
Abstract
Background:
Androgen deprivation therapy (ADT) with luteinizing hormone-releasing hormone (LHRH) agonists is well established for the treatment of men with metastatic prostate cancer. As clear differences in efficacy, safety, or tolerability between the available LHRH agonists are lacking, the healthcare management team needs to look to practical differences between the formulations when selecting therapy for their patients. Moreover, as the economic burden of prostate cancer rises alongside earlier diagnosis and improved survival, the possibility for cost savings by using products with specific features is growing in importance.
Methods:
A review was conducted to summarize the information on the different LHRH agonist formulations currently available and offer insight into their relative benefits and disadvantages from the perspectives of physicians, a pharmacist, and a nurse.
Results:
The leuprorelin acetate and goserelin acetate solid implants have the advantage of being ready to use with no requirement for refrigeration, whereas powder and microsphere formulations have to be reconstituted and have specific storage or handling constraints. The single-step administration of solid implants, therefore, has potential to reduce labor time and associated costs. Dosing frequency is another key consideration, as administering the injection provides an opportunity for face-to-face interaction between the patient and healthcare professionals to ensure therapy is optimized and give reassurance to patients. Prostate cancer patients are reported to prefer 3- or 6-monthly dosing, which aligns with the monitoring frequency recommended in European Association of Urology guidelines and has been shown to result in reduced annual costs compared with 1-month formulations.
Conclusions:
A number of practical differences exist between the different LHRH agonist preparations available, which may impact on clinical practice. It is important for healthcare providers to be aware and carefully consider these differences when selecting treatments for their prostate cancer patients.
Keywords
Introduction
Androgen deprivation therapy (ADT) is the standard of care for men with metastatic prostate cancer.1,2 It is also recommended for men with biochemically recurrent disease (defined as increasing levels of prostate-specific antigen [PSA] following initial therapy 1 ), if they have symptomatic disease, proven metastases, or a PSA doubling time <12 months. 2 Based on the discovery over 70 years ago that prostate cancer is hormone dependent, 3 the aim of ADT is to suppress testosterone secretion or inhibit the activity of circulating testosterone thereby preventing stimulation of prostate cancer cells. 1 The beneficial effects of ADT on prostate size, symptoms of progression and survival outcomes have since become well established. 4 Currently available ADTs include bilateral orchiectomy, estrogens, luteinizing hormone-releasing hormone (LHRH) antagonists, and anti-androgens, but long-acting LHRH agonists are the most widely used ADT for advanced prostate cancer,1,4 and are the focus of this review.
In patients with advanced prostate cancer, LHRH agonists have been shown to achieve improvements in survival, progression-related outcomes, and time-to-treatment failure that are similar to bilateral orchiectomy, a procedure that many patients find psychologically difficult to accept.5–8 LHRH agonists are available in a number of different formulations, allowing them to be administered every 1, 2, 3, 4, 6, or 12 months (Table 1). Globally, the most commonly prescribed LHRH agonist is leuprorelin acetate, 9 which is available as a fully biodegradable solid implant or formulations for reconstitution (Table 1).9–13 Leuprorelin Sandoz® (HEXAL/Sandoz, Holzkirchen, Germany) is the only leuprorelin acetate solid implant currently available and there are two slow-release forms, a 1-month 3.6 mg leuprorelin depot implant and a 3-month 5 mg leuprorelin depot implant.12,13 There are two different leuprorelin acetate formulations that require reconstitution: Lupron Depot® (Takeda/AbbVie, Osaka, Japan) is a microsphere powder for reconstitution and Eligard® (Astellas/Tolmar, Fort Collins, CO) is a powder that is reconstituted using the Atrigel® delivery system to form a gel-like implant; both are available in 1-, 3-, 4-, and 6-month formulations (Table 1).10,11 Other commonly used LHRH agonists include Zoladex® (AstraZeneca, Macclesfield, UK), a goserelin acetate implant, and Decapeptyl® SR (Ipsen, Signes, France), triptorelin acetate powder for reconstitution (Table 1).9,14

IM, intramuscular; LHRH, luteinizing hormone-releasing hormone; PFS, prefilled syringe; SC, subcutaneous.
Product names may vary by country.
There are no clear differences in efficacy between the various LHRH agonists1,7 but a number of practical differences may impact on clinical practice, including storage temperature, handling (i.e. whether the therapy is ready for use or requires reconstitution), and route of drug administration (subcutaneous [SC] or intramuscular [IM] injection; Table 1).1,7
A physician’s perspective
Clinical response to LHRH agonists is determined by testosterone suppression to castration level, which was defined as <0.5 ng/ml more than 40 years ago based on the results of testosterone assays available at the time. 1 However, recent updates of the European Association of Urology (EAU) guidelines on prostate cancer state that <0.2 ng/ml is a more appropriate definition of the castration level.1,21 This recommendation to lower the target castrate level follows evidence from more accurate testing techniques showing that the median value of testosterone after surgical castration is actually 0.15 ng/ml or lower, and that failure to achieve testosterone levels <0.2 ng/ml with ADT correlates with reduced time to castrate-resistant prostate cancer and increased mortality.22–25
Although regulatory authorities still regard <0.5 ng/ml as the standard castrate level, 1 it is important that the different LHRH agonists demonstrate the ability to provide long-term, stable suppression of testosterone to <0.2 ng/ml, as growing evidence suggests that reaching and maintaining this lower castration level during ADT improves clinical outcomes.22,23,26 The leuprorelin acetate implant and leuprorelin acetate powder for reconstitution formulations have been shown to achieve durable testosterone suppression to <0.2 ng/ml in recent studies of patients with advanced prostate cancer.27–29 A pooled analysis of clinical data showed that two doses of the 3-month leuprorelin acetate implant achieved median serum testosterone levels of ⩽0.2 ng/ml within 4 weeks and lasted for up to 24 weeks (6 months) for the 12-week administration interval and 32 weeks (8 months) for a potentially longer 16-week administration interval. No episodes of testosterone escape were observed. 29 In an analysis of four open-label studies of the leuprorelin acetate powder for reconstitution, mean serum testosterone was consistently maintained below 0.2 ng/ml from week 5 for up to 24 weeks with the 1- and 3-month doses, 32 weeks with the 4-month dose, and 48 weeks with the 6-month dose. At least 90% of patients receiving each formulation achieved and maintained a ⩽0.2 ng/ml level of testosterone suppression between 6 and 24 weeks. 21 Similarly, in a retrospective analysis of two clinical trials, the leuprorelin acetate microsphere 4- and 6-month formulations have been shown to suppress serum testosterone to <0.2 ng/ml in 89% and 94% of patients from 4 weeks to 24 and 48 weeks, respectively. 22 Another retrospective analysis of two clinical trials showed that triptorelin acetate IM injections suppressed testosterone levels to <0.2 ng/ml in over 90% of patients at 6 and 9 months for the 1- and 3-month formulations, and at 6 and 12 months for the 6-month formulation. 30 There are no long-term data for testosterone suppression to <0.2 ng/ml with goserelin acetate formulations. However, a small Brazilian study reported that 55% of patients who received monthly injections of goserelin acetate achieved this castration level within 3 months. 31
In general, head-to-head studies comparing the efficacy of different LHRH agonists are lacking.14,26 Evidence from the few direct comparisons32–34 and indirect between-study comparisons that have been conducted indicate that broadly similar efficacy outcomes are achieved.5,26 However, preliminary evidence from a large observational study suggests that switching patients to the leuprorelin acetate implant from alternative LHRH agonist therapies (other leuprorelin formulations, goserelin, buserelin, and triptorelin) may improve clinical outcomes. 13 Patients switched to either the 1- or 3-month leuprorelin acetate implant were shown to experience significant improvements in testosterone and PSA levels versus baseline. 13
The safety and tolerability of the LHRH agonists (and LHRH antagonists, with the exception of abarelix) also appears to be comparable, with the most common side effects related to low testosterone levels. 7 Typical side effects include hot flashes, muscle weakness, fatigue, decreased libido, erectile dysfunction, and anemia.7,35–37 Loss of bone mineral density commonly occurs with LHRH analog treatment and, long term, may lead to fractures in up to 20% of men. 36 In addition, ADT is associated with metabolic and cardiovascular changes, potentially resulting in diabetes mellitus and abnormal lipid profiles. 36 The testosterone surge, which is associated with LHRH agonist (but not LHRH antagonist) treatment, may increase the intensity of the side effects, particularly in men with high-volume, symptomatic, bony disease. 1 The EAU 2017 guidelines, therefore, recommend a LHRH antagonist for the treatment of men with metastatic prostate cancer with impending spinal cord compression or bladder outlet obstruction. 1 Men with previous congestive heart failure or myocardial infarction may also benefit from treatment with a LHRH antagonist, but prospective evidence is needed as current data are inconclusive. 1
Acute and chronic side effects can be prevented or alleviated with simple interventional measures, for example, increasing physical activity can help to maintain a healthy body mass index, thereby reducing fatigue and muscle weakness as well as decreasing the risk of fractures and cardiometabolic changes.1,36
The EAU guidelines acknowledge there are no differences in efficacy and safety between LHRH agonists and suggest that physicians may need to consider differences in practical aspects, (e.g. storage, preparation time, and administration). 1 The main practical benefit of the leuprorelin acetate and goserelin acetate implants, compared with the other LHRH agonist preparations, are that they are supplied in prefilled ready to use applicators, with no requirement for refrigeration or reconstitution.9,12,13,15 This allows for single-step administration, significantly reducing administration time.16,38 Indeed, the preparation and administration time for implants was approximately halved compared with formulations requiring reconstitution in two randomized studies,16,38 thereby reducing labor time for healthcare professionals and potentially resulting in cost savings. 9 It has been suggested that implant formulations may be associated with reduced tolerability due to the need for a larger needle. 39 However, a subsequent randomized study investigated whether needle size affected pain perception in patients who were prevented from seeing the syringe or needle used to administer their treatment. 16 Although post-injection bruising was reported more frequently with the implant compared with a reconstituted formulation, there were no differences in pain levels and no requirement for analgesia when patients were unaware of needle size. 16
Monitoring of patients during LHRH agonist therapy is an integral part of treatment management in clinical practice. 1 Although follow up should be individually tailored, EAU guidelines recommend that patients be assessed at 3 and 6 months after treatment initiation, then every 3−6 months for men with metastatic disease and a good treatment response, or every 6 months for men with nonmetastatic disease and a good treatment response. 1 Serum PSA, serum testosterone, digital rectal examination, and symptom evaluation are the minimum requirements for follow-up assessments during long-term ADT to determine treatment response, identify episodes of testosterone escape (>0.5 ng/ml), and detect signs of disease progression or complications of ADT (particularly bone, metabolic, and cardiovascular complications). 1 This requirement for regular monitoring also appears to parallel the needs of patients in terms of management and information during LHRH agonist therapy. In a French study evaluating the roles of physicians and nurses in patients with prostate cancer receiving LHRH agonists, 3-monthly dosing was considered to be particularly appropriate as it met the needs of patients for face-to-face contact as well as providing a timely opportunity for healthcare professionals to ensure they were receiving optimal therapy. 40 Similarly, in a small case series, Finnish patients with advanced prostate cancer receiving LHRH agonist therapy were reported to prefer 3-monthly versus 1-monthly injections. 41 Regular contact with healthcare professionals helps patients to cope with the effects of their disease and its management on quality of life. 40 Patients also appreciate regular monitoring of their PSA and testosterone levels to ascertain if their treatment is working.
As men with prostate cancer often receive ADT for a prolonged period, establishing good long-term relationships between patients and healthcare professionals is very important.40,42 At treatment initiation, decisions about which LHRH agonist to prescribe should involve effective communication with the patient and take their individual preferences and lifestyle into account.42,43 Patients feel more confident if they are informed prior to starting treatment (e.g. administration procedures, frequency of administration, adverse events) so they can make an informed decision on their particular preference. Interestingly, the aforementioned French study found that patients considered the urologist to be their main source of detailed information about the disease and its management, including their treatment regimen and potential side effects, while their general practitioner (GP) was seen as providing a supporting role to the urologist, prescribing and administering treatment or answering questions when necessary. 40 Physicians are further supported by nurses who also administer injections and ensure patients understand the information provided by the urologist or GP. 40
Switching LHRH analogs in clinical practice: Croatian and Finnish experience
Although current treatment guidelines give no recommendations on switching between LHRH analogs,1,2,8 changing formulation of LHRH agonist 13 as well as switching from a LHRH agonist to LHRH antagonist 44 (or vice versa) may improve clinical outcomes. The efficacy and usage of the most widely prescribed LHRH agonists in patients with prostate cancer was investigated in a retrospective study conducted over 6 months in a single center in Croatia (Solarić and Soče, unpublished data; ethical guidelines followed). The most commonly used LHRH agonists were the 3-month formulations of goserelin acetate implant (Zoladex®; n = 61), leuprorelin acetate implant (Leuprorelin Sandoz®; n = 43), and leuprorelin acetate microsphere formulation for injection (Lupron Depot®; n = 40), as well as the 3-month (n = 122) and 6-month (n = 25) formulations of leuprorelin acetate powder for reconstitution (Eligard®). The LHRH agonists were used in combination with radical radiotherapy, postoperative (adjuvant and salvage) radiotherapy as well as a treatment for biochemical relapse and metastatic disease. Indications were similar for each LHRH agonist preparation. In agreement with published evidence, there were no significant differences between the agents in efficacy, assessed by testosterone level, although a numerically higher proportion of patients experienced testosterone escape (i.e. level of >0.5 ng/ml) with the leuprorelin acetate microsphere formulation (18%) versus the other LHRH preparations (4−8%). Not unexpectedly, therefore, more patients receiving the leuprorelin acetate microsphere formulation (15%) switched LHRH agonist because of testosterone rise than any other agent (0−8%), although numbers were small.
Of the 64 (22%) patients who switched LHRH agonist, most switched from the goserelin acetate implant (34%) and the 3-month formulation of leuprorelin acetate powder for reconstitution (26%). Few switched from the leuprorelin acetate implant (7%) and the 6-month formulation of leuprorelin acetate powder for reconstitution (0%). The reasons for switching from the goserelin acetate implant were not available for most patients but where this information was available the reasons included testosterone rise and switching to a formulation that can be given less frequently (Figure 1). The most common reasons for switching from 3-monthly leuprorelin acetate powder for reconstitution to a different LHRH agonist were simpler administration, reflecting the greater handling complexity compared with other preparations, and choice of a formulation with less frequent dosing (i.e. 6-month formulation). The main reason for switching from leuprorelin microspheres for reconstitution was testosterone rise (Figure 1).

Frequency and reasons for switching to an alternative LHRH agonist: a retrospective analysis (Solarić and Soče, unpublished data).
Although there have been many reports of switching from LHRH agonist to LHRH antagonist therapy, to our knowledge there is only one study evaluating switching from LHRH antagonist to LHRH agonist. 41 A total of 10 Finnish patients with advanced prostate cancer were switched from the monthly degarelix SC injection (Firmagon®; Ferring Pharmaceuticals), as they were experiencing injection site reactions, to the 3-monthly leuprorelin acetate implant. Post-switching mean PSA levels were similar or reduced compared with those measured prior to switching, indicating that there was no compromise in efficacy (Figure 2). Patients also reported increased satisfaction with the 3-monthly leuprorelin acetate implant, mainly due to no injection site reactions and reduced frequency of injection. All patients who switched to the leuprorelin acetate implant in the adjuvant setting stated that they preferred to continue with this therapy. 41

PSA levels measured before and after switching from an LHRH antagonist to an LHRH agonist: a Finnish case series. 41
Although further data are needed to support these preliminary findings in Croatia and Finland, they are in line with the EAU 2016 guidelines statement that LHRH agonists demonstrate similar efficacy but that variations in practical aspects need to be considered in everyday practice. 1
A pharmacist’s perspective
European guidelines for the management of prostate cancer do not differentiate between LHRH analogs in their recommendations for ADT in advanced prostate cancer1,2 so there is a need for tools that help with selecting the most appropriate treatment. 7 Rational drug selection may be aided by the use of a scoring system, such as the System of Objectified Judgement Analysis (SOJA). 45 In the SOJA method, a panel of experts defines selection criteria for a given group of drugs and determines the extent to which an individual drug fulfils these criteria, resulting in an overall score. As the administration and dosing frequency of LHRH agonists varies considerably, a scoring system such as this may help physicians with their decision-making processes. Currently, the SOJA system is only available as a publication but there are plans to develop it as an internet-based, fully interactive program for use by pharmacists and physicians.
The SOJA method was recently applied to LHRH agonists (buserelin, goserelin, leuprorelin, and triptorelin) and antagonists (abarelix and degarelix) in prostate cancer (Figure 3). 7 Each of the selection criteria (clinical efficacy, safety, tolerability, dosage frequency, user friendly formulation, drug interactions, precautions, documentation) was assigned a relative weight, based on the authors’ opinion, so that the treatments could be ranked by their resulting scores. The analysis showed that the LHRH agonists (leuprorelin acetate and goserelin acetate) had the highest scores and were therefore considered to be potentially the most useful drugs. Their main advantage over the other LHRH agonists was better documentation, therefore it was concluded by the authors that all four LHRH agonists were acceptable first-line treatments. The LHRH antagonists had lower scores based on a higher incidence of adverse events, a higher dosage frequency, more drug interactions and more limited documentation compared with the agonists. Hence, the authors suggested that the LHRH antagonists should not be used as first-line ADT, based on data available at the time.

Application of the SOJA method to LHRH agonists and antagonists: overall scores. 7
One of the practical aspects that differentiates between the LHRH analogs, and is an important consideration for pharmacists, is the need for specific storage conditions. Implant formulations are stored at room temperature (<30°C), and are ready to be used at any time (Table 1). By contrast, leuprorelin acetate powder for reconstitution must be kept refrigerated at 2−8°C (with a shelf-life of only 8 weeks if stored at room temperature), protected from moisture, allowed to reach room temperature for reconstitution and used within 30 min of reconstituting. 10 Leuprorelin microspheres and triptorelin powder can be stored at room temperature, but the reconstituted injections must be discarded immediately (triptorelin) or within 2 h (leuprorelin microspheres) if not used.11,17
Once ADT options have been selected based on quality aspects, differences in associated treatment costs need to be considered to curb the increasing economic burden of prostate cancer, resulting from improved early diagnosis, longer treatment duration, and increased survival.9,46,47 Differences in injection intervals for the LHRH agonists may have economic implications, with less frequent dosing potentially providing cost savings due to lower resource use compared with 1-monthly dosing. 48 In an economic evaluation of three clinical trials investigating the clinical effects of leuprorelin acetate powder for reconstitution, efficacy and safety were similar for all formulations but 3- and 6-monthly dosing reduced annual treatment costs compared with 1-monthly dosing in all nine European countries included in the model. 48
Early evidence that the leuprorelin acetate implant could potentially reduce the economic burden of prostate cancer in Europe was provided in a recent cost analysis comparison with the three most commonly used 1- and 3-month LHRH agonist preparations (goserelin acetate implant, leuprorelin acetate microsphere injection, and leuprorelin acetate powder for reconstitution). 9 A hypothetical population of 1000 prostate cancer patients were apportioned (based on drug market share) between these three LHRH agonists, and the annual costs and labor time were calculated for France, Germany, Italy, Spain, the UK (collectively referred to as EU5), and Sweden. 9 Cost calculations were then repeated for the hypothetical scenario, in which all 1000 patients switched to the leuprorelin acetate implant and compared with the total costs for the three most commonly used LHRH agonists. 9 Switching to the leuprorelin acetate implant showed potential annual cost savings per 1000 patients of €353,000 for the EU5 countries and €699,000 for Sweden (based on 1-month formulations), and €259,000 for the EU5 countries and €300,000 for Sweden (based on 3-month formulations) (Figure 4). 9 Estimated annual savings across the six markets included in the analysis were €53 million and €42 million for the 1- and 3-month leuprorelin acetate implants, respectively. 9 In addition, the leuprorelin acetate implant was associated with a reduction in labor time of an estimated 30 h per 1000 patients per year in each market. 9
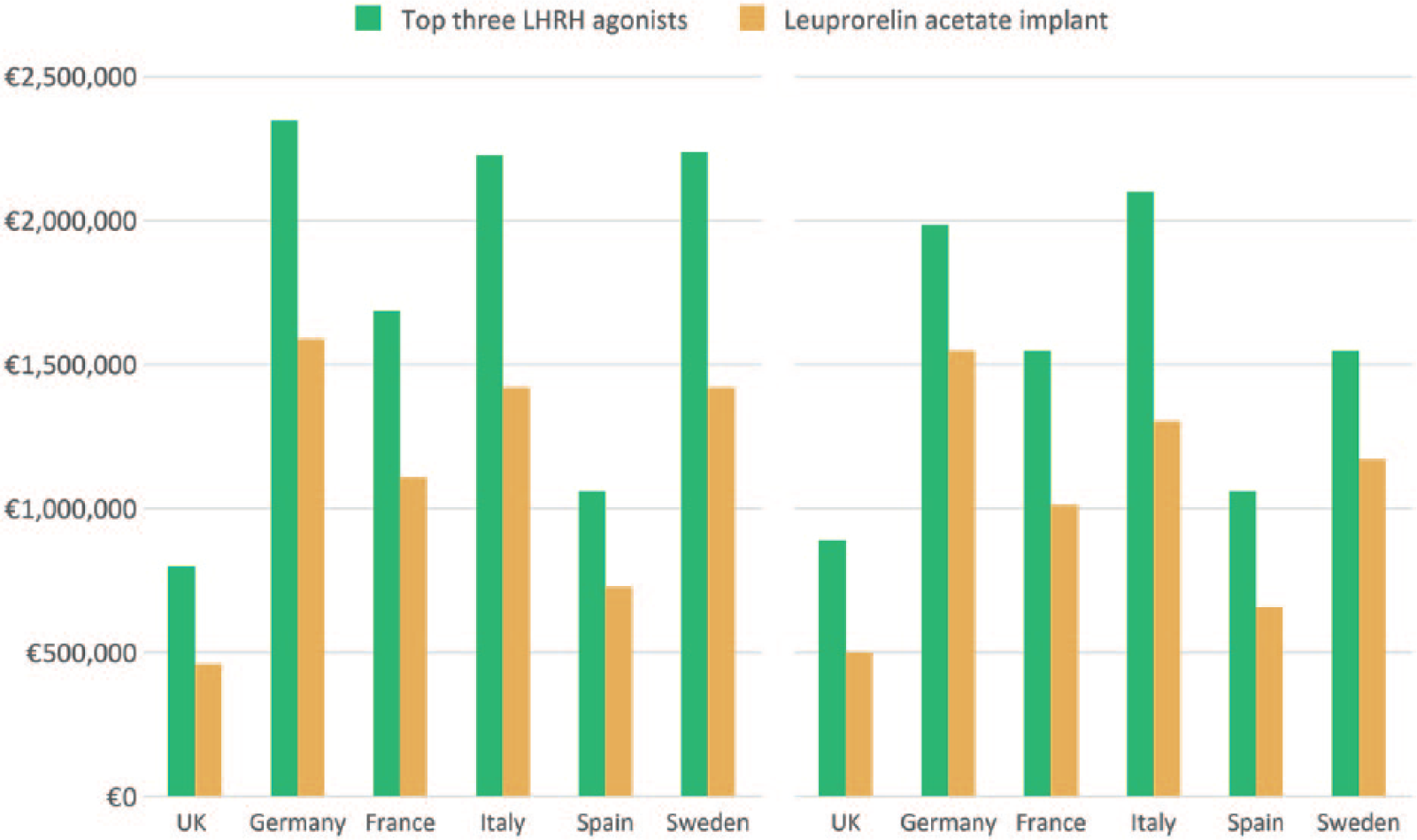
Mean annual total costs per 1000 patients based on the use of (a) 1-month or (b) 3-month formulations of the leuprorelin acetate implant versus the three most commonly used LHRH agonists. 9
These data support earlier findings from an observational study that reported the reasons for switching to the leuprorelin acetate implant from other LHRH formulations. 13 In the majority of cases (73%), patients were switched to the leuprorelin acetate implant due to high treatment costs of their previous medication, with switching for insufficient efficacy as the next most common reason (11%). 13 Hence, using the leuprorelin acetate implant in prostate cancer patients could, in theory, lead to substantial cost and time savings, potentially alongside improved treatment outcomes, 13 compared with the most commonly used alternative LHRH agonist preparations, allowing resources to be allocated elsewhere in disease management. 9
A nurse’s perspective
Clarifying what the patient’s physician (urologist or GP) has said, advising on what questions to ask the physician and providing psychological support is critical to helping both the patient and their family cope with the disease and its management. 40 In some countries, nurses are also responsible for administering LHRH agonists, 40 and for these healthcare professionals, ease of use is an important issue. 49 The leuprorelin acetate and goserelin acetate implants have the advantage of being ready to use compared with the other formulations, which may need reconstitution with vigorous mixing and administration immediately or within 0.5−2 h.9–13,16,17 Leuprorelin acetate powder for reconstitution also requires time to reach room temperature following storage at 2–8°C. 10
In a study investigating nurses’ perceptions of LHRH agonist therapies, more nurses preferred an implant formulation and perceived it as being easy to use and having a good safety profile versus a formulation requiring reconstitution. 38 Administration time, comprising preparation and delivery, has been shown to be significantly shorter with implants versus reconstituted formulations.16,38 There is a lack of data comparing the ease of use of the different LHRH implants but, in clinical practice, the technique for injecting has been found to be easier with the leuprorelin acetate implant than the buserelin acetate implant. For example, there are no loose parts in the leuprorelin acetate implant, whereas the buserelin acetate implant often separates into two parts when the safety device is removed, necessitating reassembly before it can be used. Moreover, the leuprorelin acetate implant device has a squared form enabling the nurse to achieve a firm, stable grip during the procedure, and the needle length and sharpness appear to minimize the risk of injection bleeding and pain.
In terms of administering the injection, healthcare professionals generally prefer SC injections over IM injections because there is a greater target area for the injection, fewer anatomical landmarks are needed, immobilizing the injection site is easier, muscle mass does not need to be considered, shorter needles can be used, and there are fewer safety concerns. 49 The needles used to deliver the various LHRH analogs differ in size, ranging from 14 gauge for the solid implants to 25 gauge for a reconstituted leuprorelin acetate powder formulation (Table 1). Although needle gauge has been shown to correlate with injection pain frequency, other factors such as needle length and sharpness may affect patients’ preferences and can be optimized to minimize pain.50,51 In a single-blind study conducted in 50 patients, no differences between pain levels were found between injections of goserelin acetate implant via a 16-gauge needle and a leuprorelin reconstituted powder formulation via a 23-gauge needle when patients were unaware of needle size, and the majority of patients experienced minimal pain. 16 Furthermore, in a real-world study, physicians reported that injection pain occurred at least once in 57% of patients treated with the leuprorelin acetate implant, but the intensity of pain was mild in at least 91% of cases. Most patients (85%) and physicians (76%) reported their overall satisfaction with the leuprorelin acetate implant as very good or good (Sandoz, data on file). It may also be important to consider the injection volume during SC injection as it may impact on pain experienced by the patient, potentially depending on location of the injection.52,53
Patients with prostate cancer have reported that they prefer 3- or 6-month dosing schedules overall, and 3-month dosing is often preferred at treatment initiation in order to fulfil a need for personal contact with their healthcare providers.40,42 This level of contact with the nurse, who often administers the injections, helps patients to cope with the disease and therapy, providing an opportunity to reassure them about safety and efficacy, and has beneficial effects on quality of life.40,42 Patients treated with LHRH agonists for at least 3 years are more likely to agree to 6-monthly dosing than those treated for less than 12 months, although patients willing to change to less frequent dosing would prefer to remain on their current LHRH analog than switch to an alternative. 40 Reasons for preferring a 6-month dosing schedule include convenience, quality of life, and fewer injections. 42 However, although using an LHRH agonist with a 6-month dosing interval may suit some patients and help to reduce the healthcare resource burden, this may not be a satisfactory option for some patients who prefer a shorter dosing interval. 43
Conclusions
It is important for healthcare providers to be aware and carefully consider the practical differences that exist between the different LHRH agonist preparations available when selecting treatments for their prostate cancer patients. This helps to ensure that LHRH agonist therapy is tailored to the individual patient, taking their particular preferences, disease stage, and treatment duration into consideration. It is essential that the patient is provided with sufficient information about the treatment options for their respective indication (including administration procedures, frequency of administration, and all potential adverse events) so that they are able to make an informed decision about their preference and feel confident about their treatment. Good communication between the physician and patient is therefore crucial for determining the most appropriate treatment and preventing suboptimal castration, which can lead to disease progression.
With the increasing cost burden of prostate cancer, it is inevitable that the cost of LHRH agonist therapy will also influence treatment selection. With acquisition costs of these therapies considered to be high, the introduction of generic formulations that are easy to store could potentially result in time and cost savings, irrespective of how different countries’ health systems are organized and funded.
Footnotes
Acknowledgements
Medical writing assistance was provided by Sarah Stutfield, PhD of Spirit Medical Communications Ltd, Manchester, UK, funded by Sandoz International GmbH, Holzkirchen, Germany.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. Sandoz International GmbH supported medical writing assistance as specified above.
Conflict of interest statement
Mladen Solarić has received honoraria from Abbot Nutrition, Kent, UK and is a consultant of regional offices for as well as received honoraria from Astellas Pharma, Surrey, UK; Sanofi, Paris, France; Janssen, Hrvatska, Croatia; Sandoz International GmbH, Holzkirchen, Germany; and Bayer-Pharma, Berlin, Germany. Davide Meani is an employee of Hexal AG, Holzkirchen, Germany. Harri Visapää, Majana Soče, Rose-Marie Rosén have no conflicts of interest to declare. Robert Janknegt currently has no conflicts of interest but has received in the past research grants from Sandoz, Holzkirchen, Germany and Bayer-Pharma, Berlin Germany.