
Abstract
Primary spermatic cord tumors are rare yet clinically significant urologic lesions that affect patients of all ages. They are the most common tumors of the paratesticular region and generally present as asymptomatic, slow growing, firm, palpable paratesticular masses. Although most of them are benign comprised primarily of lipomas, approximately 25% are potentially life-threatening malignant tumors. The most common reported malignant histological types include liposarcomas, leiomyosarcomas, rhabdomyosarcomas, malignant fibrous histiocytoma, and fibrosarcomas. Management of these malignant tumors has been difficult because of their rarity, therefore there is little consensus regarding optimal surgical and adjunctive treatment strategies. It is recommended that radiological techniques such as scrotal ultrasound (US), computed tomography, and magnetic resonance be used to evaluate these masses before surgery. The curative treatment of choice is radical orchiectomy with high cord ligation and wide excision of surrounding soft tissue structures within the inguinal canal. Patients with inadequately resected disease should undergo a reoperative procedure for wide inguinal re-resection. Retroperitoneal lymphadenectomy is recommended when there is preoperative evidence of retroperitoneal lymph node metastasis and as an adjuvant treatment for rhabdomyosarcomas since they have a higher propensity for lymphatic spread. Adjuvant treatments, such as radiotherapy and chemotherapy, have shown little efficacy, except in the management of patients with local recurrence or high-grade rhabdomyosarcomas. Long-term follow up is recommended given their high recurrence rates.
Introduction
Primary paratesticular tumors are rare, accounting for 7–10% of all intrascrotal tumors. They are commonly grouped according to their location: testicular tunica, epididymis, or spermatic cord. In adults, more than 75% of these lesions arise from the spermatic cord [Sogani et al. 1978]. Therefore, primary spermatic cord tumors (SCTs) are of interest given that they are the most common tumors of the paratesticular region [Sogani et al. 1978]. However, investigation regarding management of SCTs has been difficult because of their rarity. Most of the available data come from small series from single institutions, and these have had inadequate or incomplete data available for risk factor analysis. Consequently, treatment recommendations are based on case reports, small series and literature reviews, making generalization regarding treatment and prognosis difficult. Such limitations have prevented the development of a consensus concerning optimal surgical and adjunctive treatment strategies. In this article we discuss the clinical behavior and the currently recommended management strategies of SCTs by reviewing the available literature.
Clinical presentation
SCTs usually present as unilaterally, hard, firm slow-growing masses (weeks or more than 10 years) of the inguinal canal or the scrotum, whose size varies between 1.5 and 30 cm [Ballo et al. 2001; Coleman et al. 2003; Montgomery and Fisher, 2003; Sogani et al. 1978]. These are frequently irregular masses that are clearly distinct from the testis, and usually do not transilluminate light during physical exam evaluation. They may be accompanied by pain, a hydrocele, or symptoms secondary to metastasis [Ballo et al. 2001]. However, for the most part the clinical manifestations are usually nonspecific, with a sensation of compression and heaviness due to local mass effect, which is diagnosed after a long evolution, since they are usually painless. Unlike most painless SCTs, however, malignant fibrous histiocytoma (MFH) may manifest clinically as a very painful mass, depending on the histological subtype (inflammatory or giant cell) [Hyouchi et al. 1996]. The tumors may assume large proportions and up to 13.5 kg liposarcomas of the cord have been reported [Chintamani et al. 2010]. Most patients present in their 50s or 60s. For unknown reasons, a relatively higher incidence has been reported in Japanese men but the cancer has been reported worldwide [Coleman et al. 2003].
Since most tumors occur at the inferior aspect of the spermatic cord, they usually appear as an intrascrotal mass. The clinical diagnosis may be difficult, since the tumor can easily be mistaken for an inguinal hernia, cyst, cord lipoma, hydrocele, funiculocele, spermatocele, hematocele, strangulated hernia or omentum, epididymo-orchitis, tuberculosis as well as tumors of the testis and epididymis [Arlen et al. 1969; Ballo et al. 2001; Banowsky and Shultz, 1970; Chintamani et al. 2010; Sogani et al. 1978].
Diagnostic studies
Most spermatic cord malignancies originate just below the external inguinal ring and grow as scrotal masses rather than inguinal masses. Since they may appear as scrotal masses, the preoperative clinical diagnosis of SCTs may be challenging given that it may be difficult to determine the exact location of the tumor. Therefore, any palpable suspicious mass of the cord should be investigated with US before excision [Woodward et al. 2003]. Sonography is the primary imaging method for any cord or scrotal abnormalities; it has a sensitivity of 95–100% for distinguishing intratesticular from extratesticular lesions [Frates et al. 1997]. The US examination is reliable in identifying and confirming the location and consistency of the mass as well as determining the status of the cord and the testes.
Sonography may help distinguish between the many possible entities in the differential diagnosis. Inguinal hernias which are common extratesticular masses can be identified by real-time tracing of the hernia along the inguinal canal and demonstration of the bowel wall, gas or fluid in the lumen, or peristalsis of the bowel [Akbar et al. 2003]. Simple hydroceles appear as anechoic dark fluid collections surrounding the testicle, whereas a complex hydrocele may contain internal echoes with septations and loculations [Blaivas and Brannam, 2004]. Epididymal cysts and spermatoceles usually appear as well defined anechoic masses [Akbar et al. 2003]. Acute epididymitis usually appears as a hyperechoic mass with increased flow Doppler study and can be diagnosed when combined with the clinical findings [Akbar et al. 2003]. However, chronic epididymitis, granulomatosis, tuberculosis, brucellosis, fungal infections, sarcoidosis, or syphilis can appear as epididymal masses having heterogenous echogenicity sonographically indistinguishable from tumors [Secil et al. 2004]. In addition, scrotal hematomas can occur in the absence of a known traumatic event and can also present a diagnostic challenge [Kyratzi et al. 2011].
Benign SCTs have a well delineated, homogeneous, hypoechoic appearance on sonography. In contrast, malignant neoplasms in this region tend to appear as a solid, vascularized, hyperechoic, heterogeneous mass with necrotic areas of variable size that tends to displace the testis. Paratesticular sarcomas, which make up about 95% of SCTs, usually have a heterogeneous pattern and are seen as hypervascular tumors on Doppler sonography [Akbar et al. 2003; Secil et al. 2004]. Liposarcomas are commonly bulky, heterogeneous tumors that have variable amounts of fat with hyperechoic areas [Akbar et al. 2003; Secil et al. 2004]. Leiomyosarcomas often appear as well defined masses with a soft tissue consistency that may show hemorrhage, necrosis, or cystic degeneration [Kyratzi et al. 2011]. MFH may appear hypoechoic with multiple small echogenic foci and acoustic shadowing consistent with flecks of calcification [Akbar et al. 2003; Secil et al. 2004]. Although these radiographic differences exist between sarcoma types, it is often extremely difficult to characterize the type of the tumor by US examination alone. However, the heterogeneous appearance and hypervascularity of a SCT may allow for the differentiation of a sarcoma from a benign SCT.
Although sonography is reliable in delineating the extratesticular location and paratesticular origin of a mass, US findings are often variable and nonspecific. In addition, it has been shown that ultrasonography cannot definitively demonstrate benignity. Frates and colleagues correlated the sonographic findings in 17 extratesticular masses with the corresponding surgical pathologic findings to determine if the sonographic appearance of solid extratesticular masses allowed for the distinction of benign from malignant disease [Frates et al. 1997]. They found that size, distinctness of borders, relation to the epididymis, and echo texture were not useful criteria for distinguishing benign from malignant lesions.
Computed tomography (CT) scan and magnetic resonance imaging (MRI) may be helpful in refining tumor location, morphologic features, and tissue characteristics [Akbar et al. 2003], as well as determining the extent of the mass into the neighboring tissues [Woodward et al. 2003]. CT is helpful in distinguishing a primary SCT from a retroperitoneal process extending into the scrotum. Although the use of CT scans is not widely reported, it has been found to be useful in narrowing the differential diagnosis by suggesting fat-containing neoplasms, such as liposarcomas. SCTs tend to have low attenuation/density and are well demarcated. However, there are no pathognomonic CT scan features for the differentiation of benign versus malignant masses [Cardenosa et al. 1990; Coleman et al. 2003].
MRI also helps characterize and delineate the anatomical extent of the tumor, as well as distinguishing testicular from extratesticular pathologic processes and solid from cystic lesions [Akbar et al. 2003]. Other modalities such as fluorodeoxyglucose positron emission tomography have been used in evaluating recurrent cases, but it is not established in routine clinical practice [Lipset et al. 1997]. Although the role of fine needle aspiration cytology in the preoperative diagnosis of SCTs has not been clearly established, it has been successfully used to diagnose different types of spermatic cord sarcomas such as liposarcoma [Dalla Palma and Barbazza, 1990], rhabdomyosarcoma [Daneshbod et al. 2005; Valeri et al. 2009], and NFH [Berardo et al. 1997; Bosch-Princep et al. 2000]. If there is concern for metastasis, radiological studies should include chest X-ray, as well as CT scan and MRI of the abdominopelvic and inguinoscrotal regions, specifically looking for the presence of pelvic or retroperitoneal lymphadenopathy. Since SCTs do not show specific radiographic patterns, it is generally accepted that the definitive diagnosis should only be made after the histopathological results have been obtained.
Histological types
Most SCTs are benign (70–80%) and are composed primarily of lipomas [Arlen et al. 1969]. However, because the spermatic cord originates from the mesoderm layer of the embryo (Wolffian duct) most malignant tumors of the spermatic cord (90%) are sarcomas [Arlen et al. 1969]. From a genetic point of view, sarcomas occur as a result of a mutation of a pluripotent mesenchymal cell that transforms into a malignant population of clones. The first paratesticular tumor ever reported was a sarcoma by Lesauvage in 1845 [Hinman and Gibson, 1924]. The most common reported histological types include liposarcomas, leiomyosarcomas, rhabdomyosarcomas, MFH, and fibrosarcomas. Table 1 shows the histologic distribution of SCTs according to the five largest published series [Ballo et al. 2001; Berkmen and Celebioglu, 1997; Coleman et al. 2003; Fagundes et al. 1996; Russo et al. 1992]. Figure 1 shows the overall weighted histologic distribution of these five studies combined. Liposarcoma and leiomyosarcoma are the most frequent histologic types in older patients, while rhabdomyosarcomas usually appear in young adults. MFH and fibrosarcomas are rare forms of SCTs, accounting for 10% and 5% of the cases, respectively.
Histologic distribution of spermatic cord tumors according to the five largest series and their overall weighted average.

MFH, malignant fibrous histiocytoma.

Histologic distribution of spermatic cord tumors according to the weighted average of the five largest series. MFH, malignant fibrous histiocytoma.
Spermatic cord liposarcomas are the most common type of malignant tumors, and most patients present in their fifth or sixth decade of life. The World Health Organization (WHO) classification of soft tissue tumors recognizes five categories in order of increasing malignancy: well differentiated, dedifferentiated, myxoid, round cell and pleomorphic. Most SCT liposarcomas are well differentiated, low-grade malignancies with no or minimal tendency to metastasize but they may be locally invasive [Schwartz et al. 1995]. Well differentiated liposarcomas feature lipoblasts with pleomorphic, hyperchromatic nuclei, and variable areas of pleomorphic spindle cells and sclerosis [Fitzgerald and Maclennan, 2009]. Therefore, these well differentiated liposarcomas are further divided into adipocytic (lipoma-like) liposarcoma, sclerosing liposarcoma, and into the two rare types of inflammatory and spindle cell liposarcoma [Montgomery and Fisher, 2003]. The sclerosing form tends to be much more common in the retroperitoneum and spermatic cord than elsewhere [Coleman et al. 2003]. Liposarcomas are immunoreactive for MDM2 and CDK4 markers, which can help differentiate the lesion from benign lipomas [Fitzgerald and Maclennan, 2009]. However, the most specific immunohistochemical marker is the S100 protein, which is positive in up to 90% of cases; and high-grade tumors are often positive for desmin [Astigueta Perez et al. 2007]. Most reports in the literature argue that the lesion arises originally from spermatic cord tissue; however, others believe it may arise as a malignant degeneration of pre-existing lipomas [Schwartz et al. 1995; Vorstman et al. 1984].
Similar to liposarcomas, leiomyosarcomas have a higher incidence after the sixth decade of life. Although the exact origin of leiomyosarcomas is unknown, it is speculated that they most likely originate from the smooth muscle of different cord structure areas, such as the vas deferens, canal wall, blood vessels and cremasteric muscle, and are thought to arise as a result of malignant degeneration from previously existing leiomyomatous tumors [Avila Padilla et al. 1993]. The role of hormonal stimulation has also been linked to leiomyosarcoma carcinogenesis [Varzaneh et al. 2002]. Immunohistochemical techniques may facilitate the diagnosis of leiomyosarcoma. Typically, actin muscle specific and desmin immunomarkers are positive, while reactivity to vimentin and protein S100 are negative. [Llarena Ibarguren et al. 2004]. Interestingly, some spermatic cord leiomyosarcomas have been found to produce β human chorionic gonadotropin [Llarena Ibarguren et al. 2004].
Spermatic cord rhabdomyosarcomas are rare tumors that occur mainly in the first two decades of life. Its histogenesis is related to the embryonic development of the spermatic cord, epididymis, testis, and connective tissue coverings [Hermans et al. 1998]. Three histological types have been described: pleomorphic, alveolar and embryonal, the latter being the most frequent. It is characterized by a large number of round or oval primitive cells and a small number of more differentiated rhabdomyoblasts with eosinophilic cytoplasm [Moroni et al. 2003]. They have a higher propensity for lymphatic and hematogenous spread than any other sarcomas.
MFH is the most common sarcoma in adults. It most commonly occurs in the legs and retroperitoneum, but only accounts for 10% of malignant SCTs. Therefore, presentation of MFH in the spermatic cord is an uncommon finding. MFH tumors are characteristically grayish white and tend to be large and infiltrate adjacent structures [Carrion Lopez et al. 2009]. Histopathologically, MFH is classified into four types: storiform-pleomorphic (83%), giant cell (9%), inflammatory (6%) and myxoid (rare) [Lin et al. 2002]. Immunohistochemical features have also been applied for diagnosing MFH. Immunohistochemistry displays vimentin reactivity and negativity for keratins [Bosch-Princep et al. 2000]. Table 2 summarizes the different immunohistochemical profiles of SCTs by histologic type.
Immunohistochemical profiles of spermatic cord tumors by histologic type
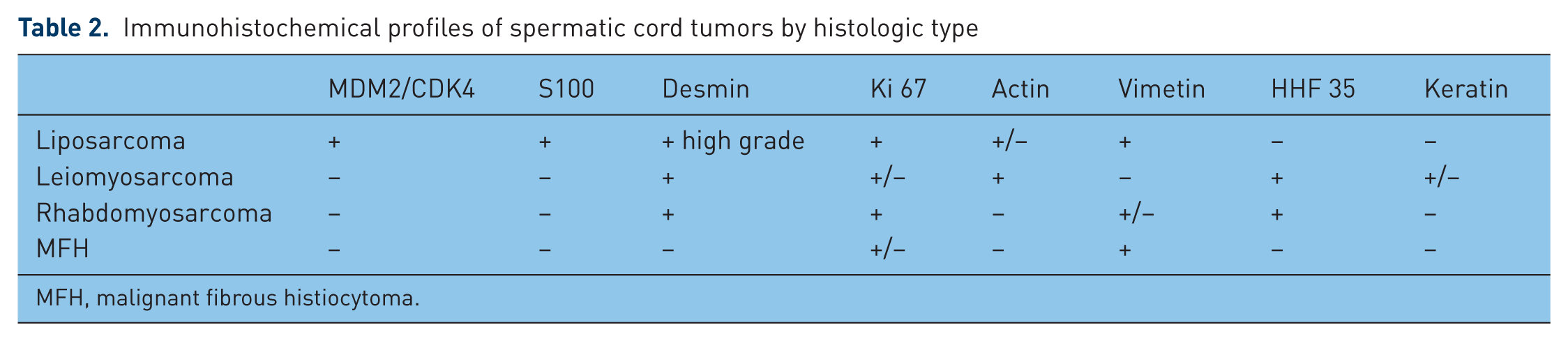
MFH, malignant fibrous histiocytoma.
Role of surgery
Consensus for proper management of SCTs has been difficult because of the rarity of the tumor. Consequently, treatment recommendations are based on case reports, small series and literature reviews, making difficult any generalization regarding treatment. Since most malignant tumors of the spermatic cord are sarcomas (90%), the general surgical principles of sarcoma therapy are followed. The standard therapeutic approach for these tumors has been radical inguinal orchiectomy and resection of the tumor with negative microscopic margins. These are essential components of the current management of SCTs.
Complete excision of the tumor with radical inguinal orchiectomy and high ligation of the cord has been the main primary surgical procedure [Ballo et al. 2001; Blitzer et al. 1981; Sogani et al. 1978]. However, due to anatomical constraints, tumors occurring in this region are rarely amenable to wide excision and wide circumferential resection margins can rarely be achieved with the tumor margins being almost invariably close. In addition, the tendency of sarcomas of all grades to infiltrate local tissues widely increases the difficulty of completing an adequate resection, and an inadequate procedure may actually promote the seeding of tumor through the operative site [Catton et al. 1999]. Therefore, loco-regional recurrence is a major common problem. The extent of appropriate amount of soft tissue excision remains controversial. Simple excision has been shown to be inadequate since repeat wide excision has revealed microscopic residual disease in 27% of completely excised cases [Catton et al. 1999]. In a more recent series Ballo and colleagues reported a local recurrence rate after resection alone of 30% at 10 years and 42% at 15 years, with local recurrence being the most common pattern of failure [Ballo et al. 2001]. Other series have also reported local recurrence rates of up to 50% after surgery alone [Blitzer et al. 1981; Catton et al. 1991, 1999; Fagundes et al. 1996; Merimsky et al. 1999; Sogani et al. 1978].
Aggressive surgical strategies are therefore recommended in the management of SCTs. A more aggressive surgical approach has recently been proposed as the gold standard of treatment. This involves wide en bloc excisions of all potentially contaminated surrounding soft tissues and re-excision in case of local recurrence of the disease [Coleman et al. 2003]. Coleman and colleagues reported that nearly one-third of patients without clinically apparent disease who underwent re-excision were found to have residual tumor. Furthermore, they noted that the presence of high-grade sarcoma in these re-resected cases represented a greater risk of recurrent and metastatic disease. Consequently, they observed a decrease in local recurrence and an improvement in disease-free survival in patients who underwent reoperative wide excision after a prior incomplete resection [Coleman et al. 2003].
It is generally accepted that the optimal initial surgical treatment of SCTs involves early radical orchiectomy and wide local resection that includes all nonvital structures. Given the high propensity for local recurrence, in patients with inadequately resected disease during primary surgery, the reoperative procedure for wide inguinal re-excision should be considered mandatory, even if this involves sacrificing some areas of adjacent normal anatomy [Enoch et al. 2005]. This includes patients who have also been previously treated with radical orchiectomy alone, and had a histopathological diagnosis of spermatic cord sarcoma. The procedure should include a wide resection around the inguinal canal, with completion radical orchiectomy, removal of the cord remnant and surrounding soft tissue deep to the internal inguinal ring. Scar excision including surrounding muscle layers should also be performed to obtain adequate negative margins [Coleman et al. 2003]. Hemiscrotectomy is also advised in the case of involvement of the scrotum or in patients presenting with a scrotal scar from prior surgery [Coleman et al. 2003]. However, it is important to note that although this more aggressive approach has been recently advocated, many publications report long disease-free periods after simple tumor excision without radical orchiectomy [Lopes et al. 2006].
Pathologic features that increase risk of recurrence include large tumor size, inguinal location, narrow or positive margins, surgery or manipulation of the tumor, the degree of nuclear differentiation, and the depth of invasion [Ballo et al. 2001; Coleman et al. 2003; Folpe and Weiss, 2000; Rabbani et al. 1997]. Rabbani and colleagues reported that a positive surgical margin was a risk factor for early local recurrence and distant metastases [Rabbani et al. 1997]. This emphasizes the importance of radical orchiectomy with wide local excision in the management of spermatic cord sarcomas. Generally, for sarcomas, size does not have any role in determining local failure. However, given the anatomical constraints of the inguinal region, it is expected that larger tumors recur more frequently due to the lack of adequacy of resection. Interestingly, it is well established that tumor grade has little influence on the probability of local recurrence, and a low-grade sarcoma is as likely to recur locally as a high-grade sarcoma [Pisters et al. 1996]. In summary, all sarcoma types, grades and sizes in the spermatic cord have a significant risk of local recurrence.
The main pattern of spread of spermatic cord sarcomas is through contiguous extension from the cord through the inguinal canal and into the abdominal cavity. Hematogenous and lymphatic invasions are less frequent. In the study of Ballo and colleagues, at 5 years, the local recurrence rate was 19.4%, the hematogenous metastases rate was 11.1%, and the pelvic lymph node involvement was 5.5% [Ballo et al. 2001].
Although the majority of spermatic cord sarcoma types have low propensity for nodal spread, a significant incidence in nodal relapse has been reported in some series, including rhabdomyosarcoma, MFH, and epithelioid sarcoma [Banowsky and Shultz, 1970; Sclama et al. 1983]. Since the regional lymphatic drainage of the spermatic cord includes the ipsilateral pelvic, inguinal, external iliac, hypogastric, common iliac and para-aortic nodes, elective treatment of these areas either with surgery or radiation therapy has been advocated. However, some authors doubt the high incidence of nodal metastases and, therefore, do not routinely advocate adjuvant nodal treatment.
Currently, the role of prophylactic lymph node dissection remains unclear. Proponents of lymphadenectomy indicate that the metastatic potential to regional lymphatics may be as high as 29% [Banowsky and Shultz, 1970]. In a review of 101 patients, Banowsky and colleagues described 29 cases of retroperitoneal lymph node involvement. Although argued by some authors, the true incidence of nodal metastasis has never actually been documented [Folpe and Weiss, 2000]. The general consensus in the literature, however, is that the most common SCTs, namely, liposarcomas and leiomyosarcomas, rarely involve loco-regional lymph nodes since they frequently recur and spread by direct extension. This might explain why to date there has not been any demonstrable benefit for patients who have undergone retroperitoneal lymphadenectomy. Therefore, there is insufficient evidence to suggest that prophylactic lymph node dissection prevents recurrence or improves the prognosis of patients with liposarcoma and leiomyosarcoma SCTs [Catton et al. 1991; Coleman et al. 2003]. However, lymphadenectomy may have a role in other types of spermatic cord sarcomas such as rhabdomyosarcomas, fibrosarcomas, and intermediate or high-grade MFH [Hermans et al. 1998; Sclama et al. 1983]. Given the low incidence of nodal metastasis from SCTs and the potential morbidity of lymphadenectomy, the consensus is against prophylactic retroperitoneal lymph node dissection. However, it is deemed mandatory in patients with preoperative evidence of retroperitoneal lymph node metastasis and in patients with a diagnosis of rhabdomyosarcoma [Banowsky and Shultz, 1970; Hermans et al. 1998].
According to the Intergroup Rhabdomyosarcoma Study, rhabdomyosarcomas are the only sarcomas in which unilateral retroperitoneal lymphadenectomy is indicated in cases of locally advanced and metastatic disease [Mora Nadal et al. 2004; Wiener et al. 2001]. Rhabdomyosarcomas have a higher propensity for lymphatic and hematogenous spread than any other sarcomas. Approximately 40% of patients with rhabdomyosarcomas present with metastatic disease [Schwartz et al. 1995]. During a 7-year period 14 cases of SCTs were seen at Memorial Sloan-Kettering Cancer Center, of which five presented with metastatic disease and all were rhabdomyosarcomas [Russo et al. 1992].
Surgical treatment of adult SCTs can provide an overall 5- and 10-year survival rate of 75% and 55%, respectively; and an overall survival rate of 52% at 15 years has also been reported [Ballo et al. 2001; Coleman et al. 2003]. However, up to 30% of patients have microscopic disease after surgery, and many argue that patients should be treated with adjuvant therapies [Ballo et al. 2001; Catton et al. 1991].
Role of radiotherapy
The role of adjuvant radiation therapy and chemotherapy in the management of spermatic cord sarcomas remains controversial [Ballo et al. 2001; Coleman et al. 2003]. Some authors recommend adjuvant radiotherapy only for high-grade tumors or for those patients believed to be at a high risk of local recurrence. Given the limited experience in the treatment of SCTs, there is no uniformity of criteria to indicate when an adjuvant therapy is necessary [Coleman et al. 2003]. While some authors advocate prophylactic radiotherapy after primary surgery for local disease control and even to reduce loco-regional recurrence [Ballo et al. 2001], others do not believe that radiotherapy plays a role in control of local recurrence. However, due to the high propensity of local recurrence following surgery alone there is increasing consensus that SCTs of all grades and histology should receive adjuvant radiotherapy. The trend in treatment of soft tissue sarcoma has been to perform wide en bloc excisions in combination with radiotherapy. For extremity sarcomas, this approach has produced high rates of local control. The experience with paratesticular sarcoma is less extensive but the literature shows that there tends to be local failure in the scrotum and groin following inguinal orchiectomy, and more recent reports suggest that this risk can be reduced with adjuvant radiotherapy [Ballo et al. 2001; Catton et al. 1999; Fagundes et al. 1996; Rabbani et al. 1997].
An improvement in loco-regional control and disease-free survival has been observed following adjuvant radiotherapy. In their series of 21 patients, Catton and colleagues observed a 5-year disease-free survival rate of 56% in the case of surgery alone and 100% when surgery was followed by adjuvant radiotherapy (p < 0.01) [Catton et al. 1991]. Fagundes and colleagues analyzed 18 patients from the Massachusetts General Hospital, half of whom received adjuvant radiotherapy coupled with orchiectomy, while the remaining half received surgery alone. They reported no local failures in patients receiving adjuvant loco-regional radiotherapy compared with a 56% recurrence risk (five out of the nine patients) in those treated with orchiectomy alone [Fagundes et al. 1996]. These findings, which are in accordance with those of Catton and colleagues, suggest that adjuvant radiation, following radical orchiectomy, may control local microscopic disease and reduce the risk of loco-regional relapse. Therefore, a multimodality approach including surgery and radiation therapy might be the most appropriate approach to reduce the local recurrence rates. Unfortunately, there is currently no study large enough to support this strategy and future prospective trials will be difficult given the rarity of this tumor [Ballo et al. 2001]. There are also few data available regarding the best radiation dosage required for adjuvant radiotherapy for SCTs [Banowsky and Shultz, 1970]. Currently, the recommended dosage is 60–65 Gy over 6 weeks. Advocates of adjuvant radiotherapy propose that the radiation field should be directly guided at the inguinal canal, the ipsilateral pelvic nodes with the adjacent pelvic tissues, and scrotum [Ballo et al. 2001; Catton et al. 1991; Fagundes et al. 1996].
For management of patients with high-grade rhabdomyosarcoma with positive surgical margins, patients with local recurrence or other poor prognostic factors, there is consensus that loco-regional radiotherapy may be beneficial [Ballo et al. 2001; Beverly Raney et al. 2011]. It is important to note that adjuvant radiation should supplement rather than substitute radical surgical excision and should be started only after complete resection of the tumor is achieved surgically. The role of preoperative radiotherapy has not been clearly established, and currently there is no evidence to suggest that radiation before surgical intervention reduces the rate of recurrence or improves the overall survival.
Role of chemotherapy
Currently, there is no definitive role of chemotherapy in the treatment of SCTs and most of the recommendations are based on cases with recurrences. There are no controlled studies at present that specifically address the role of adjuvant systemic chemotherapy in adult SCTs. However, chemotherapy has a well defined role in childhood rhabdomyosarcomas [Stewart et al. 2003]. Rhabdomyosarcomas are the only paratesticular sarcomas that have shown improvement in all stages with combined chemotherapy based on vincristine, dactinomycin, and ifosfamide/cyclophosphamide. The use of systemic polychemotherapy (vincristine, cyclophosphamide, and doxorubicin) as an adjuvant treatment of liposarcomas has been advocated in high-grade subtypes or metastatic disease [Ballo et al. 2001; Kalyvas et al. 2004; Muller Arteaga et al. 2005]. Single-agent and combination chemotherapy regimens have also been used to treat MFH, leiomyosarcomas, and fibrosarcomas, but have not been shown to produce significant improvement [Carrion Lopez et al. 2009]. However, it is important to note that adjuvant chemotherapy has mostly been considered in high-grade histologic subtypes and in metastatic disease, which might explain the low percentage of patients who may benefit from chemotherapy. Therefore, given the relative resistance of SCTs against chemotherapy, a routine adjuvant systemic therapy is not justified, except in rhabdomyosarcomas.
Follow up
Given the unfavorable prognosis of SCTs and their high recurrence rates, patients should be closely monitored for a minimum period of 36 months as recommended by the literature. Subsequently, periodic follow up is still recommended since late recurrences of up to 42% at 15 years have been reported [Ballo et al. 2001]. The follow-up studies should include chest X-rays, CT scans and if there are symptoms of bone pain, bone scans should also be performed.
Conclusion
SCTs are rare neoplasms that present as slow-growing, firm, palpable paratesticular masses. They should be considered in the differential diagnosis for inguinal and scrotal masses. Imaging techniques such as scrotal US, CT, and MRI should be used to evaluate these masses before surgery. The curative treatment of choice is radical orchiectomy with high cord ligation and wide excision of surrounding soft tissue structures within the inguinal canal. Patients with inadequately resected disease should undergo a reoperative procedure for wide inguinal re-resection. The procedure should include a wide resection around the inguinal canal, with removal of the cord remnant and surrounding soft tissue deep to the internal inguinal ring. Scar excision including surrounding muscle layers should also be performed to obtain adequate negative margins Retroperitoneal lymphadenectomy is recommended when there is preoperative evidence of retroperitoneal lymph node metastasis and as an adjuvant treatment for rhabdomyosarcomas since they have a higher propensity for lymphatic spread. Adjuvant treatments, such as radiotherapy and chemotherapy, have shown little efficacy, except in the specific situations described. Local recurrence is common and can occur several years after initial treatment. Therefore, long-term follow-up periods are recommended.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sector.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.