
Abstract
Background:
This study examines subjective reasons for the refusal of treatment and the state of objective status markers of various factors influencing the resistance of patients when treating overactive bladder by antimuscarinic drugs (AMs).
Methods:
The socioeconomic and medical parameters were studied in 2465 patients aged 18–60 years (1446 women (58.7%), 1019 men (41.3%); mean age was 52.1) taking AMs during the year. The study control was carried out by studying passport data, employers’ income certificates, patients’ ambulatory medical records, the use of OABq-SF and MOS SF-36 questionnaires, voiding diaries and uroflowmetry.
Results:
The average time to reach the 30-day break in the AM administration was 177 days. During the 12-month follow up, 74.7% of patients discontinued their participation. In total, 35.9% of patients stated medical reasons for the refusal of AM treatment; in 31.9% of individuals in the group the deviation of objective health status markers from average sample values was established. Economic reasons for the refusal were given by 20.4% of patients; in 18.5% of individuals economic status markers were different from average sample values. In 24.1% of cases of refusal of treatment, patients indicated social and psychological reasons; objective social and psychological status markers were altered in 35.9%.
Conclusions:
The percentage of patients indicating economic and medical reasons for the refusal of AM treatment is statistically uniform with respect to the percentage of patients with objective disturbances of health and economic statuses. The percentage of patients indicating social and psychological factors as a reason for the refusal of treatment was significantly lower than the percentage of patients with altered social and psychological status markers. These results can be used in practical healthcare when predicting adherence to AM use.
Introduction
The prevalence rate of overactive bladder (OAB) is not less than 10.7% of the population, increasing in older people and women. 1 Some sources indicate that up to 25% of men and 50% of women of all races ‘at least sometimes’ notice OAB symptoms. 2 It is known that OAB symptoms may reduce the quality of life related to health, physical and mental activity, performance, lead to depression and breaking of social ties.3–5 The main drugs for management of OAB symptoms are antimuscarinic drugs (AMs). 6 AMs suppress the activity of M-acetylcholine receptors of different types, thus reducing the excessive activity of the detrusor and improving the voluntary control over the process of urine collection and emptying.7,8 In previous research, we drew attention to the patient’s poor adherence to AM treatment,9,10 which is consistent with other authors’ data.11,12 Some researchers state weak or, on the contrary, fast and good treatment effect, the presence of side effects and peculiarities of AMs’ pharmacodynamics as the main reasons for the lack of the treatment resistance.13,14 Others deny a significant effect of peculiarities of different AMs’ pharmacological properties on adherence, 15 and indicate age, polymorbidity, patients’ awareness, 16 income levels and expense relating to the purchase of medicines, 17 the number of days away from work and disability, and other economic and social factors18–20 as important elements of patients’ resistance. Nevertheless, many of the above pieces of research are not free of limitations: for example, they were carried out retrospectively, without patients participating themselves, the evaluation of administration was performed on the basis of prescriptions given. Also, a comparison of reasons for the refusal of treatment stated by patients themselves with the objective health status and socioeconomic status markers was not conducted, making it impossible to evaluate the impact of complex and varied reasons for differences in patients’ adherence to AM treatment.
In view of the above, we have set an objective – to study subjective reasons for the refusal of treatment and objective health status markers related to OAB: patients’ socioeconomic status markers to improve the prediction of the efficacy of OAB treatment by AM.
Subjects and methods
A total of 2465 patients of ages 18–60 years participated in the experiment, comprising 1446 women (mean age 51.5) and 1019 men (mean age 53.9). The sample size was determined on the basis of a 95% confidence coefficient and a ±5% confidence interval. The experiment was conducted from 1 October 2013 to 15 January 2015, housed by the city polyclinic No. 3 (Vladivostok) and the Far Eastern Federal University.
The group included individuals who sought medical advice from a urologist concerning OAB (ICD-10-CM N32.81) 21 in odd-numbered days of the month, and who got AM drugs prescribed (oxybutynin, tolterodine, trospium, solifenacin, darifenacin) as a permanent therapy.6–8
Exclusion criteria were simultaneous administration by patients of other anticholinergic drugs, the presence of terminal cancer, a chronic infection of the lower urinary tract and changes in the QT interval.
The first line of the study was an objective evaluation of sociodemographic, economic and health characteristics of individuals with OAB, to whom a long course of AMs during the follow up (12 months) was recommended, as well as their division into three cohorts considering their adherence to treatment. In cohort 1 were patients with poor adherence (<50%); in cohort 2 were patients with moderate adherence (50–79%); and in cohort 3 were patients with good adherence (⩾80%). The adherence evaluation was carried out using the model of waiting for a 30-day break in the AM administration.19,22 Factors that differed significantly in cohorts of individuals with various adherence in the future served as objective social, economic and health status markers when compared with subjective reasons for the refusal of treatment (the second line of the study).19,23
Control of socioeconomic factors was performed through study of passport data, documents provided by an employer and the tax inspectorate. Calculation of wage levels and expenses is presented, adjusted for inflation from the conversion of the national currency to US dollars as of June 2013. Access to the private information was performed with informed consents of patients, after they signed corresponding authorizations.19,22 Control of the health status was carried out using OABq-SF, uroflowmetry24,25 (monthly), as well as voiding diaries supplemented by columns containing information on the time of the AM administration and side effects (daily). 26 OAB symptoms were considered severe if there were 21 or more episodes of urinary incontinence per week. 27 Control of the social and psychological discomfort level was assessed using the MOS-36 questionnaire (monthly). 28
By medical reasons for the refusal of treatment are meant poor efficacy (i.e. the presence and severity of OAB symptoms in a certain time period after the therapy started, the presence of intolerable side effects, etc.).12,14,15 By economic reasons are meant income level, a high share of expenses for the purchase of AMs, other drugs, medical care, etc.17–20 By social and psychological reasons were meant aversion to using AMs, depression, communication-level reduction, problems with social support in the family, etc. 27 At the first control point the interim analysis and comparison of results was carried out; the second control point was the final analysis of the results.
To evaluate the feature (adherence) survival time, the Weibull distribution with the right censoring type 1 was used. The adjustment of division was carried out using the Hollander-Proschan test. We used modeling of signs’ regression to control differences between the cohorts. All statistical analyses were performed using SAS version 8.0.2 (SAS Institute Inc., Cary, NC, USA).
The principles of the Declaration of Helsinki were deemed to be obligatory when planning and conducting the experiment. The research was approved by the local ethics committee. The subjects were admitted to the experiment only after providing informed consent.
Results
Figure 1 shows the reduction in the percentage of patients’ adherent to treatment under the influence of subjective reasons stated by patients during follow up. The percentage of patients who refused treatment for medical reasons was significantly higher than the percentage of patients who refused treatment for economic reasons in the second half of the follow-up period.

The percentage of the refusal of treatment for various subjective reasons within the follow-up period (n = 2465).
Table 1 provides the regression-adjusted socioeconomic and medical parameters between the cohorts of individuals with poor, moderate and high adherence.
Diverse characteristics and parameters of persons with overactive bladder from 18–60 years old taking antimuscarinic drugs (n = 2465).
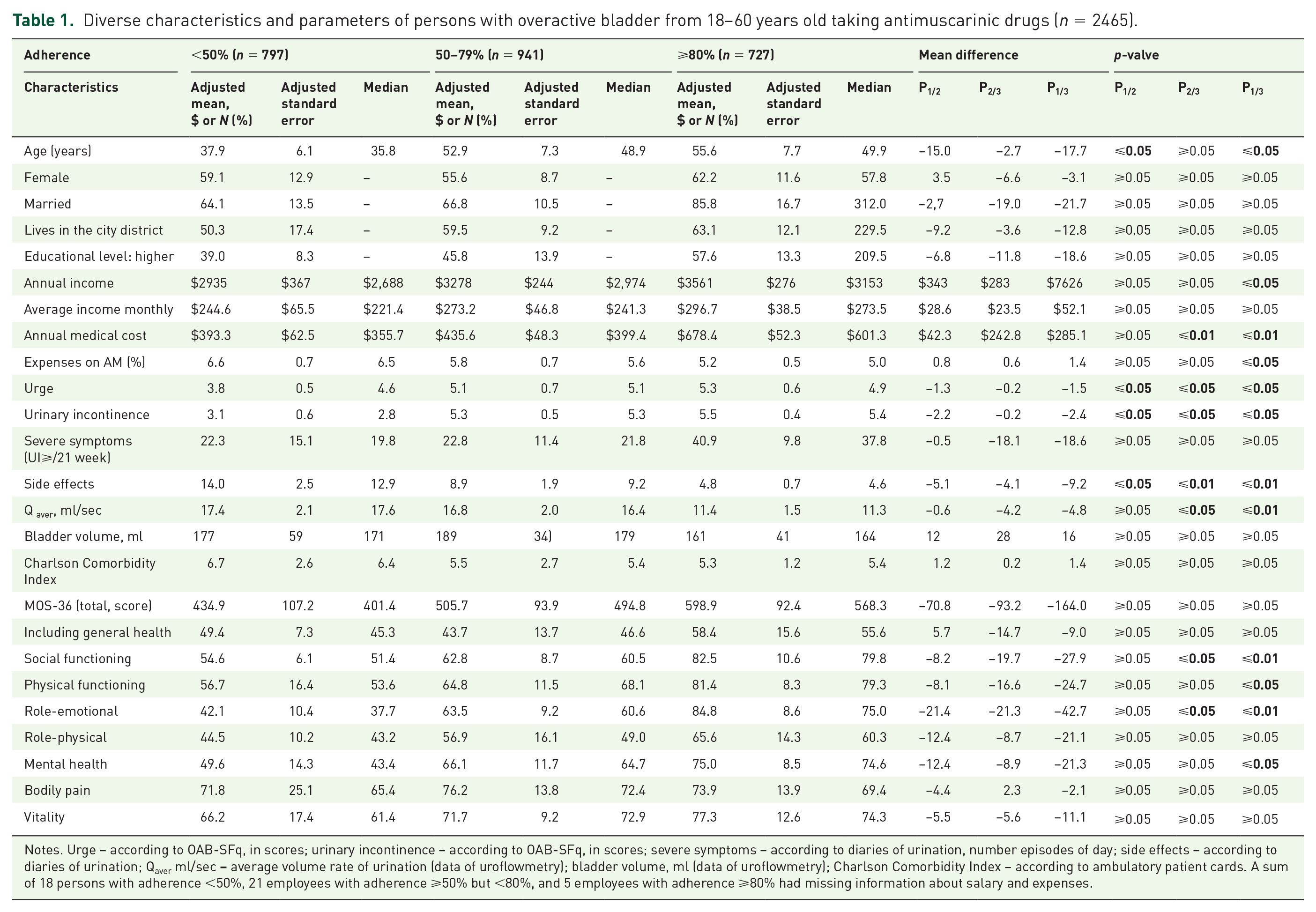
Notes. Urge – according to OAB-SFq, in scores; urinary incontinence – according to OAB-SFq, in scores; severe symptoms – according to diaries of urination, number episodes of day; side effects – according to diaries of urination; Qaver ml/sec
During the initial analysis of results, it was established that the age of resistant and moderately adherent patients was significantly higher than that of poorly adherent individuals (p ⩽ 0.05; p ⩽ 0.05), that resistant patients have high annual income and medical costs (p ⩽ 0.05; p ⩽ 0.01) and a low share of expenses for the purchase of AMs (p ⩽ 0.05). Values of urge and urinary incontinence parameters varied in all three cohorts (p ⩽ 0.05; p ⩽ 0.05). The percentage of individuals with side effects in cohorts 2 and 3 was lower (p ⩽ 0.05; p ⩽ 0.01) than in cohort 1. The average volumetric urination flow rate in persistent patients was lower than in other cohorts (p ⩽ 0.05; p ⩽ 0.01). When analyzing health parameters affecting the quality of life (MOS-36) it was established that the level of social functioning and role-emotional state in resistant patients differs from the same parameters in patients from other cohorts (p ⩽ 0.05; p ⩽ 0.01 in both cases). The level of mental health and physical functioning state between the most and least adherent patients are not statistically uniform (p ⩽ 0.05; p ⩽ 0.05).
Thus, at the first stage of the analysis we have established those objective parameters that varied in cohorts of individuals with different adherence levels. Table 2 shows the results of a comparison of these parameters in patients with different subjective reasons for the refusal of treatment. The number of urge episodes in subgroup 1 (medical reasons for refusal) exceeded values in other subgroups (p ⩽ 0.01; p ⩽ 0.05) and the sample average at both control points (p ⩽ 0.01; p ⩽ 0.01). The number of urinary incontinence (UI) episodes in this subgroup was higher than the average (CP1, CP2: p ⩽ 0.05; p ⩽ 0.05) and in subgroup 2 (economic reasons for refusal), but was statistically uniform when compared with subgroup 3 (social and psychological reasons). The Qaver indicator in subgroup 1 was also significantly lower than in subgroup 2 (p ⩽ 0.05), but did not differ from the value in subgroup 3. The number of side effects in subgroup 1 was higher than in other subgroups (p ⩽ 0.01; p ⩽ 0.01) and at both control points (p ⩽ 0.01; p ⩽ 0.01).
Objective status of medical, economic and social markers in individuals with various subjective reasons for the refusal of antimuscarinic treatment (n = 2465).

Notes. SD – standard deviation is indicated in parentheses; p-valve – significance of differences. Medical parameters: U – urge (data of OAB-SFq, in scores), UI – urinary incontinence (diaries of urination, the number of episodes per day), Qaver ml/sec
Economic indicators annual income (AI), annual medical cost (AMC) and percentage annual expenses on AM (PAEAM) significantly differed in subgroups 1 and 2 (p ⩽ 0.05; p ⩽ 0.05; p ⩽ 0.05); AI and PAEAM indicators in subgroups 2 and 3. The average values of social and psychological characteristics in subgroup 3 were not significantly different from the values in subgroup 2 (except for RE) and subgroup 1, as well as from the average group values.
Figure 2 shows the monthly percentage of individuals who refused treatment for a variety of reasons. The percentage of individuals who stated that the reason for their refusal of treatment were economic problems, and the percentage of individuals whose values of economic markers deviated from average values in the cohort were statistically uniform (Figure 2(a)). This applies to the percentage of individuals who stated that the reasons for their refusal of treatment are medical, and the percentage of patients with health status markers significantly deviated from average values (Figure 2(b)). The percentage of individuals reporting social and psychological reasons for the refusal of treatment was significantly lower than the percentage whose objective status parameters of the social adaptation state and psychological comfort level demonstrated deviations (Figure 2(c)).

A percentage ratio of monthly treatment refusals according to the subjective evaluation of patients and the percentage of individuals who refused treatment with altered economic, medical, social and psychological status markers within the follow-up period. (a) The percentage of refusals for economic reasons, and percentage of individuals with altered economic characteristics. (b) The percentage of refusals for medical reasons and the percentage of individuals with objective medical characteristics different from average values. (c) The percentage of refusals for social and psychological reasons and the percentage of individuals with altered social and psychological characteristics.
Discussion
A total of 47.9% of patients maintained adherence within the first 6 months, and 25.2% within the follow-up period. The average time of reaching the 30-day break in AM administration was 177 days.
Resistant patients were characterized by older age, higher annual incomes and medical costs, a low share of AM expenses, high frequency of manifestations of urge and urinary incontinence symptoms, low incidence of side effects and lower average volumetric urination flow rate. In the cohort of resistant patients, the level of social functioning and role-emotional status was significantly higher than that in moderately and poorly resistant patients.
According to the protocol, we have moved beyond the study of the effect of pharmacological differences between AMs, as pharmacological factors affecting resistance are deemed to be sufficiently studied,6,8,12,14,15 and focused on the analysis of reasons for refusal of treatment, indicated by the patients themselves and objective parameters of their status. A significant percentage of patients indicated social and economic factors as reasons for the refusal of the proposed therapy. They include high expenses relating to AM purchases, 17 low solvency, 19 job loss and decreased performance, which may be related to financial inability. 29 According to our data, 18.5% of patients discontinued treatment during the year for the above and other economic reasons, which is close to the results of other researchers and is confirmed by objective data on the income level and expenses of patients (these were altered in 20.4%). This percentage is comparable to the proportion of low-income individuals in the region.
According to the literature, the percentage of patients indicating medical reasons for the refusal of treatment is 64.2–75.5% on average.30,12 According to our findings, these reasons are indicated by a smaller number of patients (31.9% of the total number of patients), and this result does not significantly differ from the percentage of patients with objectively confirmed disorder of the lower urinary tract (35.9%). This result may be related to a relatively low number of side effects, the active use of latest-generation drugs providing quick and pronounced therapeutic effect, perhaps with a significant presence in a sample of elder persons not having high expectations associated with drug administration.
Several items of research provide data on aversion to the drug administration (11%) 31 including other psychological and social14,32 problems indicated by patients as reasons for the refusal (dispersion of the percentage of refusals associated with these reasons reaches 3–25%, and more in different authors). According to our results, in not less than 24.1% of cases of refusal of treatment patients indicate social and psychological reasons. However, the percentage of patients with non-average values of social and psychological status markers was 35.9%. In nearly the entire follow-up period, the percentage of individuals who stated social and psychological reasons for the refusal was significantly lower than the percentage of patients with objectively altered status parameters of social and psychological wellbeing. Perhaps this is related to the conscious or unconscious resistance on the part of patients to recognizing social and, in particular, psychological problems, to avoid statement of a social dysfunction, or lack of adequate analysis of their behavior.
We were aware of certain limitations of the experiment design. The comparison of the adherence to AM and other OAB treatments, a study of the adherence to treatment in other forms of urination disorders, a study of a number of economic characteristics have been left outside the research. These and some other issues require further study.
During the follow up for unrelated reasons, 71 individuals (2.9%) discontinued their participation in the experiment. It was not possible to collect comprehensive data on the patients’ economic statuses in 39 cases (1.6%).
Conclusion
This research allowed us to identify some factors affecting the adherence to medical prescriptions during long-term OAB treatment with antimuscarinic drugs when objectively monitoring health, socioeconomic and psychological statuses of patients.
In this research, conducted through building and analysis of regression models of different factors, it was determined that in the case of patients indicating economic and medical reasons for the refusal of treatment, these data are confirmed by objective health and economic status markers. However, the percentage of patients indicating social and psychological factors as reasons for the refusal of treatment is significantly lower than the percentage of individuals with actually disturbed social and psychological status. These results require further study, in our opinion, and can be used by practicing urologists and allied specialists to predict the efficacy of prescribing AMs and to evaluate the risk of refusal of treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.