
Abstract
Background:
The aim of this study was to report the impact of patients’ baseline characteristics on the incidence of acute kidney injury (AKI) after nephron-sparing surgery (NSS) for localized kidney cancer.
Patients and methods:
Data from our kidney cancer database were retrospectively extracted to include 402 patients who underwent NSS between March 2000 and June 2016, and had sufficient data. Definition of AKI was based on the postoperative serum creatinine levels and estimated glomerular filtration rate (eGFR) magnitude, which were measured during the 72 h after surgery.
Results:
Based on RIFLE and AKIN criteria, the overall rate of postoperative AKI was 35%. The average decrease in eGFR among patients who developed AKI was 20% as compared with the non-AKI subgroup (2%). In univariate analysis, variables that were associated with AKI included right-sided tumors (p = 0.014), male sex (p = 0.01), hypertension (p = 0.003), baseline eGFR (p = 0.009) and history of nephrolithiasis (p = 0.039). However, multivariate analysis revealed that the only independent predictors of postoperative AKI were hypertension (p = 0.009) and cigarette smoking (p = 0.024).
Conclusion:
AKI is a common complication of NSS affecting about one-third of the patients. The most important risk factors are hypertension and smoking.
Introduction
Nephron-sparing surgery (NSS) has become the standard of care for the management of localized renal tumors.1,2 NSS, as compared with radical nephrectomy, has been associated with better postoperative renal function, without compromising oncological safety.3,4 The improved postoperative renal function is associated with reduced noncancer mortality, mainly due to cardiovascular events.5,6
A significant number of patients develop acute kidney injury (AKI) after NSS; 7 this could be translated into long-term impairment of renal function with all the known deleterious consequences.
The aim of this study was to describe the relationship between patients’ characteristics including age, sex, comorbidities and the risk of AKI in patients undergoing NSS.
Patients and methods
Between March 2000 and June 2016, 640 patients underwent NSS in our department due to an enhancing solid renal mass. After excluding patients lacking critical data, patients with multiple lesions, patients <18 years-old, patients with concomitant surgical procedures and patients who had a previous NSS, the study group included 402 patients.
Routine follow up in the immediate postoperative period included renal function assessment on the day of surgery, postoperative days 1 and 2, and as clinically indicated thereafter. The long-term follow up was based on the American Urological Association and the European Association of Urology Guideline Panel for Renal Cell Carcinoma, 2015,2,8 which included history, physical examination, routine renal function, renal imaging, chest radiography and other tests as clinically indicated. After having the approval of the institutional review board, data were collected retrospectively, including patients’ demographics, comorbidities, basal renal function, surgical parameters and outcome.
Definition of AKI
AKI definition was based on AKIN and RIFLE criteria and was defined as the occurrence of one of the following conditions: (a) an increase in serum creatinine (sCr) by ⩾0.3 mg/dl (⩾26.5 mmol/l) above baseline, (b) an increase in sCr of ⩾0.5 times baseline, or (c) reduction of >25% of the estimated glomerular filtration rate (eGFR).9,10 The eGFR was calculated by the Modification of Diet in Renal Disease study equation (MDRD) equation. 11 AKI was graded based on the previously mentioned criteria:
Grade I: >25% decrease in eGFR, increase of 0.3 or more in sCr or sCrX1.5
Grade II: >50% decrease in eGFR, sCrX2
Grade III: >75% decrease in eGFR, sCrX3
Operative technique
Our operative technique for open NSS was previously described in details. 12 Briefly, an extraperitoneal, extrapleural supra-11th rib incision was performed on the operated side. In situ renal hypothermia was done by cooling the surface of the kidney with ice slush for 10–15 min immediately after clamping the renal artery. Renorrhaphy was done using either 2/0 VICRYL interrupted sutures or tissue adhesive BioGlue (CryoLife, Atlanta, GA, USA).12,13
Statistical analyses
Data were presented as averages with standard deviations, medians 95% confidence intervals and frequencies. Continuous groups were tested for normality using the Kolmogorov–Smirnov test. The two or more parametric groups were compared using the student’s t test or the one-way analysis of variance (ANOVA) tests with correction for multiple comparisons, as appropriate. Nonparametric groups were compared with the Mann–Whitney U test or the Kruskal–Wallis ANOVA test. Associations between categorical variables were evaluated using the Chi-square test or Fisher’s exact test as needed. Correlations between continuous or ordinal variables were tested using the Pearson or the Spearman correlation coefficient. Multivariate analyses were performed to control for confounding variables, using the logistic regression or the discriminant analysis models, as appropriate. Two-tailed p values of 0.05 or less were considered to be statistically significant. All statistical analyses were done using SPSS version 23 (IBM corp., Armonk, NY).
Results
The study group included 402 patients with mean age 60.9 years and a median age of 61 years (Table 1). All patients had baseline and postoperative renal function data, and were divided into two groups based on postoperative change in serum creatinine and eGFR: Group 1 (n = 261) included patients who did not develop AKI and Group 2 (n = 141) included patients who developed AKI.
Patient baseline characteristics stratified according to postoperative AKI status.

AKI, acute kidney injury; BMI, body mass index; DM2, diabetes mellitus type 2; eGFR, estimated glomerular filtration rate; F, female; HTN, hypertension; IHD, ischemic heart disease; L, left; M, male; R, right; SD, standard deviation.
Based on the previously mentioned criteria, the overall rate of postoperative AKI was 35%. The average decrease in eGFR among patients who developed AKI was 20% as compared with the non-AKI subgroup (2%). We observed the following distribution of AKI severity: Grade I, 128 (90.8%), Grade II, 11 patients (7.8%) and Grade III, 2 patients (1.4%).
Univariate analysis was performed to assess the relationship between various baseline patients’ characteristics and the occurrence of postoperative AKI. As shown in Table 2, statistically significant variables that were associated with the development of AKI included right-sided tumors (p = 0.014), male sex (p = 0.01), hypertension (p = 0.003), baseline eGFR (p = 0.009) and history of nephrolithiasis (p = 0.039).
Univariate and multivariate analysis of potential factors affecting the rate of AKI.
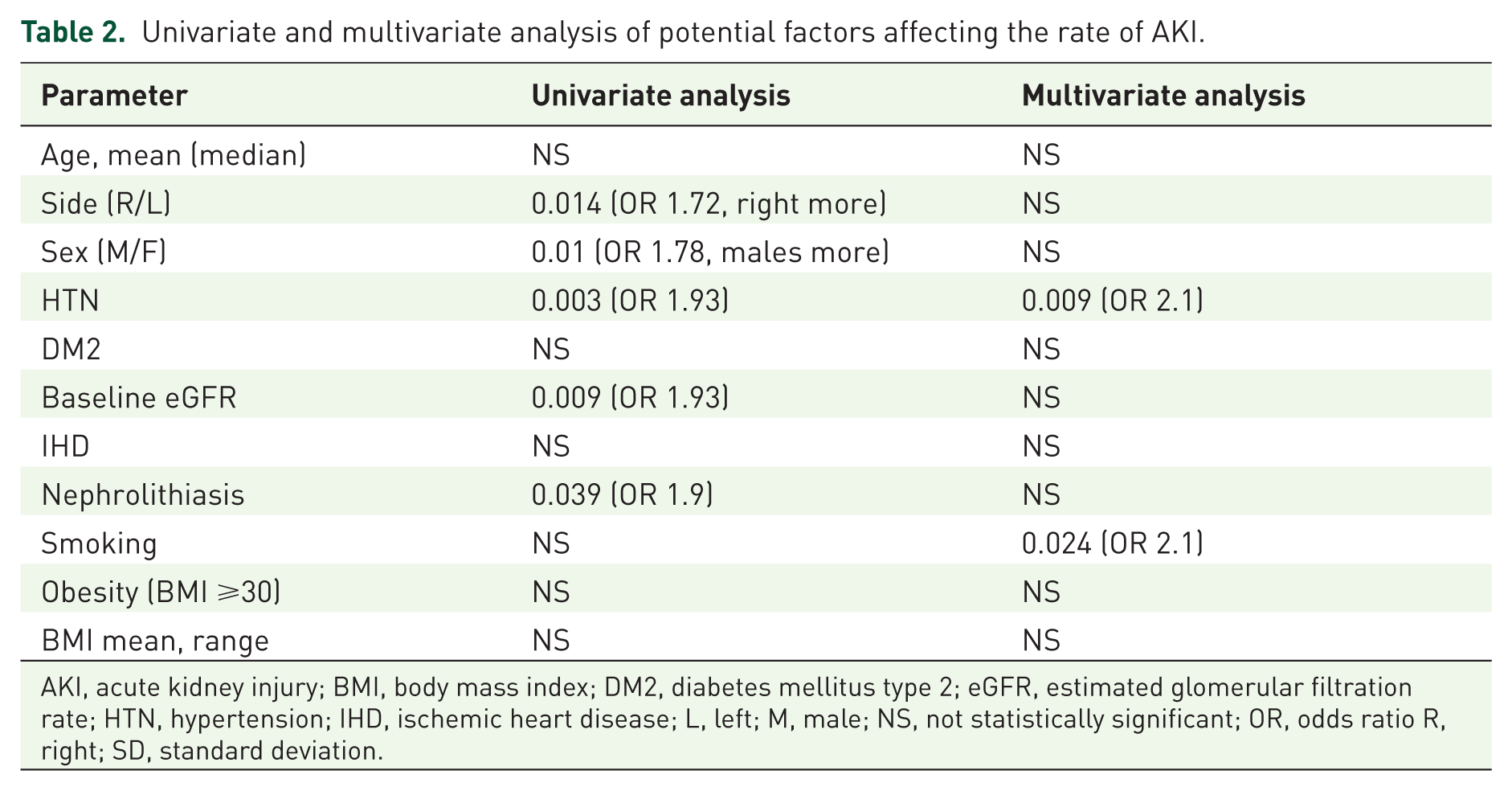
AKI, acute kidney injury; BMI, body mass index; DM2, diabetes mellitus type 2; eGFR, estimated glomerular filtration rate; HTN, hypertension; IHD, ischemic heart disease; L, left; M, male; NS, not statistically significant; OR, odds ratio R, right; SD, standard deviation.
Multivariate analysis revealed that the only independent predictors of post-surgical AKI were hypertension (p = 0.009) and cigarette smoking (p = 0.024) (Table 2).
Discussion
Compelling evidence indicates that the incidence of AKI is rapidly increasing, particularly among hospitalized patients with acute illness and those undergoing major surgery, including NSS. 14
The definition of AKI in patients undergoing NSS could be challenging. In our study, we defined AKI according to the medical AKI literature, 10 and as such, relatively a large number of patients met the criteria of AKI. Indeed, the majority of the patients with postoperative AKI had a small increase (0.3) in sCr. This small increase in sCr could be very common in patients undergoing such a major surgery, which involves some renal parenchymal loss and other patient-related factors. This may have impact on the high incidence of AKI among our patients. We assume that surgical AKI following NSS should have a more specific and less sensitive definition.
In the current study, we demonstrated that the immediate postoperative incidence of AKI among patients who underwent NSS in our medical center reached 35%. This rate is similar to the reported rates in the literature of patients undergoing NSS.15–17 For example, Gill and colleagues reported the renal outcomes of 800 laparoscopic partial nephrectomies in a single medical center, and showed that 36% of the patients exhibited a >25% decrease in eGFR. 16 On the other hand, Lane and colleagues reported 18% of AKI in their series of 660 partial nephrectomies of single kidneys. Unlike our definition, they defined AKI as any need for hemodialysis or any GFR measurement <15 ml/min/1.73 m2 within 90 days of surgery. 18 Using their definition, the AKI in our cohort would be 1.8% (two patients who developed a grade III AKI); however, their patients had single kidneys and so were more prone to AKI in these procedures.
In addition, others reported much lower 30-day incidence of AKI (4.6 %) after focal tumor ablation and after partial nephrectomy (9.4%).19,20 These studies defined AKI based on the last sCr on day 30 after surgery. Possible explanation for such a low rate of AKI could be the time course from surgery to sCr assessment, which enabled the kidney to recover. This is in contrast with our study, where sCr measurements were performed within the first 3 postoperative days. For this reason, it is hard to compare these studies with our study, mainly because they did not report the immediate AKI rate. Future reports of our data will show the short and long-term renal function in our cohort.
Whether the open technique plays a positive role in reserving renal function and reducing the AKI rate is controversial. However, our data show non-inferiority for the open technique. Lane and colleagues showed in a series of 1169 patients, that the 60% who underwent an open procedure had a slightly higher nadir eGFR and better long-term eGFR, with statistical significance. 21
Although all patients undergo similar surgical procedure, the question is why some develop an AKI while others do not experience such a complication. So far, objective definitions of patients at risk of developing an AKI due to this surgical maneuver are lacking or at most incomplete. Therefore, the present study extends our previous knowledge concerning potential demographic and clinical characteristics that prone certain patients to higher susceptibility of an NSS-induced AKI. Specifically, in our study the main independent factors that enhanced the vulnerability of patients to an NSS-induced AKI were hypertension and smoking (by multivariate analysis). Noteworthy, univariate analysis revealed that sex, side, nephrolithiasis and baseline eGFR negatively affected the postoperative renal function. The latter, which was slightly lower, in the AKI subgroup, is of special interest in light of its well established deleterious impact on the high susceptibility of the kidney to injury of various etiologies including NSS.22,23 Others have also reported association between age, hypertension and other comorbidities (diabetes, dyslipidemia and ischemic heart disease) with increased risk of reduced postoperative renal function.21,24,25 Regarding smoking, we showed in our analyses that it is a significant predictor of postoperative AKI. However, others showed that smoking does not affect postoperative renal function.15,21,25 This discrepancy could be attributed to the high smoking rate among the Israeli population, especially in men who were found to be more vulnerable to AKI in our study.
Our study had a few limitations, including its retrospective nature and being a single institution study. The database is limited with respect to the severity of diabetes mellitus, hypertension, ischemic heart disease and dyslipidemia in terms of duration, number of medication, and target organ damage. Despite that, the current study may help in preoperative patient counseling as well as considering the use of nephron-protective strategies for high risk patients undergoing NSS.
In summary, AKI is a common clinical problem following NSS. In light of the lack of an effective treatment for AKI and its association with high morbidity and mortality, pointing at certain demographic and clinical characteristics, which may predispose certain patients to AKI is of critical importance.
Conclusion
One-third of patients undergoing NSS may develop AKI. The most important patient factors related to an AKI were hypertension and smoking. A better definition for NSS-induced AKI should be considered.
Footnotes
Acknowledgements
Elias Hellouand and Zaher Bahouth contributed equally to this work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.