
Abstract
A prostate abscess is a rare complication of prostatitis, typically observed in patients with conditions such as immunodeficiency, diabetes, urinary tract abnormalities, and chronic indwelling catheters. We present a 60-year-old patient, admitted to the hospital presenting progressively with dysuria for more than 1 year, accompanied by frequent urination, urgent pain, and urinary retention, intermittent fever for 20 days. A multi-parametric magnetic resonance imaging (mpMRI) scan of the abdomen/pelvis showed a prostatic abscess. Initially, meropenem treatment was not effective. Subsequently, the patient underwent an artificial intelligence-assisted mpMRI-TRUS (transrectal ultrasonography) real-time-guided puncture drainage. The results of purulent drainage cultures were positive for K. pneumonia, sensitive to bacillosporin. Thus, the combination treatment of sensitive antibiotics and transperineal drainage was conducted. The patient was followed up for 6 months, the outcome was satisfactory. Timely and appropriate treatments (such as the combination of sensitive antibiotics and artificial intelligence-assisted mpMRI-TRUS real-time-guided transperineal puncture drainage) are crucial for both patient survival and the prevention of complications.
Keywords
Introduction
A prostate abscess is a rare inflammatory disorder of the prostate, accounting for ~0.5% of prostate diseases and having a fatality rate of 1%–16%. 1 Diabetes mellitus, hepatic and renal insufficiency, invasive surgical procedures on the urinary tract, and immunosuppression are the main predisposing factors for this disease. 2 Treatment requires consideration of patients’ condition and infected strain. A prostate abscess is primarily attributed to Escherichia coli or Klebsiella pneumoniae infection.3,4 We report a 60-year-old male patient with progressive urination difficulties for >1 year and aggravation for 20 days. After three times urinary catheter insertions in a local hospital, an MRI revealed a prostatic abscess. The patient was treated with perineal artificial intelligence (AI)-assisted multi-parametric magnetic resonance imaging-transrectal ultrasonography (mpMRI-TRUS) real-time-guided puncture drainage, combined with sensitive antibiotics, achieving a satisfactory outcome.
Case presentation
The patient presented with urinary retention and intermittent fever lasting 20 days. Symptoms worsened after repeated catheter insertions at a local hospital. During this period, the highest temperature reached 39°C. The urethral tube was retained for further diagnosis and treatment. The patient’s history included cirrhosis of the liver, ascites for 3 years, and diuretic treatments. Upon admission, examinations disclosed a temperature of 36.5°C, pulse of 82 times/min, respiration of 20 breaths/min, and blood pressure of 92/61 mmHg. Rectal examination indicated a prostate enlarged to degree III, with a vanished central groove, tough texture, and increased anal sphincter muscle tone. Laboratory tests revealed elevated C-reactive protein, blood leukocytes, and decreased albumin and potassium. Prostate-specific antigen was normal, and urine cultures were negative. MRI showed prostatic hyperplasia with possible prostatic abscess and involvement of seminal vesicle glands, rectal wall, and neurovascular bundle (depicted in Figure 1). Prostate cancer was not excluded. The admission diagnosis was prostatic hyperplasia, prostatic abscess, possible tumor, alcoholic cirrhosis in the decompensated stage, pyoperitoneum, hypokalemia, and hypoproteinemia. The patient underwent mpMRI-TRUS-guided puncture drainage assisted by AI. Purulent drainage cultures were positive for K. pneumoniae, sensitive to bacillosporin. The patient was treated with a combination of sensitive antibiotics and transperineal drainage.

Preoperative multi-parametric MRI of the prostate gland suggests multiple abscesses in the prostate gland, as marked by the white arrow.
During the surgical procedure, the mpMRI image was introduced into the VENUS multimodal AI image fusion ultrasound system, where the AI intelligently identified the prostate morphology, and the lesion location of the prostate target area was manually delineated (depicted in Figure 2(a)). Initially, the prostate abscess cavity was punctured and decompressed, extracting approximately 80 ml of pus from the cavity (depicted in Figure 2(b)). Subsequently, two F10 drainage tubes were inserted into the larger pus cavities of the left and right lobes to facilitate continuous drainage. Furthermore, biopsy needles were inserted into regions suspected of containing substantive nodules based on MRI findings. Then, a cystostomy urinary catheter was inserted, and the original urethral catheter was removed. The postoperative pathology report disclosed the presence of fibrous connective tissue, muscular tissue, fibrous tissue, and foamy histiocyte hyperplasia, along with inflammatory cell infiltration dominated by lymphocytes and neutrophils. These findings were in accordance with prostatic abscess and prostatic hyperplasia (depicted in Figure 2(c)).
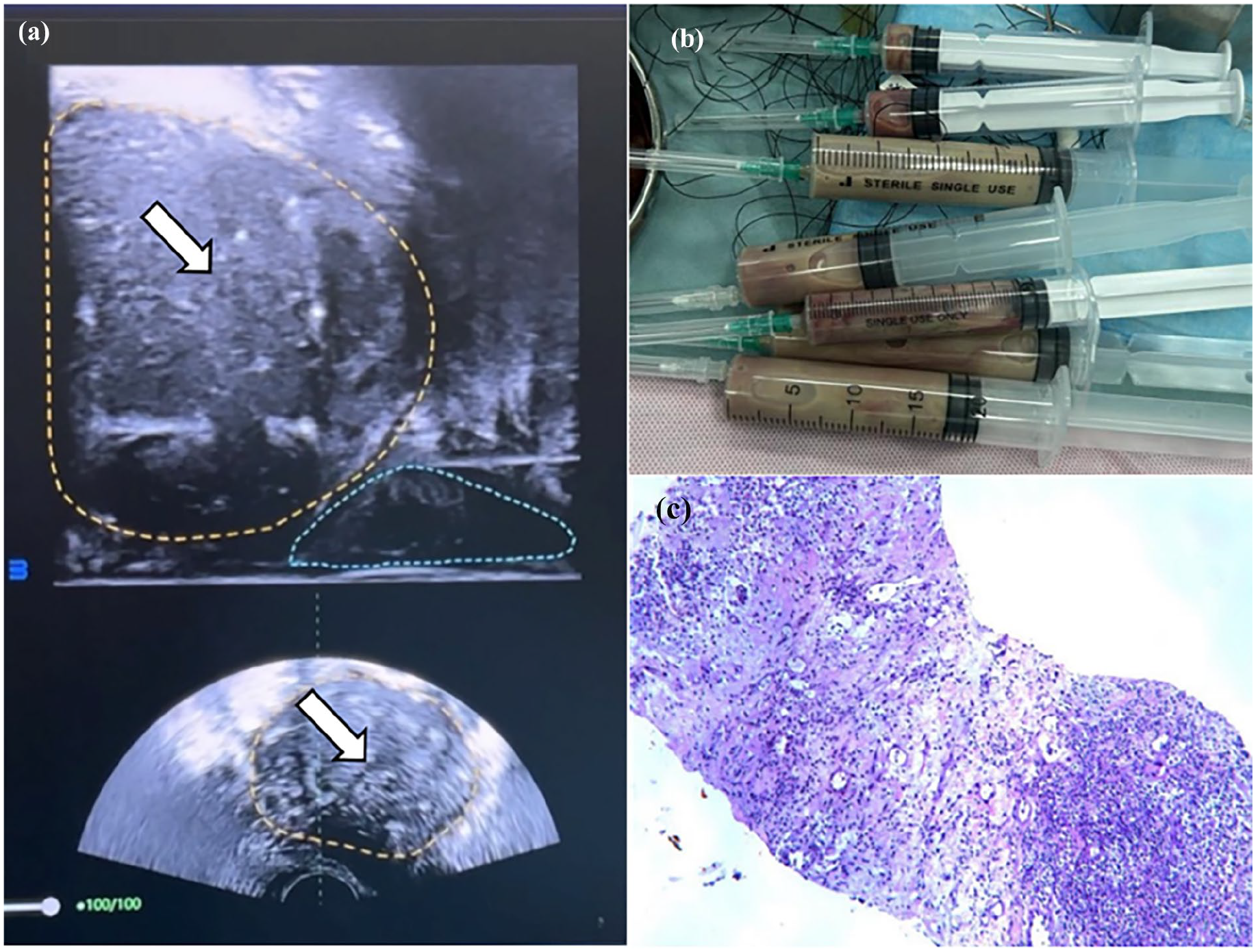
Real-time fusion of mpMRI-TRUS images assisted by AI. (a) The yellow dashed area represents the morphology of the prostate envelope identified by AI, while the white arrow represents the area of the pus cavity identified by AI. (b) About 80 ml of pus was extracted intraoperatively. (c) Postoperative pathology report suggests prostatic abscess and prostatic hyperplasia.
Postoperatively, the patient showed improvement in chills. Analysis of the pus drainage fluid culture identified K. pneumoniae. Based on drug sensitivity results, polymyxin was administered to control the infection, and the patient did not have further fever. Postoperative prostate computed tomography (CT; depicted in Figure 3) indicated that the prostate abscess cavity had almost vanished, with only a small amount of pelvic fluid remaining. Consequently, the abscess drainage tube was removed. Four weeks later, the cystostomy tube was removed, and the patient was prescribed finasteride + tamsulosin for prostatic hyperplasia. He was capable of urinating independently and remained asymptomatic for 6 months.

Postoperative prostate computed tomography scans have demonstrated that the abscess cavity has almost resolved, with minimal pelvic effusion observed.
Discussion
The occurrence of prostate abscess is rare and it is mainly attributed to E. coli or K. pneumoniae infection.3,4 Diabetes mellitus, hepatic and renal insufficiency, invasive surgical procedures on the urinary tract, and immunosuppression are the primary predisposing factors for this disease.2,5 In the current case, the patient was in the decompensated phase of liver cirrhosis and had a previous history of acute urinary retention with recurrent catheterization, which is in line with existing literature.
Patients diagnosed with prostate abscess commonly undergo systemic discomfort, including fever. In addition, they frequently encounter symptoms related to urinary tract irritation, perineal discomfort, and difficulty in urinating.5–7 Rarely, patients might also encounter abnormal penile erection, hematuria, and lumbar or dorsal pain. If the abscess ruptures in the urethra, a considerable amount of purulent discharge may be observed. According to studies, 66.7% of prostate abscess patients exhibit a palpable fluctuating sensation during rectal examination.8,9 If patients suspected of having acute bacterial prostatitis fail to show improvement after 36 h of standardized treatment, it is recommended to conduct a rectal ultrasound to assess the presence of a prostate abscess.1,10 MRI is the most reliable imaging modality for diagnosing prostate abscesses and is highly valuable in determining the presence of infection in tissues surrounding the prostate or in conjunction with other abscesses. 11 In this particular case, the patient presented with high fever, chills, perineal tenderness, and an enlarged prostate gland upon rectal palpation, with no obvious fluctuating sensation. The diagnosis was subsequently confirmed through a combination of MRI and other diagnostic tests.
The morbidity and mortality of prostate abscesses have declined with the widespread use of antibiotics. After receiving treatment with anti-infective drugs and undergoing surgical drainage, most patients have a favorable prognosis. However, there is a risk of recurrence. 1 The treatment of a prostate abscess is classified into conservative drug treatment and surgical treatment. Currently, surgical treatment is the primary clinical treatment for prostate abscesses. Antibiotic treatment is also necessary as an adjunctive therapy. Some studies have indicated that microabscesses of the prostate (<1 cm) can be cured with antibiotic treatment alone, without surgical intervention.1–3 Surgical procedures include transperineal puncture and drainage, transrectal puncture and drainage, and transurethral decortication and drainage.7,12 These procedures are typically severe under general or lumbar anesthesia. In this case, the patient had multiple abscesses in the prostate gland and infectious shock. Due to the severity of the condition and the difficulty of tolerating general anesthesia, we employed AI-assisted, real-time fusion-guided magnetic ultrasound transperineal perineal prostatic abscess puncture and drainage under local anesthesia. The results were encouraging due to the following factors:
MRI image fusion precise puncture techniques mainly comprise mpMRI-TRUS cognitive fusion-targeted puncture, AI software fusion targeted puncture, etc. The cognitive fusion-targeted puncture process is significantly affected by the subjective factors of the operator and the film reading level, which may result in missed diagnosis in diagnosis. 13 Different from cognitive fusion, for the treatment of this patient, we utilized the built-in software of the multimodal AI image fusion ultrasound system to intelligently fuse the mpMRI and TRUS images, reducing the operator’s requirements for the mpMRI image film reading ability and enhancing the accuracy of targeted puncture. 13 This combination ensured a high puncture success rate and minimized the risk of injuring surrounding prostate tissues. It also guaranteed complete drainage.
Transperineal puncture, compared to rectal puncture, decreased the risk of rectal urethral fistula complications. This approach minimized postoperative defecation, eliminated the need for fasting, and facilitated nutritional therapy for faster recovery. The trauma associated with transperineal puncture and drainage was relatively minor, enabling the use of local anesthesia only.12,14,15 This approach lowered anesthesia risks, particularly crucial for patients with preoperative hypotension or shock.14,15 MRI imaging of the prostate revealed the presence of an abscess and the necessity for a biopsy during the transperineal puncture and drainage procedure. With the development of AI software image fusion technology, multimodal image fusion-targeted puncture has significantly improved the detection rate of clinically significant prostate cancer. 14 In the future, AI will also play a role in fields such as disease monitoring, diagnostic assistance, and medical education. 16 Overall, the AI-assisted, real-time fusion-guided magnetic ultrasound approach offered a safe and effective method for prostatic abscess puncture and drainage, minimizing risks, and promoting patient recovery.
Conclusion
A prostatic abscess is an uncommon yet severe urological ailment. Its initial symptoms lack specificity, necessitating prompt diagnosis of suspected cases with concomitant prostate abscess predisposition factors via transrectal ultrasound, CT, and MRI. In terms of treatment, mpMRI-TRUS real-time-guided transperineal abscess puncture drainage assisted by AI offers numerous benefits, including complete drainage, superior accuracy, reduced complications, alleviated patient discomfort, accelerated recuperation, minimal invasiveness, and concurrent prostate biopsy.
Footnotes
Acknowledgements
The authors gratefully acknowledge the financial support provided by the National Key Research and Development Program of China & Hunan Provincial Inclusive Policy and Innovative Environment Construction Plan.
Author contributions
Y.W. and Y.Y. conceived the study and wrote the main manuscript. X.H. and C.W. collected the data and performed the literature search. Y.L. participated in the treatment of this patient. Q.L. provided financial support and revised the thesis. All authors reviewed the manuscript, and all authors approved the final version for submission.
Data availability statement
No datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by the National Key Research and Development Program of China (2021YFC2009300) and Hunan Provincial Inclusive Policy and Innovative Environment Construction Plan (2020Sk50902).
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.