
Abstract
Background:
Owing to the improved vision and instrument manipulation in robot-assisted procedures, we sought to evaluate the comparative outcomes of robot-assisted laparoscopic pyeloplasty (RALP) and laparoscopic pyeloplasty (LP) in a paediatric patients with pelvi-ureteric junction obstruction (PUJO).
Methods:
We conducted a systemic literature search of online sources, including PubMed, MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials, and respective bibliographic reference lists. Success rate, operative time, hospital length of stay, postoperative complication rate and re-intervention rate were our primary outcomes. Combined overall effect sizes were calculated using fixed-effect or random-effects models.
Results:
We identified 14 observational studies reporting a total of 2254 paediatric patients with PUJO, who underwent LP (n = 1021) or RALP (n = 1233). Our analysis demonstrated that RALP was associated with a significantly higher success rate [odds ratio (OR) 2.51; 95% confidence interval (CI) 1.08–5.83, p = 0.03] and shorter length of hospital stay [mean difference (MD) −1.49; 95% CI −2.22 to −077; p < 0.0001] compared with LP. Moreover, nonsignificant reductions in postoperative complications (OR 0.61; 95% CI 0.36–1.02; p = 0.06) and re-intervention (OR 0.43; 95% CI 0.15–1.21; p = 0.11) were found in favour of RALP. There was no difference in procedure time between the two approaches (MD −0.15; 95% CI −30.22 to 29.93, p = 0.99).
Conclusions:
Our meta-analysis of observational studies demonstrated that RALP is safe and may have higher success rate compared with the more traditional laparoscopic approach in a paediatric population. Moreover, it may be associated with lower postoperative complications and re-intervention rates. Evidence from randomized trials is required.
Introduction
Pelvi-ureteric junction obstruction (PUJO) is a condition frequently encountered by urologists, both paediatric and adult, and describes an obstruction of urinary flow from the renal pelvis into the ureter. 1 It is the commonest cause of hydronephrosis in children, with around half of antenatal hydronephrosis diagnoses on screening ultrasound being secondary to PUJO upon further investigation. The reported incidence of PUJO is around 1 in 500 live births.2,3
The most commonly performed surgical intervention for PUJO in a paediatric population remains the open pyeloplasty, with an unrivalled success rate to date. 4 Despite this, there has been a growing acceptance towards laparoscopic pyeloplasty (LP) in the past few decades, and more recently, robotic-assisted laparoscopic pyeloplasty (RALP), owing to their reported similar success rates, shorter hospital stays, and increased parental approval. 5 Moreover, more precise suturing and a reduced learning curve have been reported associated with RALP compared with LP.6,7 The complexity of reconstructive procedures, such as pyeloplasty, which require challenging anastomoses, has further been aided by the robotic approach, negating the two-dimensional views and restricted instrument movements that can often cause difficulty. 8 A minimally invasive approach, such as LP or RALP is often performed transperitoneally, with either three or four ports being placed into the abdomen. In RALP, one port allows access for the bedside assistant, with the remaining ports accommodating the robot arms. A similar surgical technique is subsequently used for both approaches. 9
In 2014, a meta-analysis 10 of comparative studies demonstrated shorter length of hospital stay and lower analgesia requirement associated with RALP compared with LP in children with PUJO. However, the number of included studies in that meta-analysis was limited. As several more comparative studies have been published since 2014, we aimed to conduct a comprehensive systematic review and meta-analysis to evaluate the comparative outcomes of RALP and LP in paediatric patients with PUJO.
Methods
Design and study selection
This review conformed to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards. 11 Our study selection, analysis methods and outcomes for investigation were specified prior to the study. We planned to include all comparative studies evaluating the outcomes of LP and RALP in paediatric populations. Patients of any sex aged less than 18 years were included.
The intervention of interest was RALP in children for PUJO, and this was compared against LP. Primary outcome measures were success rate (defined by either the resolution of symptoms, or radiologically by resolution or reduction of hydronephrosis on ultrasound scan, or improved drainage with or without differential renal function on MAG-3 renogram, with or without resolution of symptoms), postoperative complications, length of hospital stay, procedure time and re-intervention rate.
Literature search strategy
Two authors (ST and OL) independently conducted a literature search utilizing: PubMed, MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials, with the final search on the 21 June 2018. The search strategy is listed in Table A.1. Bibliographic lists were also scrutinized for any further eligible studies.
Search Strategy.

This search strategy was utilized on the following databases: PubMed, MEDLINE, EMBASE and Cochrane Central Register of Controlled Trials.
Selection of studies
Two authors (ST and OL) independently assessed each study identified from the literature search. Full texts were obtained (MA), examined and at a study meeting, the eligibility criteria were selected. Discrepancies in study selection were resolved between the two authors following study selection and an independent third author (Shahin H) was consulted in the event of disagreement.
Data extraction and management
An electronic data extraction spreadsheet was created in line with Cochrane’s data collection form for intervention reviews. This spreadsheet was pilot tested in randomly selected studies and tailored as necessary. The data extraction spreadsheet contained:
(1) Study data and design (first author, country of origin, and year and journal of publication);
(2) Baseline demographics (age, sex, weight);
(3) Primary outcomes data.
Two authors (ST and OL) independently collected and recorded all data in this spreadsheet. Disagreements were resolved between the two authors, and if no resolution achieved, an independent third author (Shahin H) was consulted.
Assessment of risk of bias
The methodological quality and risk of bias of the included studies were assessed independently by two authors (ST and OL) using the Newcastle–Ottawa Scale (NOS). 12 When discrepancies existed, a third author (Shahin H) was consulted.
Summary measures and synthesis
For dichotomous outcome measures (success rate, postoperative complications and re-intervention), the odds ratio (OR) was calculated as the summary measure and presented with the 95% confidence interval (CI). The OR was defined as the odds of an event in the RALP group compared with the LP group. An OR < 1 would favour the RALP group except in the analysis of the success rate, where the OR > 1 would favour the RALP group. For continuous outcome measures (length of hospital stay, procedure time), the mean difference (MD) was calculated between the RALP and LP groups.
The individual patient was used as the unit of analysis, with information regarding missing data evaluated, and if required, authors contacted.
The Review Manager (RevMan) 5.3 software (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, 2014) for data synthesis 13 was used. An independent author (Shahin H) entered the extracted data into the Review Manager, and this was independently checked by another author (Shahab H). Fixed-effect modelling was used as appropriate for the analysis, with the random-effects models applied when significant between-study heterogeneity existed. The results were reported in the forest plots with 95% CIs.
Heterogeneity among the studies was evaluated using the Cochrane Q test (χ2). Inconsistencies were addressed by calculating I2 and interpreted using the following guide:
(1) 0–25% may not be important;
(2) 25–75% may represent moderate heterogeneity;
(3) 75–100% demonstrates considerable heterogeneity.
Additional analyses were performed to explore potential sources of heterogeneity, involving repeated primary analysis, and the effect of each study individually on the results, thereby assessing the robustness of our results.
Results
Literature searches via the databases identified 375 articles. Following further evaluation of the titles, abstracts and full text, 14 articles were deemed eligible for inclusion4,14–26 (Figure 1). These were one case-control study, one prospective cohort study, and 12 retrospective cohort studies, reporting a total of 2254 paediatric patients who underwent LP (n = 1021) or RALP (n = 1233) for PUJO. In 11 articles,4,14–16,18,20,22–26 all LP and RALP cases were performed using a transperitoneal approach, with one 19 only including cases that carried out a retroperitoneal approach. The RALP cases included in Franco and colleagues’ 26 study which adopted a standard laparoscopic technique to initiate exposure of the renal pelvis before completing with robotic assistance. The remaining two studies made no comment on the approach utilized.

PRISMA study flow diagram.
Table 1 represents our studies, including their date and origin of publication, journal and study design, as well as the baseline demographic and clinical characteristics of the study population. All studies, except one, included patients with similar ages and weights in their treatment groups. Reporting of baseline clinical characteristics were variable, with nonsignificant difference between the groups in each study.
Study characteristics and baseline demographics.

PLOS, Public Library of Science; RCS, retrospective cohort study; PCS, prospective cohort study; CCS, case-control study; NR, not recorded; L, laparoscopic; R, robotic-assisted; USS, ultrasound scan.
Methodological appraisal
Table 2 highlights the risk of bias assessment of the cohort studies, using the NOS. The risk of bias was low in 10 studies and moderate in 4.
Summary of study quality analysis using Newcastle–Ottawa Scale (NOS).

Each item scored 1 point, highlighted by asterisk, aside from comparability, which scores maximum of 2 points.
Outcome synthesis
Outcomes are highlighted in Figures 2 and 3.

Forest plots comparing LP with RALP.
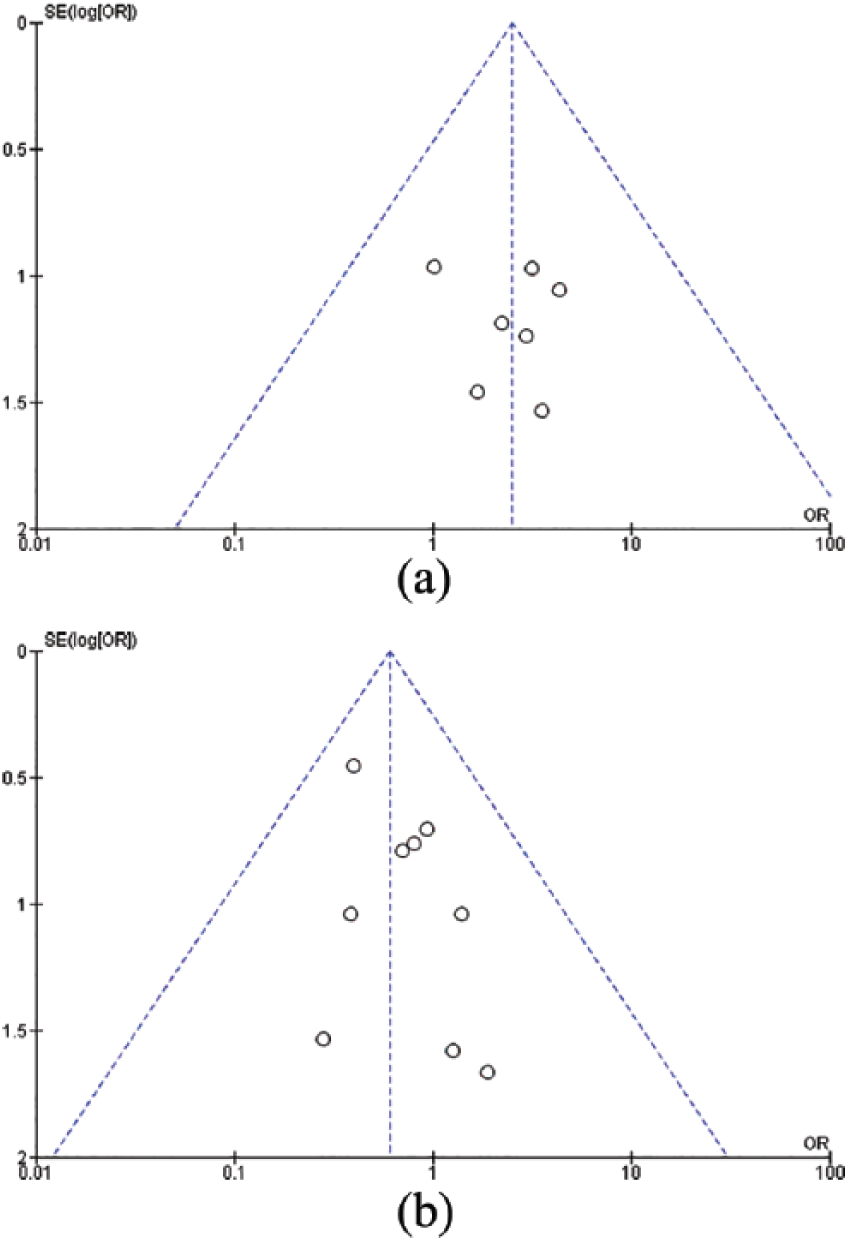
Funnel plots comparing outcomes.
Success rate
Eleven studies reported success rate as an outcome. The success rate in the LP and RALP were 96.2% and 98.2%, respectively. Our pooled analysis of 1138 patients demonstrated that RALP was associated with a significantly higher success rate compared with LP. Low between-study heterogeneity existed (I2 = 0%; p = 0.97).
Postoperative complications
Twelve studies (1721 patients) reported the incidence of their postoperative complications. There were 52 (8.0%) complications in the LP group and 43 (3.9%) complications in the RALP group. RALP was associated with lower postoperative complications than LP but the difference was not statistically significant (OR 0.61; 95% CI 0.36–1.02; p = 0.06). There was low heterogeneity among the included studies (I2 = 0%; p = 0.93).
Length of hospital stay
Six studies reported the length of hospital stay of their patients. Our analysis of 1791 patients showed that there was a significantly shorter length of hospital stay in favour of RALP (MD −1.49; 95% CI −2.22 to −077; p < 0.0001). There was considerable between-study heterogeneity (I2 = 93%; p < 0.00001).
Procedure time
Although 10 studies reported their procedure time, only four studies were included in the pooled analysis as the rest of the studies did not report the procedure time as mean ± standard deviation (SD) of their reported mean. The pooled analysis included 689 patient and did not find any significant difference in procedure time between LP and RALP (201.3 minutes versus 200.5 minutes, MD −0.15; 95% CI −30.22 to 29.93; p = 0.99). Considerable heterogeneity existed among the included studies (I2 = 86%; p < 0.0001).
Re-intervention
This outcome has been evaluated by nine studies (421 patients). The re-intervention rate in the RALP group was 1.7%, whereas 5.9% of the patients in the LP group had re-interventions. A nonsignificant reduction in re-intervention rate was associated with RALP compared with LP (OR 0.43; 95% CI 0.15–1.21; p = 0.11). There was low heterogeneity among the included studies (I2 = 0%; p = 0.79).
Sensitivity analysis
Using random-effect or fixed-effect models did not affect the pooled-effect size in any of the outcomes. The direction of pooled-effect size remained unchanged when the OR, RR, or RD was calculated.
Discussion
In light of current operative trends continually evolving in not only the urological field, but throughout the surgical world, it is imperative high-quality data are updated to give clinicians the resource to adapt, maintain and improve the care to their patients. As we enter an era whereby robotically assisted procedures are becoming the mainstay of tertiary urology centres, more and more data are extracted, highlighting promising results in a range of urological procedures. Despite this, current systematic reviews of the literature have highlighted a paucity of comparative trials in this field. 27 Furthermore, controversy exists with regards to pyeloplasty in children, and the ideal approach to perform optimal reconstructive procedures in this population. 28
In view of controversies with regards to pyeloplasty in children, and the ideal approach to perform optimal reconstructive procedures in this population, we conducted a comprehensive systematic review and meta-analysis to compare the outcomes of LP and RALP in children with PUJO and identified 13 cohort studies (1 prospective and 12 retrospective) and a case-control study reporting a total of 2254 paediatric patients [LP (n = 1021) or RALP (n = 1233)]. Our outcome analysis demonstrated that RALP was associated with a significantly higher success rate and shorter length of hospital stay compared with LP. Moreover, it was associated with a nonsignificant reduction in postoperative complications, and re-intervention rate. Nevertheless, our analysis did not find any difference in procedure time between the two groups. The between-study heterogeneity was low in the analyses of success rate, complications and re-intervention, suggesting that our conclusions regarding these outcome measures may be robust. However, there was considerable between-study heterogeneity in the analysis of length of hospital stay and procedure time, indicating a variability in reporting by the included studies.
Our findings from this meta-analysis indicate that an increased success rate using a robotic-assisted approach to paediatric pyeloplasties exists compared with the laparoscopic approach. This was determined utilizing imaging to determine a resolution of the PUJO in patients, in the form of ultrasound scanning or MAG-3 renograms, or describing the resolution of symptoms in patients troubled previously. These findings may be related to the more technically challenging laparoscopic approach in children, considering the much smaller working space, and thus a robotic approach may be adequate to alleviate this, specifically due to the enhanced magnification, three-dimensional vision and instrument dexterity associated especially when performing the more technically challenging elements. 29 An accelerated learning curve in robotic procedures has also been demonstrated, while maintaining safety and similar efficacies. 30
The previous meta-analysis performed by Cundy and colleagues 10 in 2014, found no significant differences in success rate between LP and RALP in a paediatric population. This is not consistent with our findings which demonstrated higher success rate associated with RALP. This may reflect that more widespread use of robotic surgery in recent years has positively influenced the surgeons’ learning curve, leading to higher success rate of robotic procedures. Nevertheless, no study quantified the learning curve of RALP to date. Therefore, we believe that our meta-analysis may demonstrate more realistic comparison of the RALP and LP.
We did find reduced postoperative complications and re-intervention rates in the children who underwent a robotically assisted procedure, and despite this not being clinically significant, it may still reinforce the better visualisation, access and approach associated with using the robot for paediatric pyeloplasty operations.
Our study does have some limitations. Namely, we were unable to identify any randomized-controlled trials despite their gold-standard status in comparative studies, with the majority being retrospective cohort studies. This will undoubtedly subject our studies to a degree of selection bias. Considering that an ideal meta-analysis should be a meta-analysis of randomized studies, findings of our meta-analysis of nonrandomized studies should be interpreted in context of its limitation. Furthermore, the risk of bias was moderate or high in most of the included studies, which may subject our finding to bias. Moreover, there remains an inconsistency in definition of operative time, which, through the included studies, can range from commencing at the initial incision or from the initial cystoscopy performed, as highlighted in Table 3. Finally, the included studies heterogeneously reported their follow-up period which was not comparable within and between the included studies. This, undoubtedly, subjects our findings to bias.
Definitions of operative time in included studies.

LP, laparoscopic pyeloplasty; RP, robotic pyeloplasty.
We encourage future studies to focus more on stent and drain placement. The psychological impact of drain insertion or living with and removing a JJ stent, as an infant and for family members, is an important comparative outcome that can be assessed through accurate and reliable reporting in cohort studies. Song and colleagues 4 suggested that the use of a robotically assisted approach requires less need for JJ stent insertion, comparatively. The use of patient- and family-related outcomes measures for this should be included in future studies. Consideration for future research with longer follow up for these patients, into adult life, and a consistent approach in reporting may be necessary to ensure that robust conclusions can be made in favour of an intervention.
Conclusion
Our meta-analysis demonstrated that RALP is safe and may have higher success rate compared with the more traditional laparoscopic approach in a paediatric population. Moreover, it may be associated with lower postoperative complications and re-intervention rates. Considering the ever-increasing exposure to robotically assisted procedures, especially in urological practice, it is imperative that high-quality randomized trials with longer follow up and adequate sample sizes are rolled out worldwide to improve the reliability of conclusions formulated, and the recommendations made for children requiring intervention to last them into their adult life.
Footnotes
Acknowledgements
Samih Taktak and Oliver Llewellyn equally contributed to this research and first authorship is shared.
Conception and design: ST, OL
Literature search and study selection: ST, OL, MA
Data collection: ST, OL
Analysis and interpretation: ST, OL
Writing the article: ST, OL
Critical revision of the article: All authors
Final approval of the article: All authors
Statistical analysis: Shahab H, Shahin H
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.