
Abstract
Sunitinib is an oral multi-targeted tyrosine kinase inhibitor (TKI) that targets various receptors, including vascular endothelial growth factor receptors (VEGFRs). Sunitinib received approval in 2006 and became a standard treatment option in the first-line treatment of metastatic renal cell cancer (mRCC) after a phase III trial showed superiority compared with interferon alpha (IFN-α). Sunitinib has also shown activity in second-line treatment in several trials. Most of the combination trials with sunitinib with various agents have led to considerable toxicity without improving efficacy. Sunitinib alone causes significant side effects and has a distinct profile with diarrhoea, hypertension, skin effects hypothyroidism, fatigue and nausea of special interest. The recommended dose of sunitinib in mRCC is 50 mg orally daily for 4 weeks, followed by 2 weeks off treatment (4/2 schedule). An alternative 2 weeks on, 1 week off schedule (2/1 schedule) seems to be of similar efficacy and better tolerability and could be more widely used in the future. An intermittent treatment strategy with a stop in remission and re-induction after progression showed efficacy in smaller trials and is currently being evaluated in a phase III trial. Direct comparison of sunitinib with pazopanib in first-line treatment showed a similar efficacy for both TKIs with a distinct toxicity profile. Data from two phase II trials showed that sunitinib has also activity in non-clear cell cancer and is an option due to a lack of better alternatives. Currently, after immune checkpoint inhibitors have shown very promising results in the second-line treatment of RCC, they are being tested in a number of phase III trials in the first-line setting. The future will show the position of sunitinib in the first-line treatment of RCC in the era of the immune checkpoint inhibitors.
Introduction
Sunitinib (sunitinib malate, Sutent®, SU11248, Pfizer Inc.) is an oral multi-targeted tyrosine-kinase inhibitor (TKI) of vascular endothelial growth factor (VEGF) receptors (VEGFRs), platelet-derived growth factor (PDGF) receptors (PDGFRs), stem cell factor receptor (KIT) and FMS-like tyrosine kinase-3 (FLT3) receptor, as well as macrophage colony-stimulating factor receptor (CSF-R) and glial cell-line derived neurotrophic factor receptor [Farrell et al. 2003; Mendel et al. 2003; Abrams et al. 2003; Osusky et al. 2004; Patyna et al. 2008; Chow and Eckhardt, 2007].
In 2012, renal cell cancer (RCC) accounted for an estimated 388,000 new cases (2.4% of all malignancies) and an estimated 144,000 deaths (1.7% of all deaths caused by cancer) worldwide [Ferlay et al. 2015]. Clear cell RCC is the most common histological subtype with a proportion of approximately 80% of all RCCs [Moch et al. 2000; Leibovich et al. 2010] and commonly associated with an inactivation of the von Hippel-Lindau (VHL) tumour suppressor gene [Kaelin, 2007]. VHL inactivation leads to an up-regulation of VEGF, PDGF and other promoters of angiogenesis and cellular growth, proliferation and migration. VEGF is seen as the key mediator of angiogenesis, which is essential for cancer development and growth [Rini, 2009; Carmeliet, 2005]. VEGF overexpression and a high degree of vascularization is one of the features of RCC [Herbst et al. 1998; Jacobsen et al. 2004]. Therefore, drugs inhibiting the VEGF pathway, such as sunitinib, play an important role in the treatment of RCC.
The aim of this review is to provide an overview of the role of sunitinib in the management of metastatic RCC (mRCC) and to describe current schedules and toxicity management strategies. We also briefly discuss the use of sunitinib in the context of other targeted therapies and the newer immunotherapy agents.
Early trials
RCC is largely refractory to cytotoxic agents [Medical Research Council Renal Cancer Collaborators, 1999; Motzer et al. 1996]. Before the era of VEGF-targeted therapy, systemic treatment for advanced RCC was mainly limited to cytokine therapy with interleukin-2 (IL-2) or interferon-alpha (IFN-α), both of which effected objective responses, but in a small proportion of patients these agents were also associated with significant toxicities [McDermott et al. 2005; Coppin et al. 2005; Medical Research Council Renal Cancer Collaborators, 1999].
Sunitinib initially demonstrated promising antitumour activity in a phase I trial in patients with acute myeloid leukaemia [Fiedler et al. 2004]. Following this, a phase I dose-escalation study in solid malignancies was published in which three out of four patients with RCC had a response [Faivre et al. 2006]. Sunitinib was given orally in a 4 weeks on, 2 weeks off schedule (4/2 schedule) in order to allow patients to recover from the potential bone marrow and adrenal toxicity that had been observed in animal models.
Subsequently, two open-label single-arm multicentre phase II trials of sunitinib in patients with mRCC who had progressed on first-line cytokine treatment were published by Motzer and colleagues [Motzer et al. 2006a, 2006b].
In the first trial, 40% of the patients had a partial response, as assessed by the ‘Response Evaluation Criteria in Solid Tumours’, RECIST [Therasse et al. 2000], and in addition 27% achieved stable disease lasting ⩾3 months. The median time to progression (TTP) was 8.7 months [Motzer et al. 2006a]. The second trial confirmed the antitumour efficacy of sunitinib. Partial responses were achieved in 34% of the patients and the median progression free survival (PFS) was 8.3 months [Motzer et al. 2006b]. A pooled analysis of these two phase II trials with a total of 168 patients showed an objective response rate (ORR) of 42%, a rate of stable disease of ⩾3 months of 24% and a median PFS of 8.2 months [Motzer et al. 2006b].
First-line trials
After having shown remarkable efficacy in the first two phase II trials, sunitinib was compared with IFN-α at first-line in a randomized phase III landmark trial in patients with clear cell mRCC [Motzer et al. 2007, 2009a]. A total of 750 patients were enrolled and received either sunitinib (50 mg/day on a 4/2 week schedule) or IFN-α subcutaneously at a standard dose of 9 MU three times weekly. The primary endpoint of median PFS was significantly longer in the sunitinib arm (11 months) compared with the IFN-α arm (5 months), corresponding to a hazard ratio (HR) of 0.42 [95% confidence interval (CI) 0.32–0.54; p < 0.001]. Sunitinib also resulted in significantly higher ORRs than IFN-α (31% versus 6%; p < 0.001). The toxicity assessment showed a significantly higher proportion of grade 3 or 4 treatment-related fatigue in the IFN-α group (p < 0.05), whereas grade 3 or 4 diarrhoea, vomiting, hypertension and hand-foot syndrome were significantly more frequent in the sunitinib group (p < 0.05 for all comparisons). However, quality of life as assessed by the Functional Assessment of Cancer Therapy (FACT), general (FACT-G) and Kidney Symptom Index (FKSI) questionnaires [Cella et al. 1993, 2006] was significantly better in the sunitinib group [Motzer et al. 2007].
In an updated analysis, the median overall survival (OS) was significantly longer in the sunitinib group, 26.4 months compared with 21.8 months for the IFN-α group (HR = 0.818; 95% CI 0.669–0.999; p = 0.049 by stratified log-rank test). However, in pre-stratified poor-risk patients (Memorial Sloan-Kettering Cancer Centre criteria) [Motzer et al. 2002], the median PFS as well as the median OS did not significantly differ between the sunitinib group and the IFN-α group although the number of patients in the poor-risk group was small, at only 48 patients [Motzer et al. 2009a].
Data from the large expanded access programme (EAP) in a broad, more heterogeneous population of 4543 patients who received sunitinib as first-line treatment, or after progression on cytokine or anti-angiogenic treatment, showed an overall ORR of 16%, a median PFS of 9.4 months and an OS of 18.7 months. The median PFS for subgroups of special interest was 10.1 months for elderly patients (age ⩾65 years), 3.5 months for patients with an Eastern Cooperative Oncology Group (ECOG) performance status (PS) ⩾2, 6 months for non-clear cell histology, and 5.3 months for patients with brain metastases. Thrombocytopenia (10%), fatigue (9%), asthenia (7%), neutropenia (7%) and hand-foot syndrome (7%) were the most common grade 3/4 treatment-related adverse events. This study confirmed that sunitinib is effective and well-tolerated with manageable toxicities in a unselected group of patients [Gore et al. 2015].
On the basis of these trials, sunitinib received regulatory approval by the United States Food and Drug Administration (US FDA) and full marketing authorization by the European Medicines Agency (EMA) in 2007. It is still recommended as a first-line treatment option for advanced or metastatic predominantly clear cell RCC for patients with good, intermediate and poor-risk disease [NCCN Panel Members, 2016a; Escudier et al. 2014a].
Table 1 gives an overview of the early and first-line trials of sunitinib.
Sunitinib early and first-line trials.

CI, confidence interval; EAP, early access program; HR, hazard ratio; IFN-α, interferon-alpha; mRCC, metastatic renal cell cancer; NA, not available; ORR, objective response rate; OS, overall survival; PFS, progression free survival; TTP, time to progression.
p < 0.001.
HR = 0.539 (95% CI 0.451–0.643; p < 0.001).
HR = 0.818 (95% CI 0.669–0.999; p = 0.049 by stratified log-rank test).
Second-line and further-line trials
The use of cytokines as a first-line treatment has decreased considerably so the emphasis of this section will be on the data relating to the role of sunitinib following other VEGF-targeted agents.
Several retrospective studies investigated the sequential use of sunitinib after sorafenib, another multi-targeted TKI with an overlapping but not identical kinase inhibition profile [Wilhelm et al. 2004]. Sunitinib showed activity after sorafenib in these strategies [Eichelberg et al. 2008; Dudek et al. 2009; Sablin et al. 2009; Zimmermann et al. 2009; Porta et al. 2011a]. In another retrospective study, patients who progressed after first-line sunitinib and had received subsequent therapies were re-challenged with sunitinib at the time of further progression. Sunitinib showed activity (ORR 22% and median PFS 7.2 months upon re-challenge) without additional or increased toxicities [Zama et al. 2010]. In a prospective study 22 patients with mRCC and progression after sorafenib were treated with sunitinib. The median PFS on sunitinib was 21.5 weeks with a 1-year survival of 60% [Zimmermann et al. 2009]. The open-label phase III SWITCH trial evaluated the sequential administration of sorafenib followed by sunitinib (So-Su) versus sunitinib followed by sorafenib (Su-So) on progression or intolerable toxicity in patients with mRCC. The primary endpoint was PFS following the end of the sequence of therapy, sometimes known as PFS2. There was no statistically significant difference between the two treatment sequences, median PFS2 was 12.5 months for So-Su and 14.9 months for Su-So (p = 0.5 for superiority). Median PFS to first-line treatment was 5.9 months for sorafenib and 8.5 months for sunitinib (NS; p = 0.9 for superiority), while at second-line it was 2.8 months for sorafenib and 5.4 months for sunitinib (HR 0.55, p < 0.001 for superiority) [Eichelberg et al. 2015]. The results of these studies are suggestive of a degree of non-cross-resistance between sunitinib and sorafenib.
Rini and colleagues published a phase II multicentre trial with sunitinib as second-line treatment following disease progression after bevacizumab-based first-line treatment. The primary endpoint, ORR was 23%. Median PFS was 30.4 weeks and the median OS was 47.1 weeks. The study showed that sunitinib has substantial antitumour activity in patients progressing after bevacizumab-based therapy [Rini et al. 2008a].
Table 2 provides an overview of the second-line or further line trials of sunitinib.
Sunitinib second-line trials (post VEGF-targeted agents).

CR, complete response; NA, not available; ORR, objective response rate; PFS, progression free survival; PR, partial response; VEGF, vascular endothelial growth factor.
Sunitinib re-challenge for ⩾ 3rd line treatment.
Combination trials
A number of studies have investigated sunitinib in combination with different agents.
The addition of IFN-α to sunitinib was assessed in a phase I dose-finding trial in treatment naïve patients with clear cell mRCC. All patients developed grade 3/4 treatment-related adverse events and partial responses were only achieved in 12% of patients [Motzer et al. 2009b]. These data compared unfavourably with those from the pivotal phase III trial of sunitinib alone which demonstrated partial responses in 31% of the patients [Motzer et al. 2007]. The combination of sunitinib with IFN-α was therefore not investigated further.
The tolerability and efficacy of sunitinib in combination with bevacizumab was explored in a phase I trial in patients with progressive mRCC. The ORR was high (52%) but treatment resulted in frequent grade 3/4 toxicities such as hypertension (60% grade 3/4), proteinuria and thrombocytopenia as well as thrombotic microangiopathy. Furthermore, 48% of patients had to discontinue treatment due to toxicity [Feldman et al. 2009]. In an expanded cohort of five patients in another phase I trial of the combination of sunitinib and bevacizumab three out of five patients had laboratory evidence of thrombotic microangiopathy [Rini et al. 2010a]. The high rates of grade 3/4 toxicity including thrombotic microangiopathy precluded further investigation of this combination.
The combination of sunitinib and everolimus (an oral inhibitor of mammalian target of rapamycin pathway, mTOR) in advanced RCC was tested in two phase I trials. Both trials reported a high incidence of grade 3/4 toxicity, and the second trial was closed prematurely for this reason [Molina et al. 2012b; Kanesvaran et al. 2015].
The combination of sunitinib with temsirolimus, an intravenously administered mTOR pathway inhibitor was tested in a phase I study in patients with advanced RCC. The trial was terminated early due to dose-limiting toxicity that was seen at low doses of both drugs and the conclusion of the study investigators was that this combination should not be taken forward [Patel et al. 2009].
A recently published phase II trial investigated the combination of sunitinib with trebananib, an intravenous recombinant-Fc fusion protein that neutralizes the receptor-ligand interaction between Tie2 and angiopoietin-1/2. Trebananib was administered at two different doses (cohort A at 10 mg/kg and cohort B at 15 mg/kg). The rate of grade 3/4 adverse events was 58% (cohort A) and 59% (cohort B), respectively. The ORRs were 58% (cohort A) and 63% (cohort B) and the median PFS were 13.9 months and 16.3 months in cohort A and B, respectively. These results suggest a potential benefit for this combination, but it appears to be associated with significant toxicity [Atkins et al. 2015].
In a phase II trial, published in 2015, AGS-003, an autologous dendritic cell-based immunotherapy was tested in combination with sunitinib in patients with intermediate and poor-risk mRCC according to Memorial Sloan-Kettering Cancer Center (MSKCC) and Heng risk scores [Motzer et al. 2004; Heng et al. 2009]. The ORR was 43%, the median PFS was 11.2 months and 43% of the patients had grade 3 toxicities [Amin et al. 2015]. Given the promising results of this trial, an international phase III randomized trial (ADAPT) is ongoing (phase III Trial of Autologous Dendritic Cell Immunotherapy (AGS-003) Plus Standard Treatment of Advanced Renal Cell Carcinoma (RCC; ADAPT) [ClinicalTrials.gov identifier: NCT01582672]).
Preliminary results from a phase I trial (Checkmate 016) of sunitinib or pazopanib and nivolumab (anti-PD1 AB) have been published and show evidence of activity for the combination (ORR 52% for nivolumab plus sunitinib and 45% for nivolumab plus pazopanib) with a manageable safety profile [Amin et al. 2014; ClinicalTrials.gov identifier: NCT01472081].
Table 3 gives an overview of the combination trials.
Combination trials in renal cell carcinoma.

2/1, 2 weeks on, 1 week off schedule; 4/2, 4 weeks on, 2 weeks off schedule; ALT, alanine aminotransferase; IFN-α, interferon-alpha; iv, intravenously; NA, not available; od, once daily; ORR, objective response rate; OS, overall survival; PD, progressive disease; PFS, progression free survival; q1w, weekly; q2w, every 2 weeks; q12w, every 12 weeks; t.i.w., three times a week; TTP, time to progression
Toxicity management
Sunitinib is associated with a significant burden of side effects. Adverse events of any grade were reported in approximately 95% of the patients in the large global sunitinib EAP representing a ‘real world’ population, although the incidence of grade 3/4 adverse events was 46% in patients with ECOG PS ⩾2 and 56% with ECOG zero or one. The most frequent adverse events of any grade were diarrhoea (47%), fatigue (40%), nausea (36%) and decreased appetite (31%) [Gore et al. 2015].
Toxicities from this EAP and the first-line phase III trial are listed in Tables 4 and 5.
Treatment related adverse events of interest and that occurred in more than 10% of patients.

Only grade 3.
mRCC, metastatic renal cell carcinoma; NA, not available.
Treatment related laboratory abnormalities of interest and that occurred in more than 10% of patients.

ALT, alanine aminotransferase; AST, aspartate aminotransferase; EAP, early access program; mRCC, metastatic renal cell carcinoma.
Only grade 3.
Toxicities of special interest
Hypertension
The incidence of grade 3/4 hypertension was 6% in the EAP [Gore et al. 2015]. Hypertension is regarded to be a class effect of angiogenesis inhibitors that target VEGF signalling [Sica, 2006; Willett et al. 2004; Yang et al. 2003; Ahmad and Eisen, 2004; Escudier et al. 2007a; Soria et al. 2009]. Patients receiving sunitinib should be advised to measure their blood pressure at home and once hypertension occurs, antihypertensive treatment should be initiated with standard antihypertensive drugs. As sunitinib is primarily metabolized by the cytochrome P-450 (CYP) isoenzyme system, namely CYP3A4, physicians should avoid known CYP3A4 inhibitors such as diltiazem or verapamil as there are no data available on the safety of their concomitant use with sunitinib to date [Houk et al. 2009].
Hypothyroidism
Grade 3/4 hypothyroidism occurred in 4% of the patients on sunitinib [Gore et al. 2015]. In a smaller, more detailed study of 66 patients treated with sunitinib, 85% had at least one abnormal thyroid function test, consistent with hypothyroidism and 71% of all patients had signs or symptoms that were possibly related to hypothyroidism. The thyroid function abnormality was detected early within a median of two cycles (range 1–14). Overall, 26% of all patients needed a thyroid hormone replacement, which improved symptoms in 50% of the patients [Rini et al. 2007]. In another analysis of 42 patients, 62% developed abnormal serum thyroid stimulating hormone concentrations and 36% developed persistent, primary hypothyroidism. The risk for the development of hypothyroidism was increased with the duration of sunitinib therapy [Desai et al. 2006]. Measurement of the thyroid function should be performed at baseline and thereafter on a regular basis; most would recommend 3-monthly.
Cardiac toxicity
A decrease in the left ventricular ejection fraction (LVEF) is the main cardiac toxicity of sunitinib. Grade 3 LVEF decline was reported in 3% with no grade 4 decline in the phase III first-line trial [Motzer et al. 2009]. Patients with cardiac risk factors such as recent history of myocardial infarction, unstable angina or symptomatic congestive heart failure (CHF) were excluded from the sunitinib trials. It is not known if patients with pre-existing cardiac risk factors are at a higher risk to develop drug-related LVEF decline. Nevertheless, these patients should be carefully monitored for clinical signs and symptoms of CHF while receiving sunitinib. They should have baseline and periodic evaluations of LVEF [Pfizer Canada Inc., 2014]. The frequency of monitoring depends on the severity of the baseline cardiac function and co-morbidities. In patients without cardiac risk factors, a baseline evaluation of ejection fraction should be considered. In the presence of clinical manifestations of CHF, discontinuation of sunitinib is recommended [Pfizer Canada Inc., 2014].
Skin toxicity
Skin toxicity typically occurs after 3–4 weeks of a treatment [Faivre et al. 2006]. Hand-foot syndrome (palmar-plantar erythrodysesthesia) is one of the most common skin side effects, with grade 3/4 events reported in 7% of patients in the EAP [Gore et al. 2015]. As no randomized trials exist to determine the best management strategy for hand-foot syndrome, recommendations from expert opinion are the best guide. Preventative measures include manicure and pedicure, wearing thick cotton gloves, and the avoidance of hot water, constrictive footwear and excessive friction. If a patient develops hand-foot syndrome, topical treatment with intensive moisturizing creams such as those containing urea or lanolin is recommended. If grade ⩾2 hand-foot syndrome occurs, a steroid-based cream should be added and a dose reduction or break of sunitinib should be considered [Lacouture et al. 2008; Kollmannsberger et al. 2007; Pfizer Canada Inc., 2014].
Diarrhoea
The incidence of grade 3/4 diarrhoea was 5% in the EAP [Gore et al. 2015]. Grade 1/2 diarrhoea can commonly be managed by oral hydration and oral antidiarrheal agents such as loperamide as needed. Sunitinib treatment should be interrupted for grade 3/4 diarrhoea until diarrhoea is grade 1 or less. Usually, the diarrhoea resolves fast in the 2-week break between sunitinib cycles [Kollmannsberger et al. 2007; Motzer et al. 2006b; Pfizer Canada Inc., 2014].
Fatigue
Fatigue is one of the most common adverse events with sunitinib but also in cancer patients generally. Grade 3 fatigue which limits self-care activities of daily living [National Institute of Cancer, 2010] occurred in 9% of the patients in the EAP [Gore et al. 2015]. It is advisable to undertake an assessment to identify potentially treatable contributing factors of fatigue such as anaemia, hypothyroidism, depression, pain, nutritional deficits/imbalances or sleep disturbance. General strategies for management of fatigue include light physical activity such as walking, use of welcome distractions such as listening to music, limiting naps during the day to under 1 h to not interfere with night-time sleep quality, eating well, and drinking plenty of fluids. Pharmacological intervention with psychostimulants (methylphenidate) may improve fatigue in some patients [NCCN Panel Members, 2016b; Kollmannsberger et al. 2007; Minton et al. 2010].
Nausea
The emetogenic potential of sunitinib is low [Grunberg et al. 2011]. While nausea of any grade has been reported by 36% of the patients with sunitinib, grade 3/4 nausea has only been noted in 2% in the EAP. If nausea occurs, common antiemetics should be used. However one should be aware of the concomitant use of sunitinib with antidopaminergic agents as domperidone and 5HT3 antagonists such as ondansetron as they all have the potential to prolong the QTc interval [Kollmannsberger et al. 2007; Rossi and Giorgi, 2010; Brygger et al. 2014]. Practical guidelines for the management of nausea are published by the National Comprehensive Cancer Network (NCCN) and the European Society of Medical Oncology (ESMO) [NCCN Panel Members, 2016c; Roila et al. 2010].
For further information about management of sunitinib toxicity in RCC see the comprehensive review by Kollmannsberger and colleagues [Kollmannsberger et al. 2007].
Toxicity and outcome
Several of the above toxicities are thought to serve as independent predictive biomarkers for the treatment efficacy of sunitinib. The occurrence of treatment-related hypertension has been shown to be an independent biomarker of sunitinib efficacy. A large retrospective analysis included pooled data from 544 sunitinib-treated mRCC patients in the three prospective clinical trials. Patients with sunitinib-induced hypertension had better outcomes than those without treatment-induced hypertension in terms of ORR (54.8% versus 8.7%; p < 0.001), median PFS (12.5 months versus 2.5 months; p < 0.001) and median OS (30.9 months versus 7.2 months; p < 0.001) [Rini et al. 2011]. In another large retrospective analysis of five randomized trials, with a total of 770 patients treated with sunitinib, the occurrence of hypertension as well as neutropaenia under treatment was associated with a prolonged PFS and OS, independent of baseline prognostic factors [Donskov et al. 2015].
Two analyses have suggested a correlation between good outcome and the development of hypothyroidism while on sunitinib [Kust et al. 2014; Nearchou et al. 2015]. In a retrospective analysis of 41 patients with mRCC treated with sunitinib, the occurrence of symptomatic hypothyroidism was associated with longer median PFS (25.3 months versus 9.0 months; p = 0.042) but without a difference in median OS [Kust et al. 2014]. However, meta-analysis found no statistical significant difference in the PFS between patients who developed hypothyroidism on sunitinib therapy and unaffected patients (HR 0.82; p = 0.22; six studies, 250 patients). An OS benefit was observed in patients who developed hypothyroidism (HR 0.52; p = 0.01; four studies, 147 patients), but this should be interpreted with caution, because the trials did not report data for subsequent treatment after sunitinib [Nearchou et al. 2015].
Effects of sunitinib on the immune system
Sunitinib and other multi-targeted TKIs inhibit signalling pathways which are also relevant in the immune system. For example, the administration of sunitinib has shown to increase the plasma VEGF levels [Deprimo et al. 2007]. VEGF, on the other hand, is able to inhibit the ability of mature dendritic cells to stimulate allogeneic T-cells [Mimura et al. 2007; Porta et al. 2011b].
Several studies have shown that sunitinib may enhance antitumour activity of the immune system:
In a mouse model study, treatment with sunitinib reduced the number of myeloid-derived suppressor cells (MDSCs) and T-regulatory cells and resulted in a reduction of immune suppressive cytokines and co-stimulatory molecules such as IL-10, and in an enhanced expression of Th1 cytokine IFN-gamma. Even more importantly, the expression of the negative co-stimulatory molecules CTLA4 and PD-1 in both CD4 and CD8 T-cells, and PDL-1 expression on MDSCs and plasmacytoid dendritic cells was significantly reduced by sunitinib treatment [Ozao-Choy et al. 2009].
In an in vitro trial, treatment with sunitinib in mRCC patients was found to result in a significant reduction in MDSCs [Ko et al. 2009], which are usually increased in RCC patients and represent a mechanism by which tumours induce T-cell suppression [Kusmartsev et al. 2008; Ozao-Choy et al. 2009]. This MDSC reduction was correlated with reversal of type-1 T-cell suppression as well as a reversal of T-regulatory cells elevation [Ko et al. 2009].
Immune suppression which includes a shift from a type-1 to a type-2 T-cell cytokine response and an enhanced T-regulatory cell expression has been reported in patients with mRCC. It has been shown that both can be reversed by sunitinib [Finke et al. 2008].
A disturbed myeloid lineage development with impaired dendritic cell differentiation may contribute to tumour immune escape. After one cycle of sunitinib, dendritic cell rates recovered and the myeloid lineage distribution was normalized [van Cruijsen et al. 2008].
However, results from another study imply, that sunitinib may also have immune suppressive effects.
Sunitinib inhibited the proliferation of primary human T-cells from normal healthy volunteers and also from RCC and other cancer patients. This inhibition was recoverable after drug withdrawal [Gu et al. 2010].
The current evidence suggests that sunitinib has a considerable impact on the immune system.
Most of the studies, but not all, show that sunitinib has mainly immune stimulatory effects; however the picture is not that clear.
A comprehensive review of immunological effects of multikinase inhibitors for RCC was published by Porta and colleagues [Porta et al. 2011b].
Sunitinib schedules
Four weeks on, 2 weeks off versus 2 weeks on, 1 week off
The standard schedule for sunitinib is 50 mg once daily for 4 weeks, followed by a rest of 2 weeks (4/2 schedule) to recover from side effects [Motzer et al. 2009a].
In a pharmacokinetic analysis, data from one phase II study with a 4/2 schedule were analysed and showed, that the concentration of sunitinib and its active metabolite SU12662 decreases to pre-dose levels in the 2 weeks off period, indicating a potential lack of drug exposure during which the tumour could potentially progress [Houk et al. 2009].
An alternative continuous daily dosing schedule of sunitinib 37.5 mg once daily was compared with the standard intermittent schedule (50 mg once daily, 4/2 schedule) in a randomized phase III trial (Renal EFFECT trial). The ORR, median OS and adverse events were not significantly different. However, there was a trend towards an inferior median TTP in the continuous schedule and a statistically significant superiority in a composite endpoint of death, progression and disease-related symptoms for the 4/2 schedule (HR 0.77, p = 0.034) [Motzer et al. 2012]. On the basis of these results, the 4/2 schedule remains the standard sunitinib schedule.
Several retrospective studies showed promising results for a 2 weeks on, 1 week off schedule (2/1 schedule) in terms of efficacy and toxicity [Neri et al. 2012; Kletas et al. 2013; Atkinson et al. 2014; Kondo et al. 2014; Najjar et al. 2014; Bracarda et al. 2015]. The prospective randomized phase II RESTORE trial evaluated the efficacy and safety of the sunitinib 2/1 schedule versus the standard 4/2 schedule in 74 patients with clear cell mRCC. The 2/1 schedule resulted in a higher 6-month failure-free survival (the primary endpoint, 63% versus 44%) and median time to treatment failure (7.6 versus 6.0 months, HR = 0.57, p = 0.029) without compromising the efficacy in terms of ORR (47% versus 33%) and TTP (12.1 months versus 10.1 months). In addition the 2/1 schedule was associated with lower toxicity in terms of neutropaenia (all grades 61% versus 37%, p = 0.037) and fatigue (all grades 83% versus 58%, p = 0.017) and time to first dose reduction (HR = 0.35, p = 0.014) [Lee et al. 2015]. The major limitation of the trial was the small sample size, powered only to select the schedule with higher failure-free survival and not to detect differences in ORR, TTP, and OS.
The above data suggest, that patients who experience intolerable toxicities on a 4/2 schedule could switch to a 2/1 schedule, which would likely improve tolerability without compromising efficacy.
Table 6 provides an overview of the trials that investigated the 2/1 schedule.
Sunitinib schedules 4/2 versus 2/1 week schedule.
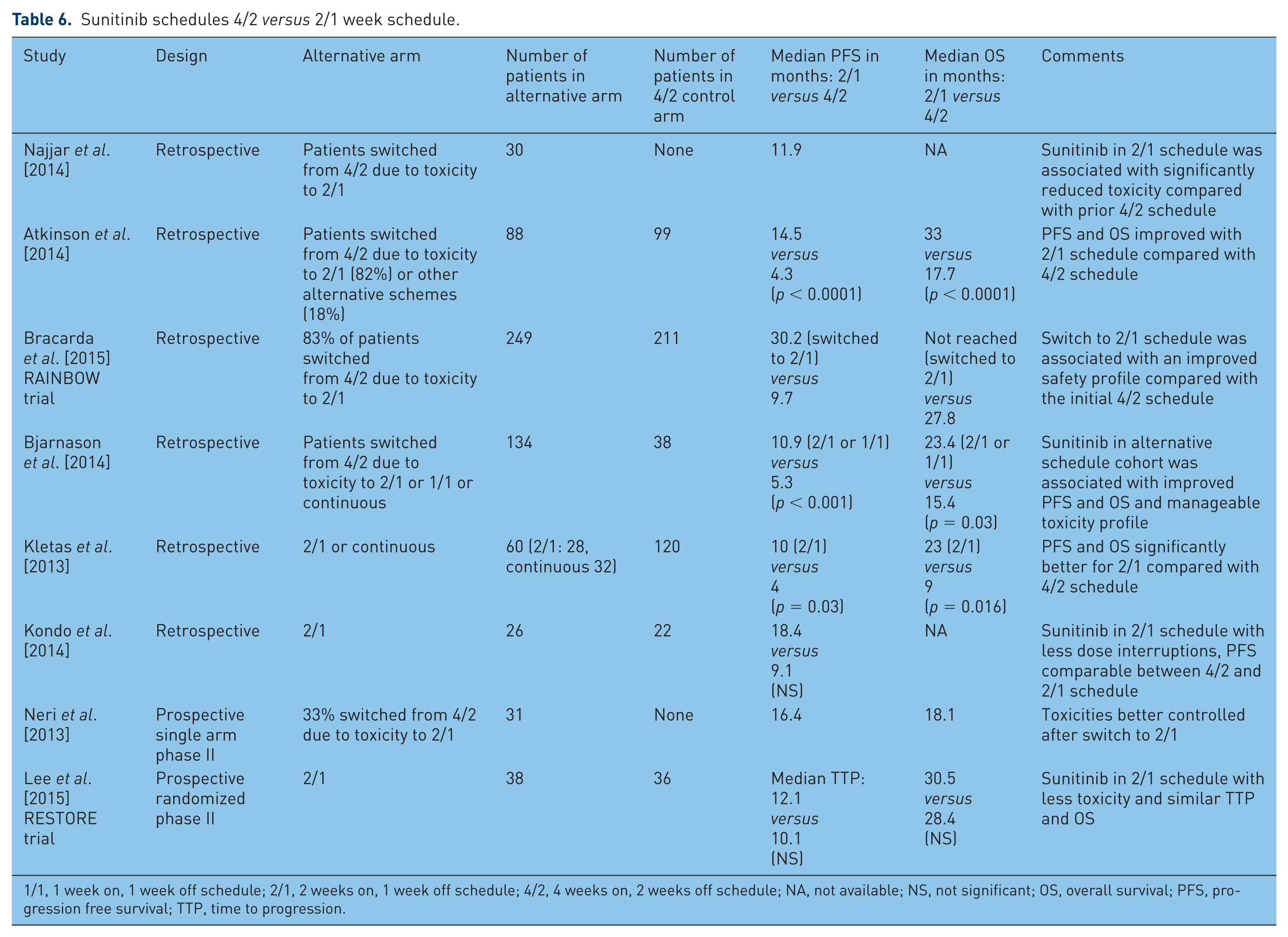
1/1, 1 week on, 1 week off schedule; 2/1, 2 weeks on, 1 week off schedule; 4/2, 4 weeks on, 2 weeks off schedule; NA, not available; NS, not significant; OS, overall survival; PFS, progression free survival; TTP, time to progression.
Stopping treatment in remission and reintroduction of sunitinib after progressive disease
Several smaller studies support the strategy of ‘drug holidays’ (i.e. sunitinib free intervals). A retrospective study with 11 patients reported the consequences of stopping sunitinib after a complete response, with or without surgical metastasectomy, had been achieved. At a median follow up of 8.5 months after sunitinib discontinuation, five patients had relapsed, with a median TTP of 6 months. However, reintroduction of sunitinib was effective in regaining disease control in all cases [Johannsen et al. 2009]. These results were confirmed in an updated analysis of 22 patients [Johannsen et al. 2011]. Preliminary results from a prospective phase II trial of intermittent sunitinib in previously untreated patients with mRCC were presented at the American Society of Clinical Oncology Annual Meeting, 2013. A total of 36 patients were initially treated for four cycles with sunitinib, and patients achieving a ⩾10% reduction in tumour burden had sunitinib withheld. Sunitinib was reintroduced for two cycles in those patients with an increase in tumour measurements of ⩾10% and discontinued after ⩾10% tumour burden reduction. This intermittent dosing was administered until RECIST-defined disease progression occurred. The ORR was 53% and most patients exhibited a stable saw-tooth pattern of tumour burden reduction on sunitinib with tumour burden increasing when off sunitinib. Toxicity resolved completely during the off-treatment periods. The results suggest that intermittent dosing of sunitinib may be better tolerated than standard fixed schedules without compromising efficacy [Rini et al. 2013]. Currently, a randomized multicentre phase III study is ongoing (STAR trial) that compares the conventional schedule of sunitinib 50 mg daily 4/2 weeks with a drug-free interval strategy, namely a treatment break after completion of at least four cycles and maximal radiological response until progressive disease (PD) and then a restart of sunitinib for a minimum of four cycles and maximal radiological response [Collinson et al. 2012].
Where does sunitinib fit in first-line treatment?
Sunitinib was compared in two trials with pazopanib, another approved and recommended TKI for first-line treatment for clear cell mRCC (Category 1 in NCCN guidelines and IA Level of recommendation in ESMO guidelines) [NCCN Panel Members, 2016a; Escudier et al. 2014a].
A randomized non-inferiority phase III trial (COMPARZ) involving 1100 patients compared pazopanib with sunitinib for the first-line treatment in clear cell mRCC. The two arms showed similar efficacy but a different safety profile. The study showed non-inferiority (predefined non-inferiority upper bound of the 95% CI < 1.25) for pazopanib for the primary endpoint median PFS, pazopanib 8.4 months versus 9.5 months with sunitinib (95% CI 0.90–1.22). Median OS, pazopanib 28.4 months versus sunitinib 29.3 months (HR 0.91; p = 0.28), was not significantly different, whereas the ORR was significantly higher in the pazopanib group (31% versus 25%; p = 0.03). Fatigue, hand-foot syndrome and thrombocytopenia were more frequent with sunitinib, while increased levels of alanine aminotransferase were higher with pazopanib; quality of life analysis favoured pazopanib [Motzer et al. 2013].
A second, smaller phase III trial (PISCES) supported the results of the COMPARZ trial. In total, 169 patients with mRCC were randomized to receive either first-line pazopanib for 10 weeks, followed by sunitinib for 10 weeks or the reverse sequence. The primary endpoint was patient preference at week 22. Significantly more patients preferred pazopanib (70%) to sunitinib (22%; p < 0.001). The main reasons for pazopanib preference were less fatigue and better overall quality of life [Escudier et al. 2014b]. Preliminary data from a retrospective analysis with 3606 patients with mRCC in a population-based setting, who received first-line treatment with sunitinib or pazopanib were recently presented. There was no difference in terms of ORR (sunitinib 30.3% versus pazopanib 25.7%; p = 0.09), median PFS (sunitinib 7.2 months versus pazopanib 6.8 months; p = 0.49) or median OS (sunitinib 20.1 months versus pazopanib 23.6 months; p = 0.19) between the two drugs [Morales et al. 2016].
Other first-line treatment recommendations in clear cell mRCC are bevacizumab plus IFN-α, sorafenib or axitinib. There are no phase III trials which compared these agents against sunitinib. The recommendation as a first-line treatment for bevacizumab plus IFN-α (NCCN guidelines 02.2016 category 1) is based on the results of two phase III trials (AVOREN and CALGB90206), which compared bevacizumab plus IFN-α versus IFN-α alone. Bevacizumab plus IFN-α improved the median PFS [Escudier et al. 2010; Rini et al. 2010b] but due to side effects and the inconvenience of IFN-α administration, this regimen is not widely used. Sorafenib is recommended as an option for first-line treatment for clear cell mRCC (category 2A in NCCN guidelines 02.2016, option in ESMO guidelines version 2014) [NCCN Panel Members, 2016a; Escudier et al. 2014a]. The evidence for sorafenib use at first-line is less strong as it has shown to prolong PFS compared with placebo after (mainly cytokine based) first-line treatment of patients with mRCC in a phase III trial (TARGET) [Escudier et al. 2007a], but failed to demonstrated superiority in a phase II trial against IFN-α in untreated patients [Escudier et al. 2009]. Axitinib, a second generation TKI has been investigated in a phase III trial against sorafenib in the first-line setting but failed to show an improvement [Hutson et al. 2013].
An overview of the first-line trials between sunitinib, pazopanib, bevacizumab plus IFN-α and sorafenib is set out in Table 7.
First-line randomized treatment trials for advanced clear cell RCC.

4/2, 4 weeks on, 2 weeks off schedule; Bid, twice daily; CI, confidence interval; HR, hazard ratio; IFN-α, interferon-alpha; NA, not available; od, once daily; ORR, objective response rate; OS, overall survival; PFS, progression free survival; q2w, every 2 weeks; RCC, renal cell carcinoma; sc, subcutaneously; t.i.w., three times a week.
Sunitinib and non-clear cell renal cancer
Non-clear cell RCC represents a histologically and genetically diverse group of cancers that arise from the kidney [Bitting et al. 2011; Shuch et al. 2015; Armstrong et al. 2016]. In contrast to clear cell RCC, the evidence for sunitinib treatment in non-clear cell RCC is less strong, as most of the phase III trials in RCC have restricted the enrolment to patients whose tumours are of clear cell subtype. Data are available from several retrospective and prospective phase II trials, which have focused on non-clear cell RCC histology, as well as from a subgroup analyses of the large EAP [Choueiri et al. 2008; Yildiz et al. 2014; Paglino et al. 2012; Shi et al. 2015; Molina et al. 2012a; Tannir et al. 2012; Ravaud et al. 2015; Lee et al. 2012; Gore et al. 2015].
Two randomized prospective phase II trials compared everolimus and sunitinib as first-line treatment in non-clear cell RCC. The first trial (ESPN), published an interim analysis in 2015. The results showed no benefit for everolimus in terms of median PFS (sunitinib 6.1 months, everolimus 4.1 months) and median OS (sunitinib 16.2 months, everolimus 14.9 months) and both agents demonstrated only modest efficacy [Tannir et al. 2015]. The second trial (ASPEN) showed a significant increase in the median PFS with sunitinib (8.3 months) versus everolimus (5.6 months; HR 1.41; p = 0.16, prespecified level of statistical significance 0.20) while the median OS was not different between the two groups. However, there was a difference in the treatment effect based on histological subtypes and prognostic risk groups [chromophobe subtype (median PFS 11.4 months versus 5.5 months)] and MSKCC poor-risk group (median PFS 6.1 months versus 4.0 months) favoured everolimus in exploratory nonpowered subgroups [Armstrong et al. 2016]. These differences demonstrate that non-clear cell RCC is not a homogeneous disease group and one should be aware of this in the interpretation of trial data.
Given these data, sunitinib is still recommended as an option for first-line treatment in non-clear cell RCC in current guidelines, especially for patients with good MSKCC risk scores [NCCN Panel Members, 2016a; Escudier et al. 2014a]. But as the overall efficacy in non-clear cell RCC remains poor with the current treatment options, the need for individual morphological subtype and genotype analysis and developing of new agents according to morphological subtype and genomic signalling remains urgent and patients should be offered entering into clinical trials if possible [Tannir et al. 2015; Armstrong et al. 2016].
Tables 8 and 9 give an overview of the different trials with sunitinib in advanced non-clear cell RCC.
Sunitinib in non-clear cell RCC.

ccSRCC, clear cell RCC with >20% sarcomatoid features; CDC, collecting duct carcinoma; ChRCC, chromophobe RCC; CI, confidence interval; EAP, expanded access programme; HR, hazard ratio; Minor CCRCC, minor clear cell RCC; NA, not available; OS, overall survival; PFS, progression-free survival; pRCC, papillary RCC; RCC, renal cell carcinoma; sarcD, sarcomatoid differentiation; SpcRCC, spindle cell type RCC; TrlC, translocation carcinoma.
Prespecified level of statistical significance for the study: two-sided type I error rate of 0.20).
Sunitinib in papillary and chromophobe non-clear cell RCC.

ChRCC, chromophobe RCC; OS, overall survival; PFS, progression-free survival; pRCC, papillary RCC; NA, not available; RCC, renal cell carcinoma.
Only sunitinib treated patients.
Is there a role for sunitinib as adjuvant treatment?
To date, the standard approach for patients with localized or locally-advanced RCC who have undergone nephrectomy is surveillance [NCCN Panel Members, 2016a; Escudier et al. 2014a]. Various studies did not show a benefit for immune treatment (cytokines or autologous tumour cell vaccines) versus observation in the adjuvant setting of RCC [Pizzocaro et al. 2001; Messing et al. 2003; Clark et al. 2003; Passalacqua et al. 2007; Atzpodien et al. 2001; Jocham et al. 2004; Wood et al. 2008].
Several trials are investigating the adjuvant use of targeted treatment in RCC. Data from randomized trials testing sorafenib (SORCE trial), axitinib (ATLAS trial), pazopanib (PROTECT trial) and everolimus (EVEREST S0931) versus placebo are not published yet (by the end of June 2016; Sorafenib in Treating Patients at Risk of Relapse After Undergoing Surgery to Remove Kidney Cancer (SORCE) [ClinicalTrials.gov identifier: NCT00492258]; Adjuvant Axitinib Therapy of RCC in High Risk Patients (ATLAS) [ClinicalTrials.gov identifier: [NCT01599754]; A Study to Evaluate Pazopanib as an Adjuvant Treatment for Localized Renal Cell Carcinoma (RCC; PROTECT) [ClinicalTrials.gov identifier: NCT01235962]; Everolimus in Treating Patients With Kidney Cancer Who Have Undergone Surgery (EVEREST S0931) [ClinicalTrials.gov identifier: NCT01120249].
Sunitinib was tested in two randomized trials (ASSURE and S-TRAC). The ASSURE trial was a double-blind placebo-controlled randomized phase III trial that compared 54 weeks of sunitinib or sorafenib with placebo in the adjuvant setting of 1943 patients with resected RCC at high risk for recurrence. Patients were randomly assigned (1:1:1) to receive sunitinib, sorafenib or placebo. The primary endpoint of disease free survival (DFS) was not significantly different between each experimental arm and the placebo arm [median DFS for sunitinib 5.8 years (HR for sunitinib versus placebo 1.02; 97.5% CI 0.85–1.23; p = 0.8038), for sorafenib 6.1 years (HR for sorafenib versus placebo 0.97; 97.5% CI 0.80–1.17; p = 0.7184) and for placebo 6.6 years]. Substantial treatment discontinuation due to toxicity occurred in the sunitinib and sorafenib arm [Haas et al. 2016].
S-TRAC is a phase III randomized trial, which tested sunitinib for 1 year versus placebo in the adjuvant setting of more than 670 patients with resected RCC at high risk of recurrence (A Clinical Trial Comparing Efficacy And Safety Of Sunitinib Versus Placebo For TheTreatment Of Patients At High Risk Of Recurrent RCC (S-TRAC) [ClinicalTrials.gov identifier: NCT00375674]. A press release by the drug company Pfizer on 8 July 2016 announced, that the trial met its primary endpoint DFS, while the adverse events were consistent with the known safety profile of sunitinib [Pfizer Press Release, 2016]. At the time of writing this review, no other information is in the public domain, but results are expected to be presented at the ESMO 2016 Congress in Copenhagen in October 2016. It has to be waited until the full results are published to see, if sunitinib has a potential use in the adjuvant setting of patients with resected RCC at high risk of recurrence.
Immunotherapy and future perspectives
Immunotherapy with IL-2 has a curative potential in a small subset of mRCC patients, but its role has been replaced by targeted agents (TKI and VEGF inhibition) due to higher rates of clinical benefit and better toxicity profiles [Gore et al. 2010].
However, the new generation of immunotherapies with immune checkpoint inhibitors (e.g. anti-PD1 or anti PDL-1 agents) have shown very promising results in various tumour types including RCC. For example, nivolumab, the PD1 checkpoint inhibitor has been compared with everolimus at second-line following sunitinib failure (CheckMate 025 trial). Nivolumab was superior to everolimus in terms of median OS (25.0 versus 19.6 months; HR 0.73; p = 0.002), ORR (25% versus 5%; p < 0.001) and tolerability (frequency of grade 3 or 4 adverse events 19% versus 37%), respectively [Motzer et al. 2015]. Nivolumab is likely to become a standard of care in the second-line treatment of mRCC following these results.
Sunitinib was initially investigated as a novel first-line treatment to replace interferon. Now it is frequently the comparator arm in first-line trials against novel agents. Preliminary results from a phase I study that investigates the anti-PD1 antibody nivolumab in combination with sunitinib, pazopanib or ipilimumab (Checkmate016), have been mentioned above [Amin et al. 2014; Nivolumab (BMS-936558; MDX-1106) in Combination with Sunitinib, Pazopanib, or Ipilimumab in Subjects with Metastatic Renal Cell Carcinoma (RCC; CheckMate 016) [ClinicalTrials.gov identifier: NCT01472081]. Another phase I and II trial compares varlilumab (anti-CD27 antibody) and sunitinib and is currently (by the end of June 2016) recruiting (A Study of Varlilumab (Anti-CD27) and Sunitinib in Patients with Metastatic Clear Cell Renal Cell Carcinoma [ClinicalTrials.gov identifier: NCT02386111]. Several phase III trials are comparing immunotherapy in combination against the standard first-line sunitinib treatment. A randomized phase III trial (CheckMate 214) of nivolumab plus ipilimumab versus sunitinib in first-line treatment of mRCC is ongoing, but not recruiting patients to date (by the end of June 2016; Nivolumab Combined with Ipilimumab Versus Sunitinib in Previously Untreated Advanced or Metastatic Renal Cell Carcinoma (CheckMate 214) [ClinicalTrials.gov identifier: NCT02231749]. Another phase III trial (JAVELIN Renal 101) is comparing avelumab (anti-PDL-1 antibody) with axitinib versus sunitinib and currently (by the end of June 2016) recruiting patients (A Study of Avelumab with Axitinib Versus Sunitinib In Advanced RCC (JAVELIN Renal 101) [ClinicalTrials.gov identifier: NCT02684006]. A further phase III trial investigates atezolizumab (anti-PDL-1 antibody) in combination with bevacizumab versus sunitinib and is currently (by the end of June 2016) recruiting patients (A Study of Atezolizumab in Combination with Bevacizumab Versus Sunitinib in Participants with Untreated Advanced Renal Cell Carcinoma [ClinicalTrials.gov identifier: NCT02420821].
Sunitinib has been a standard first-line treatment in mRCC for the last decade. The main question in the coming years will be where sunitinib will have its position with regard to the new immune-checkpoint inhibitors. Will sunitinib lose its role as a preferred first-line option to the new-checkpoint-inhibitors, will it keep its role as standard single agent treatment or will there be a usage in combination with immune-checkpoint inhibitors?
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.