
Abstract
Paratesticular soft tissue tumours are remarkably rare entities, with malignant subtypes accounting for approximately 30%. Due to the paucity of cases, a consensus on the best treatment has not yet been reached, presenting a diagnostic and therapeutic challenge for clinicians. Although rare, three such cases presented to the care of our institution serving a population of approximately 400,000 in the space of 13 months. These were three gentlemen, aged 54, 82 and 86 years old, presenting with left sided testicular swellings. Ultrasound in each case confirmed an extratesticular mass. Only the second gentleman complained of associated pain, however he had experienced scrotal trauma in the preceding weeks. Only one patient had suspicions of metastatic disease, with a 9 mm pulmonary nodule on computed tomography. All patients underwent a radical inguinal orchidectomy with high ligation of the spermatic cord, in keeping with best accepted guidelines. Histology confirmed a well-differentiated liposarcoma, a dedifferentiated liposarcoma and a leiomyosarcoma respectively, all high grade. One gentleman returned to theatre for re-excision of margins. Our case series emphasises the need for full multidisciplinary team specialist sarcoma input, as well as radical resection with judicious margins in order to reduce the risk of local recurrence, in the treatment of these rare tumours.
Introduction
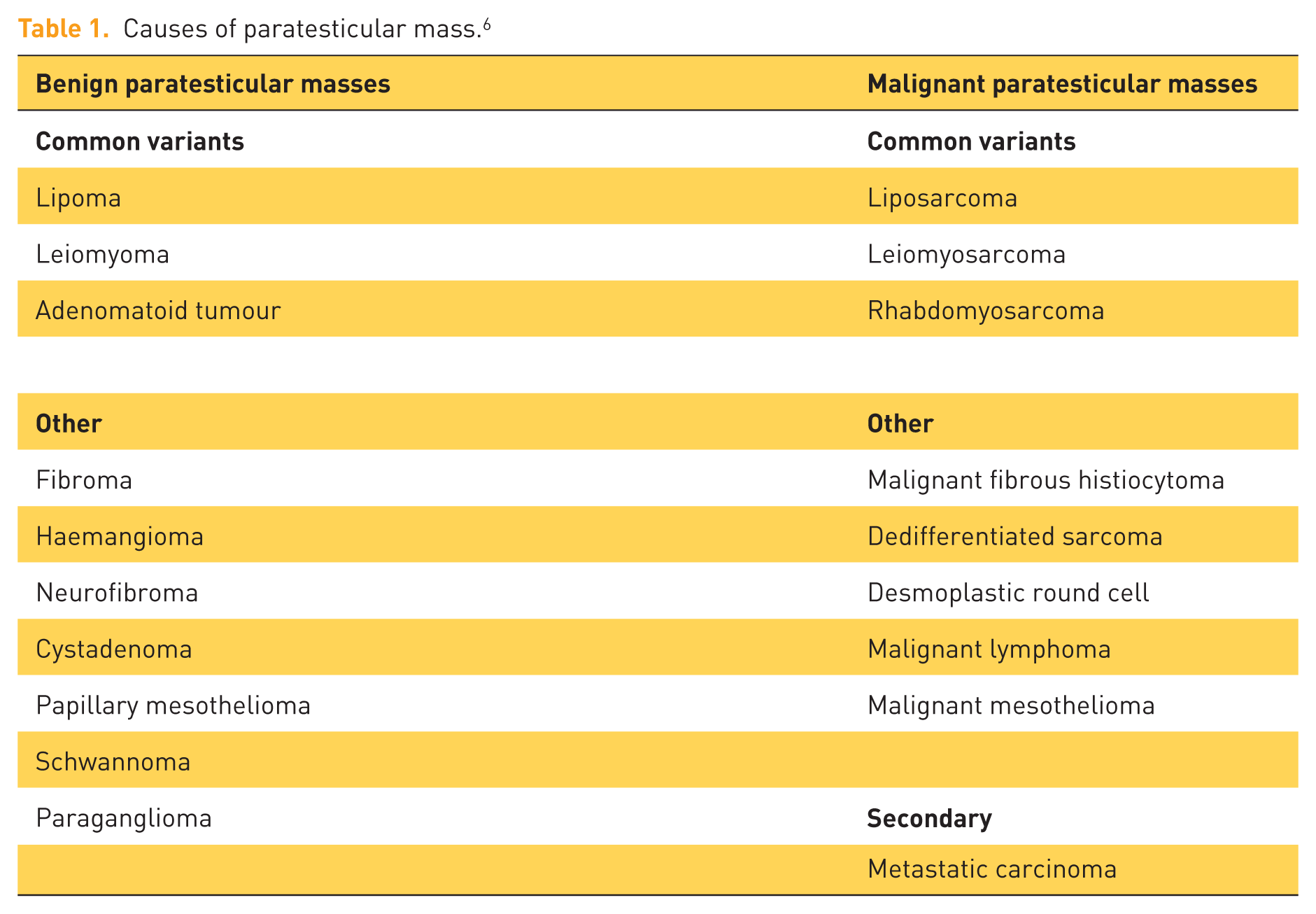
Paratesticular sarcomas is an all-encompassing term to describe the tumours arising within the scrotum but not of testicular origin and includes the epididymis, spermatic cord, tunica vaginalis and various supporting structures. 1 Thus, tumours arising from mesenchymal, epithelial and mesothelial cells may develop, however, on the whole, these are rare tumours, accounting for fewer than 5% of all testicular masses. 2 The majority of all paratesticular masses are benign and include lipomas, adenomatoid tumours and leiomyomas, however fewer than a third are malignant with 90% of these being sarcomas. 3 Malignant sarcomas include liposarcomas, rhabdosarcomas, and leiomyosarcomas as the most common three variants, with malignant fibrous histiocytomas or dedifferentiated sarcomas also being seen4–6 (see Table 1). The majority of paratesticular sarcomas arise from the spermatic cord. 7
Causes of paratesticular mass. 6
Men in their sixth decade exhibit the peak incidence of paratesticular sarcomas and typically present with a painful or painless scrotal mass or swelling, occasionally accompanied by a hydrocele.8,9 Rhabdomyosarcomas have a propensity to affect males in the first two decades of life and tend to be a more aggressive subtype. 7 Differentiation between the benign and malignant lesions by clinical examination alone is rarely accurate, let alone differentiation of tumour type, 9 thus further characterisation with imaging, namely ultrasonography is required. 10 This is of importance due to the radical nature of the resection in malignant cases (often requiring hemiscrotectomy and high cord ligation) when compared with simple excisions for benign tumours. Factors such as the age of the patient as described here and features on ultrasonography as mentioned in the section below, lend to help clinicians determine suspicious lesions from the benign and thus how aggressive the resection should be.
Ultrasound of the scrotum and its contents can very reliably differentiate between a testicular and a paratesticular mass with a sensitivity reported as >95%. 11 Due to its easy availability, lack of radiation exposure and ability to determine location and consistency of scrotal masses, it is typically the first investigation undertaken in the work up. Tunica vaginalis, epididymis, vestigial remnants and spermatic cord make up the paratesticular scrotal contents and thus tumours may arise from any of these structures. 12 Poorly defined, disorganised solid masses with heterogeneity and hypervascularity are features seen on ultrasonography favouring malignancy; however, in practice, the features between benign and malignant lesions often overlap, which may require further imaging techniques as described here.13–15 Lipomas are typically homogenous, hyperechoic, avascular lesions whilst the majority of liposarcomas will demonstrate abnormal fat, with solid or enhancing components indicating high-grade tumours for example.12,16 Calcifications, unlike testicular tumours, are not typically a feature of liposarcomas. 5 Leiomyomas sonographically present as well-defined solid lesions with variable echogenicity, with or without central necrosis or a whirling pattern. 12 Leiomyosarcomas display similar features to this, occasionally with a hypervascular flow of solid components, thus making sonographic differentiation between benign and malignant lesions challenging. 12 Rhabdomyosarcomas feature heterogenous lesions with cystic or necrotic areas on ultrasound. 12
In the case where the diagnosis is equivocal, magnetic resonance imaging (MRI) can be used with good effect to further characterise the lesion in question, in particular in defining the location of the tumour and its relationship with paratesticular structures.17,18 All sarcomas appear as solid, heterogenous, avidly enhancing paratesticular masses on MRI except for liposarcomas (NEW 17). MRI can also be of use in assessing the stage of the tumour by clarifying the local extent of disease. 19 Computed tomography (CT) of the abdomen and pelvis, with or without the thorax, is typically the modality of choice for staging tumour spread.6,10 CT and MRI can also be used to assess local, pelvic or retroperitoneal lymphadenopathy, the presence of which may influence surgical management as described later. 10 In relation to childhood sarcomas, some groups recommend positron emission tomography (PET) CT in the initial work up, staging and re-staging of rhabdomyosarcomas in particular, allowing the identification of inapparent soft tissue metastases as well as nodal and distant disease; however, there is no literature to support its use in adults. 20
Staging of paratesticular sarcomas is reported using the TNM (tumour, nodes, metastasis) system and is described in Table 2. 21
TNM staging of soft tissue sarcomas. 21

G1, well differentiated; G2, moderately differentiated; G3, poorly differentiated; GX, not assessed; M0, no distant metastasis; M1, distant metastasis; N0, no regional lymph node metastasis; N1, regional lymph node metastasis; T1, tumour ⩽5 cm (T1a superficial, T1b deep); T2, tumour >5 cm (T2a superficial, T2b deep); TNM, tumour, nodes, metastases.
The treatment of paratesticular sarcomas is surgical, with all tumours amenable to resection. 22 Simple excision of these tumours is inadequate and a previous study has shown that between 25–33% of patients who underwent simple excision had residual microscopic disease.8,23 The key to an optimal resection involves performing a radical inguinal orchidectomy with resection of surrounding tissue as well as high ligation of the spermatic cord at the external inguinal ring.6,24 Hemiscrotectomy, in cases where scrotal skin is involved or a previous operative scar is present, should be performed. 8 Although surgical clear margins can be difficult to achieve in paratesticular sarcomas, re-resection of incompletely resected tumours has been shown to trend towards improved disease-free survival, and thus should be attempted in those patients who are fit for a second procedure.8,25 Histological tumour grade has minimal impact on the risk of local recurrence; however, tumour size, proximity to the inguinal canal and positive surgical margins have all been implicated in recurrence.23,26,27 The role of aggressive surgical resection cannot be emphasised enough. Khandekar and colleagues showed in 25 cases of paratesticular liposarcomas that local recurrence-free survival (LRFS) is negatively impacted by positive margins with 29% versus 100% LRFS at 3 years, despite radiation therapy in those with positive margins. Thus, achieving clear margins in the first instance is the key to disease-free survival. 28
The role of retroperitoneal lymph node dissection (RPLND) has been debated but consensus seems to trend towards forgoing lymph node excision unless in the presence of suspiciously enlarged lymph nodes on imaging, or in the cases of rhabdomyosarcomas which have a significant propensity to spread to retroperitoneal lymph nodes.10,29 Tumour spread is typically by local extension into surrounding tissues, with direct invasion, haematogenous and lymphatic spread occurring in approximately 19.4%, 11.1% and 5.5% of cases respectively after 5 years of follow up in one study of spermatic cord sarcomas. 30 The more common subtypes, liposarcomas and leiomyosarcomas, spread and recur by direct invasion, thus RPLND is rarely required. 10 In relation to rhabdomyosarcomas specifically, retrospective analysis has identified retroperitoneal lymph node involvement in up to 40% of patients, with increased patient age (older than 12 years) and greater tumour size (>7 cm) of significant risk, thus should be considered in paediatric patients over 10 years of age as part of staging for rhabdomyosarcomas, however it must be emphasised that a consensus has not been reached.31–33
Adjuvant chemotherapy, as with lymph node dissection, does not have an established role and the jury remains out on its use. A statistically insignificant improvement in time to local and distant disease recurrence was seen with doxorubicin-based chemotherapeutic agents in a meta-analysis of several randomized control trials. 34 There have been case reports of patients with metastatic and locally recurrent rhabdomyosarcomas being successfully treated with surgery and adjuvant chemotherapy. 35 The exception to its limited benefit appears to be in childhood rhabdomyosarcomas where, instead of burdensome RPLND in the high risk group, systemic chemotherapy appears to have similar outcomes to RPLND in improving survival. 36 Some also advocate the use of chemotherapy in metastatic or high-grade liposarcomatous disease; however, in general, routine adjuvant use in paratesticular sarcomas is yet to be supported. 30
Radiation therapy in an adjuvant setting, on the other hand, has a more robust evidence base for its use, although a consensus on exactly who should have it routinely has also not been reached. Radiotherapy for sarcomas of the extremities is well documented to achieve a local control benefit, with a systematic review on its adjuvant use post-surgery quoting 90% local control. 37 In comparison, adjuvant radiotherapy for nonextremity-located soft tissue sarcomas such as head and neck, breast, retroperitoneum etc., does not translate into a definitive local control benefit. 37 With regards to paratesticular sarcomas, Coleman and colleagues reported no therapeutic benefit in adjuvant radiation therapy in any of the 21 patients whom they retrospectively analysed. 8 Catton and colleagues, however, had 100% local control of disease in the six patients they treated with adjuvant local groin or scrotal irradiation or adjuvant surgery and recommended it in all cases and recommended adjuvant radiotherapy in those at risk of local recurrence (namely those with previous intralesional surgery or narrow repeat resection margins).23,38 This was echoed by Ballo and colleagues who did not have any recurrences in the three patients treated with surgery and adjuvant radiotherapy.23,30 Fagundes and colleagues add weight to this argument following their study and also reached the conclusion that adjuvant radiotherapy may reduce locoregional recurrence. 39 More recently, Cerda and colleagues also had a 100% absence of recurrent disease following locoregional irradiation for spermatic cord sarcomas. 40 The main drawback of these conclusions is paucity of patient numbers.
Overall, 5 year cancer-free survival by international standards ranges from approximately 60–80%. 6 The 10 and 15 year overall survival rates have been quoted as 63% and 52% respectively, with local recurrence being the main failure pattern seen. 30 Recurrences however, have been seen several years after treatment and many authors recommend long-term follow up.10,24,41 The majority of high-grade tumours have been seen to fail, namely in retroperitoneal nodes or systemically, and thus, should be followed closely. 6
Case one
An 82-year-old gentleman presented with a left sided scrotal mass, present for approximately 6 weeks following scrotal trauma. This was initially treated in primary care with antibiotics; however, the gentleman presented with ongoing swelling and pain of his left hemiscrotum. On examination a tender and fluctuant swelling of the left hemiscrotum was evident. His notable bloods included a haemoglobin of 9.2 g/dl and C-reactive protein of >200. Tumour markers were performed and were within normal limits (β-hCG < 0.1 mIU/ml, α-fetoprotein = 0.7 ng/ml and lactate dehydrogenase (LDH) = 156 IU/l).
A scrotal ultrasound was performed, revealing an 11 × 9 cm extratesticular large, solid, heterogenous lesion with peripheral vascularity and occupying the whole scrotum (see Figures 1 and 2).

Left scrotal ultrasound showing heterogenous mass.

Left scrotal doppler duplex ultrasound showing peripheral vascularity of mass.
A scrotal exploration was performed under general anaesthetic where a large haematoma was found; however, with suspicions for underlying mass, a left orchidectomy was performed. Histopathological analysis was consistent with a high-grade malignant fibrous histiocytoma with positive spermatic cord margins. Following completion excision of the spermatic cord and hemiscrotectomy, the case was referred to a sarcoma unit which found the sarcoma to be consistent with an 8 cm high-grade dedifferentiated liposarcoma with associated positive margins. A subsequent staging CT of the thorax, abdomen and pelvis was positive for multiple satellite recurrences in pre-pubic and perineal soft tissue plus penile and scrotal lesions. Multidisciplinary team (MDT) meeting and clinical review found the patient to be too frail for further radical therapy or systemic treatment and he was referred for palliative radiotherapy.
Case two
A 54-year-old gentleman presented with a 2 year history of an increasing nontender, firm lump of the left spermatic cord. Tumour markers were performed and were within normal limits (β-hCG < 0.1 mIU/ml, α-fetoprotein = 1.7 ng/ml and LDH = 169 IU/l). Examination revealed a left hard hemiscrotal mass, distinct from the left testicle, measuring approximately 3 cm × 3 cm.
A scrotal ultrasound was performed which revealed a 2.3 cm × 3.7 cm soft tissue abnormality with central calcifications, potentially representing a fat-containing inguinal hernia however a sarcomatous lesion could not be ruled out (see Figure 3).

Ultrasound image of left inguinal lesion.
A scrotal exploration under general anaesthetic was performed which revealed a left groin mass, separate to the testis, which was resected intact. Subsequent histopathological analysis revealed a well-differentiated spermatic cord liposarcoma.
A CT of the thorax, abdomen and pelvis was performed which was notable for a left lung base 9 mm nodule. Sequential imaging 2 months later showed an increase in size of this nodule to 1.1 cm. The patient has been discussed at a specialist sarcoma MDT and is for clinical review and lung MDT for further discussion of the lung nodules.
Case three
An 86-year-old gentleman presented with a painless left testicular mass which had been present for several years however had recently been increasing in size. Tumour markers were also within normal limits (β-hCG < 0.1 mIU/ml, α-fetoprotein = 2.0 ng/ml and LDH = 143 IU/l).
A scrotal ultrasound was performed which identified a 10 cm irregular heterogenous hypervascular soft tissue lesion in the left hemiscrotum, separate to the left testicle, concerning for a sarcomatous lesion (see Figures 4 and 5).

Left hemiscrotal mass.

Increased vascularity of left hemiscrotal mass.
A preoperative staging CT of the thorax, abdomen and pelvis was performed which was negative for metastatic disease or pathological lymphadenopathy. A scrotal exploration, left orchidectomy with high ligation of the spermatic cord, wide local resection of hemiscrotal mass and hemiscrotectomy was performed under general anaesthetic. Histopathological analysis confirmed a high-grade leiomyosarcoma. The patient was referred to the sarcoma unit for further discussion and management. Figures 6 –8 show the resected specimen.

Left testicle, hemiscrotum and associated paratesticular lesion post-resection, anterior view.

Left testicle, hemiscrotum and associated paratesticular lesion post-resection, posterior view.

Sagittal section of left paratesticular sarcomatous lesion.
Conclusion
Paratesticular sarcomas account for the vast minority of scrotal masses and have several subtypes, with liposarcomas, rhabdomyosarcomas and leiomyosarcomas, among the commonest variants. Clinically, there is little to aid a diagnosis of paratesticular sarcomas and ultrasonography remains the most reliable radiological means of making a diagnosis of a sarcoma preoperatively. This is of significant importance and a high index of suspicion is required as the cornerstone of surgical management of these tumours involves radical resection with high spermatic cord ligation and possible hemiscrotectomy. Staging of tumours with modalities including CT and MRI is used, with PET CT reserved for cases of childhood rhabdomyosarcomas. Adjuvant chemotherapy has yet to establish a clearly defined role. Adjuvant radiotherapy has promising, yet sparse, data in reducing locoregional recurrence. All patients should have long-term (i.e. greater than 5 years) follow up. From the cases presenting to our institution, the value of case discussion at a specialist sarcoma unit is paramount and should be performed in all jurisdictions where possible to ensure specialist input and optimum patient management.