, 12 but in contrast with a study that reported 4% recurrence rate after TUD, attributed to large multilocular abscesses. 11 We observed recurrences in three out of the six TRUS aspiration patients; these three patients were effectively treated with TUD, and hence had a prolonged hospital stay. Others have observed a 22% 12 and 31.6% 11 recurrence rate after TRUS needle aspiration.
In connection with LOS, our TRUS needle aspiration LOS of 11.20 ± 8.13 agreed with the 12.5 days reported by others, 11 but was much shorter that the 23.25 described by Jang et al. 12 Our TUD patients had about 7.9 days LOS, comparable with other studies (range 6.1–10.22 days).11,12 Our conservatively treated patients had short LOS (7.44 days), much shorter than the LOS reported by others for conservatively treated patients (19 days). 12 Generally, our shortest LOS was for conservative management, followed by TUD and then TRUS needle aspiration. The optimal drainage achieved by generous deroofing of the abscess cavities during TUD might explain the faster recovery and shorter LOS. Longer LOS for TRUS needle aspiration is attributed to recurrences that required additional TUD intervention and follow up. Although there is increase in LOS in TRUS needle aspiration patients compared with TUD patients,11,12 we found no statistically significant differences in LOS across treatment modalities. Average LOSs in previous studies were 10.23 and 17.5 days;11,12 our mean LOS was 8.45 days.
In terms of mortality, there was no mortality across our 23 patients, in contrast to previously reported mortality that ranged from 1% to 16%. 3 Likewise, others reported two mortalities (3.8%) due to sepsis in 71 and 76-year-old patients who underwent conservative management. 12 The possible reasons for our zero mortality and shorter LOS is attributed primarily to our undertaking of laboratory inflammatory markers and CT scan for all cases, resulting in prompt diagnosis of PA based on a high index of clinical suspicion by the urologist who is immediately contactable by the emergency physician. The outcomes of such actions were fruitful as many patients could hence be treated conservatively. Other modalities were also timely executed subject to the extent and severity.
To the best of our knowledge, the role of laboratory inflammatory markers, for example leukocytosis, CRP, procalcitonin, and lactic acid, in the diagnosis and follow up of patients with PA have not been reported so far. In the current study, leukocytosis, CRP and procalcitonin were used in the diagnosis, treatment, prognosis, and to monitor the recurrence. CRP was a statistically significant predictor of the LOS. Future research could address this gap in the evidence base.
The current study has limitations. It is a retrospective study with its inherent limitations (e.g. potentially missing patients, data may have some reporting bias). Larger scale studies could more precisely define the outcomes, with a large number of patients in each treatment modality to overcome the limitations of small sample size. Despite such limitations, the current study is one of the very few studies that addressed the baseline characteristics, diagnostic tools used, management, and outcomes of each treatment modality.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Publication was supported by funding from the Medical Research Center, Hamad Medical Corporation, Qatar.
Conflict of interest
The authors declare that there is no conflict of interest.