
Abstract
The beneficial effect of cytoreductive nephrectomy on survival of patients with metastatic renal cell carcinoma in the immunotherapy era was based on two prospective randomized trials. Unfortunately, such evidence does not yet exist in the present-day period of targeted therapy. Despite this, cytoreductive nephrectomy remains integral in the multimodal management of patients with metastatic renal cell carcinoma. Multiple retrospective studies as well as data from prospective studies examining targeted therapy support the continued use of cytoreductive nephrectomy in the properly selected patient. Ongoing studies will hopefully fine-tune the role and timing of cytoreductive nephrectomy in the context of targeted therapy.
Introduction
Thirty percent of patients diagnosed with renal cell carcinoma (RCC) present with synchronous metastatic disease [Lam et al. 2005]. Improved understanding of the molecular mechanisms underlying the development and progression of RCC led to identification and institution of agents that target either the vascular endothelial growth factor receptor (VEGF-R) or mammalian target of rapamycin pathways. Since 2005, multiple drugs from each class have been approved and are now the standard of care in the management of patients with metastatic RCC (mRCC), based on improvement in both progression-free (PFS) and overall survival (OS) and a better toxicity profile when compared with immunotherapy [Hudes et al. 2007; Motzer et al. 2007; Di Lorenzo et al. 2009; Escudier et al. 2010; Sternberg et al. 2010]. The beneficial use of cytoreductive nephrectomy (CN) prior to the targeted therapy era was established from level 1 evidence demonstrating improved survival in patients undergoing CN prior to interferon α-2b (IFNα) therapy compared with patients treated with IFNα therapy alone [Flanigan et al. 2001, 2004; Mickisch et al. 2001]. Unfortunately, no level 1 evidence currently exists regarding the role of CN in the era of targeted therapy, raising questions about its continued use.
Historical perspective
Prior to the introduction of immunotherapy, CN was primarily reserved for the palliation of symptoms (e.g. bleeding, intractable pain, uncontrolled hypertension or hypercalcemia due to paraneoplastic syndromes, etc.) although reports did exist demonstrating complete resolution of metastases, albeit a very rare event (0.4–0.8%), in patients with metastatic disease who underwent nephrectomy without systemic therapy [Marcus et al. 1993]. During the early years of immunotherapy, controversy existed as to whether or not CN was beneficial. Studies demonstrated an improved response to immunotherapy in patients undergoing debulking surgery compared with those patients treated with the primary tumor still in place [Fisher et al. 1988; Atkins et al. 1993]. However, disease progression and the morbidity associated with CN prevented a significant percentage (up to 77% in one series) of patients from receiving subsequent interleukin 2 (IL-2) therapy [Bennett et al. 1995].
Investigators at Tufts University were the first to devise strict criteria as to which patients might benefit from CN prior to systemic therapy: The ability to debulk at least 75% of the tumor burden, absence of brain, liver, and bone metastases, an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1, clear cell histology, and adequate cardiac and pulmonary function [Fallick et al. 1997]. The authors identified 28 eligible patients based on these criteria and found that 93% of these patients were able to subsequently undergo systemic therapy with IL-2 and, importantly, at least 40% demonstrated at least a partial therapeutic response [Fallick et al. 1997]. From these data, the authors concluded that CN can be beneficial prior to systemic therapy in the properly selected patient.
Level 1 evidence for the survival benefit of CN prior to immunotherapy in patients with mRCC was based on two randomized prospective trials published in 2001. The European Organization for the Research and Treatment of Cancer (EORTC) trial 30947 enrolled 85 patients (42 randomized to CN followed by IFNα treatment and 43 randomized to IFNα alone) and found that both PFS and OS were increased in the CN plus IFNα group [5 versus 3 months (p = 0.04) and 17 versus 7 months (p = 0.03), respectively] [Mickisch et al. 2001]. Similarly, the Southwestern Oncology Group (SWOG) trial 8949 examined 241 patients with mRCC (120 randomized to CN followed by IFNα treatment and 121 treated with IFNα alone) and found that median OS was increased in the surgery group (11.1 versus 8.1 months, p = 0.05) [Flanigan et al. 2001]. In a combined analysis of these two trials, median OS was higher in the surgery group (13.6 versus 7.8 months) with a 31% decreased risk of death in patients undergoing surgery (p = 0.002) (Figure 1) [Flanigan et al. 2004]. Importantly, both trials enrolled only patients with a reasonable performance status. Although these trials were based on treatment with IFNα, Pantuck and colleagues applied the entrance criteria from the SWOG study to a cohort of patients with mRCC treated at their institution with CN followed by IL-2 [Pantuck et al. 2001]. The authors found that median survival of patients treated with nephrectomy plus IL-2 was significantly higher than patients undergoing surgery plus IFNα in the SWOG study (16.7 versus 11.1 months, p < 0.05). Collectively, these studies demonstrated that debulking nephrectomy followed by adjuvant immunotherapy improved survival of patients with mRCC.

Combined analysis of European Organization for the Research and Treatment of Cancer (EORTC) and Southwestern Oncology Group (SWOG) prospective randomized trials [Flanigan et al. 2004]. IFN, interferon.
Cytoreductive nephrectomy in the targeted therapy era
With the advent of targeted therapy, the utility of nephrectomy in patients with mRCC came into question. With data demonstrating improved survival and tolerability of targeted therapy compared with immunotherapy, there was concern that the morbidity of surgery might delay or even prevent patients from receiving systemic therapy. Since targeted therapeutics would in theory treat all tumor sites and based on a lack of definitive data showing that nephrectomy may alter outcomes in conjunction with targeted therapy, it would seem reasonable that usage of CN may decrease. In fact, studies have shown that rates of CN decreased somewhat after the introduction of targeted therapy in 2005, although the demographics of the surgery population largely remained the same [Tsao et al. 2013; Conti et al. 2014]. Patients with mRCC most likely to have undergone CN in the immunotherapy era and early years of targeted therapy were younger, white, male, and had higher stage tumors [Tsao et al. 2013; Culp et al. 2014]. Nonetheless, CN usage after 2005 remained greater than 35% indicating that, at least initially, there was an a priori assumption that the survival benefit of CN would be present regardless of the type of systemic therapy a patient received. Potential theories as to why CN would provide the same benefit include removal of immunosuppressive cytokines and tumor-promoting growth factors, the latter especially important in the context of targeted therapy since previous studies demonstrate decreased levels of circulating VEGF after nephrectomy [Sato et al. 1999; Rini et al. 2009].
Current prospective trials
There is currently no level 1 evidence supporting the use of CN in the context of targeted therapy. To prospectively examine the role of CN in relation to targeted therapy, two large randomized trials are ongoing. The Clinical Trial to Assess the Importance of Nephrectomy (CARMENA) [ClinicalTrials.gov identifier: NCT0093033] examines nephrectomy followed by sunitinib treatment compared with sunitinib only in patients with mRCC. Initiated in 2009, this phase III noninferiority trial enrolls patients with metastatic clear cell RCC and an ECOG performance status of 0 or 1. With a goal of 576 patients, this trial is still recruiting patients with an estimated study completion time of February 2018. The EORTC Immediate Surgery or Surgery After Sunitinib Malate in Treating Patients with Metastatic Kidney Cancer (SURTIME) [ClinicalTrials.gov identifier: NCT01099423] assesses the timing of nephrectomy relative to treatment with sunitinib. Initiated in 2010, this trial randomizes patients with mRCC to either nephrectomy followed by treatment with sunitinib or to three courses of sunitinib therapy with subsequent nephrectomy. With an estimated recruitment of 458 patients, the primary and secondary outcomes of this trial are PFS and OS, respectively.
There has been some controversy about the current prospective trials and whether or not they are designed to appropriately address the survival benefit of CN in the era of targeted therapy. First, CARMENA is a noninferiority trial (i.e. is sunitinib therapy alone equivalent to sunitinib plus surgery?) and, as such, its results may underestimate the benefit of cytoreductive surgery. Second, the EORTC SURTIME trial examines the timing of targeted therapy relative to nephrectomy. Since every patient undergoes surgery, the true benefit of cytoreduction is not addressed. Both of these trials enroll only patients with an ECOG performance status of 0 or 1 and diagnosed with clear cell mRCC, therefore excluding a significant percentage of patients diagnosed with mRCC. This, in combination with sunitinib being the only targeted agent examined in these trials, questions whether or not results from these trials will be generalizable to the ‘real-world’ experience of multiple histologies of RCC as well as the number of currently approved targeted drugs.
Supporting evidence for continued use of cytoreductive nephrectomy
The continued use of CN in the multimodal management of patients with mRCC is supported by the fact that in studies evaluating targeted therapy, the majority (67–100%) of patients had undergone nephrectomy prior to initiation of systemic therapy [Escudier et al. 2007, 2010; Hudes et al. 2007; Motzer et al. 2007; Rini et al. 2010; Sternberg et al. 2010; Tsao et al. 2013]. In the prospective randomized trial evaluating sunitinib versus IFNα, a subgroup analysis found that PFS was increased in patients undergoing CN compared with patients treated with sunitinib alone (11 versus 6 months) [Motzer et al. 2007]. In addition, multiple retrospective studies have been performed over the past decade supporting a benefit of CN in the context of targeted therapy. In an expanded access trial evaluating patients treated with sunitinib with or without prior nephrectomy (including partial resection), Szczylik and colleagues found that patients with a history of nephrectomy but no cytokine treatment had both an improved PFS (12.0 versus 6.5 months, p = 0.0021) and OS (19.0 versus 11.1 months, p < 0.0001) compared with patients treated with sunitinib and the primary tumor in situ [Szczylik et al. 2008]. In a study of 314 patients treated with anti-VEGF therapy from multiple institutions in North America, Choueiri and colleagues found that, after adjusting for documented prognostic factors, CN was an independent predictor of decreased risk of death [hazard ratio (HR) 0.68, 95% confidence interval (CI) 0.46–0.99; p < 0.01] and median OS was significantly higher (19.8 versus 9.4 months, p < 0.01) in patients undergoing CN prior to treatment with anti-VEGF therapy (sunitinib, sorafenib or bevacizumab) [Choueiri et al. 2011]. Important to note is that patients from the CN group were younger had lower corrected serum calcium levels and a better Karnofsky performance status [Choueiri et al. 2011]. The largest retrospective study published to date used the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) to identify patients with synchronous mRCC and examine survival [Heng et al. 2014]. This study included patients from multiple institutions around the world and did not exclude patients based on type of targeted therapy used. Out of a total of 1658 patients, 982 (59.2%) underwent CN. Median OS was significantly higher in patients undergoing CN (20.6 versus 9.5 months, p < 0.01) and, after adjusting for prognostic risk factors, patients undergoing nephrectomy had a 40% decreased risk of death (HR 0.60, 95% CI 0.52, 0.69; p < 0.0001) (Figure 2) [Heng et al. 2014].

Overall survival of patients with metastatic renal cell carcinoma (n = 1633) undergoing treatment with targeted therapy based on cytoreductive nephrectomy (CN) versus no CN [Heng et al. 2014]. CI, confidence interval; HR, hazard ratio; OS, overall survival.
Importance of patient selection
When considering the utility of CN as part of the multimodal management of patients with mRCC, debate continues as to whether there are subsets of patients that will not benefit from surgery compared with treatment with targeted therapy alone. In an evaluation of 141 patients undergoing CN, Kutikov and colleagues found that 30% of these patients were not able to undergo subsequent systemic therapy [Kutikov et al. 2010]. Reasons for not proceeding to systemic treatment after surgery included rapid disease progression (30%) and perioperative mortality (19%) [Kutikov et al. 2010]. Studies have shown that perioperative mortality is significantly higher in patients with mRCC. Using the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) database, Cloutier and colleagues examined 30-day mortality of patients undergoing nephrectomy in the USA between 1988 and 2004 [Cloutier et al. 2009]. Patients with mRCC (all T stages) had a 30-day mortality of 4.2% compared with 0.3% and 1.3% for patients with T1–2N0M0 and T3–4N0–2M0, respectively. Importantly, 30-day mortality was increased to 10.5% in patients with mRCC aged 80 years or older [Cloutier et al. 2009]. Similarly, in a single institutional study of 404 patients, Kader and colleagues found that 30-day mortality in older patients (⩾75 years) was 21% compared with 1.1% in younger patients (⩽75 years) (p < 0.01) [Kader et al. 2007]. More recently, using a population-based cohort of 3300 patients with mRCC undergoing CN, Sun and colleagues demonstrated that perioperative mortality was 2.2 times more likely in older patients (⩾75 years) (4.8% versus 1.9%, p < 0.001) [Sun et al. 2012]. Similarly, perioperative morbidity is higher in patients with mRCC undergoing CN [Abdollah et al. 2011].
In order to maximize the usefulness of CN in the management of mRCC, it is necessary to first identify prognostic factors predictive of survival in patients diagnosed with mRCC. Prior to 2005, multiple prognostic models were developed based on cytokine-based therapy and experiences from individual institutions [Motzer et al. 2002; Negrier et al. 2002; Manola et al. 2011]. This most widely used model, developed in the context of immunotherapy, is from the Memorial Sloan-Kettering Cancer Center (MSKCC) [Motzer et al. 2002]. The MSKCC model was based on 463 patients with mRCC treated with IFNα in the context of clinical trials [Motzer et al. 2002]. It stratifies patients into favorable (no risk factors), intermediate (one to two risk factors) or poor risk (three or more risk factors) groups based on the presence of five prognostic factors (Table 1). Following the introduction of targeted therapy, additional models were developed based on patients treated with VEGF-directed therapy. In a single-institutional study, Choueiri and colleagues identified 120 patients with metastatic clear cell RCC treated with VEGF-directed therapy (sunitinib, sorafenib, bevacizumab or axitinib) as part of prospective clinical trials at the Cleveland Clinic [Choueiri et al. 2007]. From this, the authors identified five factors to be independent predictors of reduced PFS (Table 1). This report was followed by a larger, multi-institutional study by Heng and colleagues which examined OS of 645 patients treated with anti-VEGF therapy (sunitinib, sorafenib or bevacizumab). The authors found that four of the five MSKCC prognostic factors were still independent predictors of OS in patients with mRCC treated with VEGF-directed therapy [Heng et al. 2009]. In addition, the authors found that neutrophil and platelet counts above normal were also independent predictors of survival (Table 1) [Heng et al. 2009]. As with the MSKCC model, patients were stratified into favorable (no risk factors), intermediate (one or two risk factors) or poor (three or more risk factors) risk groups. Two-year survival was 75% in the favorable risk group and median OS was 27 and 8.8 months in the intermediate and poor risk groups, respectively. Heng and colleagues subsequently validated their model using 1028 patients from the IMDC separate from those patients used in the original study [Heng et al. 2013]. The authors found that all six prognostic factors originally identified were also independent predictors of inferior OS in the external validation study with median OS rates of 43.2 months (favorable risk), 22.5 months (intermediate risk) and 7.8 months (poor risk). In addition, higher concordance indices were observed and the 2-year reported versus predicted death number being most similar with the IMDC model compared with the MSKCC, Cleveland Clinic Foundation, International Kidney Cancer Group, and the updated French model adapted to the AVOREN trial [Heng et al. 2013]. Importantly, one important aspect of the IMDC model differentiating it from the other models is that it is based on consecutive patients diagnosed with mRCC and not excluded based on clinical trial eligibility which potentially makes it more generalizable to the ‘everyday’ mRCC patient population.
Prognostic models developed for patients with metastatic renal cell carcinoma.

ECOG, Eastern Cooperative Oncology Group; IMDC, International Metastatic Renal Cell Carcinoma Database Consortium; MSKCC, Memorial Sloan-Kettering Cancer Center; RCC, renal cell carcinoma.
Identifying patients suitable for cytoreductive nephrectomy
Although the above-mentioned models are important in assessing survival of patients with mRCC treated with targeted therapy and their suitability for clinical trials, the ultimate goal from a surgical standpoint is to identify those variables known prior to surgery predictive of who will benefit from CN. In a series from the MD Anderson Cancer Center (MDACC), Culp and colleagues retrospectively examined OS of 576 patients undergoing CN [Culp et al. 2010]. The authors subdivided surgical patients into two groups based on an OS of 8.5 months, the point at which survival of surgical patients diverged compared with a cohort of nonsurgical patients (n = 110). Multivariable Cox proportional regression analyses were performed using all clinical and pathological variables that would be known at the time of surgery. From this, a total of seven preoperative factors independently associated with decreased patient survival were identified: Serum albumin below normal, lactate dehydrogenase above normal, clinical tumor stage at least T3, liver metastasis, symptoms at presentation due to a metastatic site, retroperitoneal lymphadenopathy, and supradiaphragmatic lymphadenopathy. Decreased OS and increased risk of death were both positively correlated with the number of prognostic factors. Importantly, patients with four or more of the seven prognostic factors did not appear to have benefited from surgery compared with the nonsurgical patient cohort (Figure 3). Data from this study, in addition to perioperative as well as final pathological variables, were subsequently used to develop models predicting cancer-specific survival at 6 and 12 months postoperatively [Margulis et al. 2013].

Overall survival of patients with metastatic renal cell carcinoma undergoing cytoreductive nephrectomy (CN) based on the number of preoperative prognostic factors. Solid line corresponds to patients treated with medical therapy alone [Culp et al. 2010].
In a population-based study of 2478 patients with mRCC undergoing CN between 2005 and 2010, the time period corresponding with the initial use of targeted therapy, Culp and colleagues identified factors associated with disease-specific survival (DSS) in this cohort of patients [Culp et al. 2014]. The authors found that primary tumor size at least 7 cm, clinical American Joint Committee on Cancer stage at least T3, high Fuhrman nuclear grade (3 or 4), sarcomatoid histology, regional lymphadenopathy, both distal lymph node and visceral metastases, age at least 60 years, and African-American race were each independently predictive of decreased DSS in patients undergoing CN. The increased number of factors was inversely correlated with DSS (p < 0.001) and patients with up to two, three or four, or at least five factors exhibited median DSS intervals of 40 (95% CI 36–43), 18 (95% CI 17–20) and 7 (95% CI 6–9) months, respectively (Figure 4). Notably, this study was limited by the lack of laboratory data as well as patient performance status, both of which would influence DSS as evidenced in other studies.
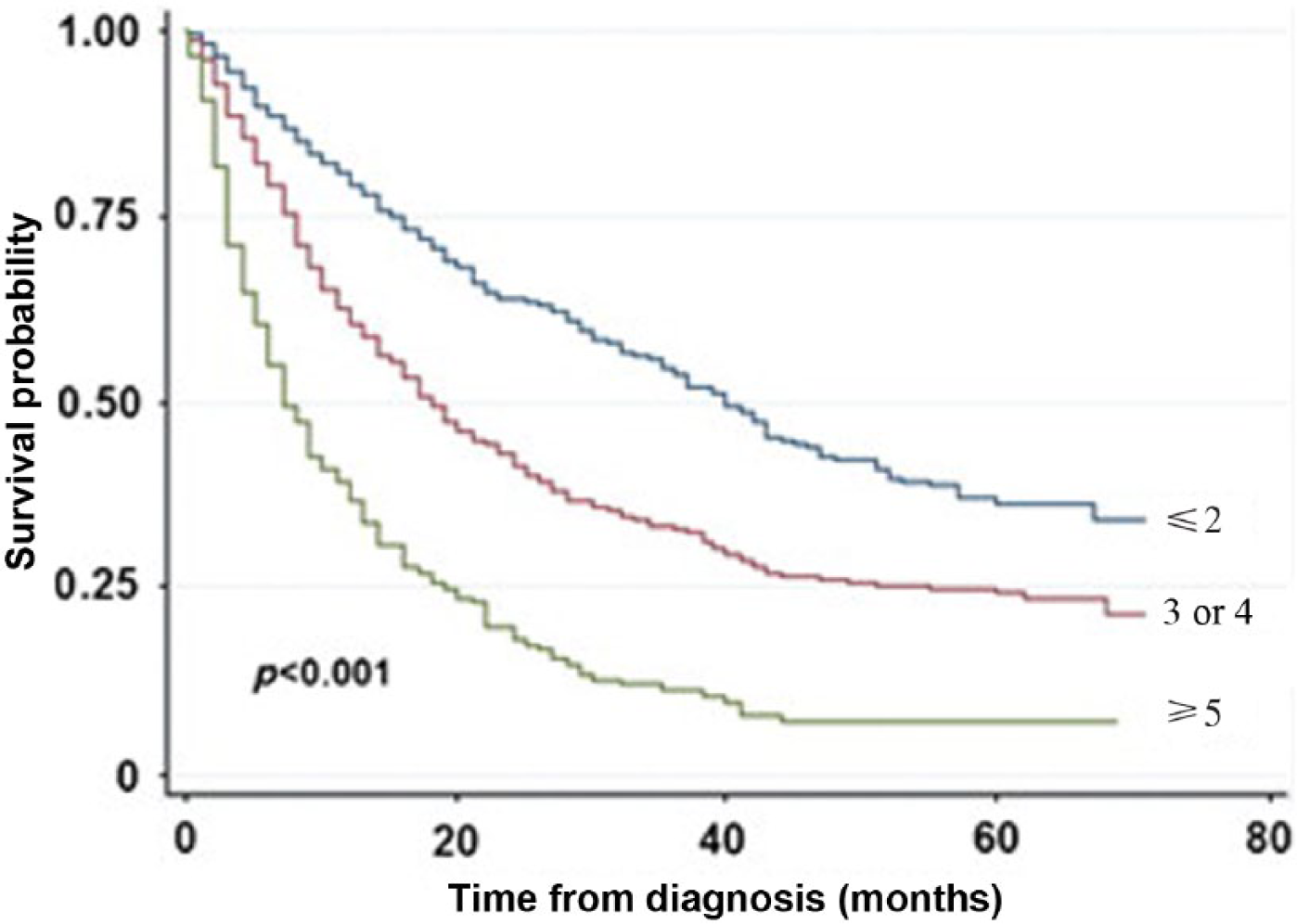
Disease-specific survival of patients with metastatic renal cell carcinoma who underwent cytoreductive nephrectomy (CN) based on number of adverse prognostic factors (National Cancer Institute Surveillance, Epidemiology, and End Results 2005–2010) [Culp et al. 2014].
Based on all of the predictive models developed to date, it is evident that no single factor, but rather the confluence of multiple factors, is predictive of outcome in patients with mRCC regardless of whether CN is performed. That being said, patient performance status is likely the one factor that outweighs the rest, especially in terms of surgical suitability. It is important to note that most prospective trials to date, including the EORTC 30947 and SWOG 8949 trials evaluating CN in the context of IFNα, enrolled only those patients with a reasonable (e.g. ECOG or Karnofsky performance status ⩽1% or ⩾80%, respectively) performance status. In the retrospective studies that have included patients with poor performance status, any OS benefit seen with CN is lost when examined in this subgroup of patients. In the study by Choueiri and colleagues, subset analyses were performed separating patients into favorable/intermediate/poor risk groups and also based on Karnofsky performance status (⩾80 versus <80) [Choueiri et al. 2011]. Patients in the poor risk category demonstrated a marginal benefit with CN (p = 0.06). Whereas patients with a good Karnofsky performance status undergoing CN exhibited a significantly better median OS (23.9 versus 14.5 months, p < 0.01), the difference in patients with a Karnofsky performance status less than 80% was not significant (10.1 versus 6 months, p = 0.08). Similar to and likely related to performance status, expected life expectancy seems crucial to experiencing a survival benefit with CN. In the IMDC study by Heng and colleagues, the benefit of CN was positively associated with the longer a patient was expected to survive. After adjusting for IMDC prognostic criteria, no significant survival benefit from CN was seen in patients who survived less than 12 months [Heng et al. 2014]. These results mirrored those of the MD Anderson study whereby no survival benefit of CN was noted in patients dying within 8.5 months of diagnosis [Culp et al. 2010].
Timing of cytoreductive nephrectomy
In the immunotherapy era, CN was typically performed prior to cytokine-based therapy. However, based on improved tolerability, it is reasonable that targeted therapy can be given prior to cytoreductive surgery in order to potentially downstage a primary tumor, improve resectability or assess a patient’s response to systemic therapy [Bex et al. 2010]. In terms of primary tumor response based on size, the largest series to date is from Abel and colleagues at MDACC which examined 168 patients treated with one of a number of targeted agents, the most common being sunitinib (45%) [Abel et al. 2011a]. At a median time of 62 days following initiation of therapy, the median change in maximal diameter of the primary tumor was −7.1%. The greatest change in primary tumor size was seen in patients who demonstrated at least a 10% decrease in tumor size. Importantly, although 41% of patients demonstrated disease progression in the metastatic sites, a 10% or higher response in the primary tumor was significantly associated with either a partial response or stable disease in the sites of metastasis, indicating that response in the primary tumor could be used as a surrogate for overall treatment response. In fact, in a separate study by Abel and colleagues evaluating 75 patients treated with sunitinib, early tumor response (e.g. >10% decrease in maximal primary tumor diameter within 60 days) was an independent predictor of increased OS on multivariable analysis [Abel et al. 2011b] (Figure 5). Based on these data, it would appear that early response (>10% within 60 days) of the primary tumor correlates with overall response as well as OS. Conversely, little or no response within the first 60 days of therapy would indicate less likelihood of the primary tumor responding significantly to targeted therapy. These findings are significant in deciding on whether or not to proceed with CN or to continue with systemic therapy.
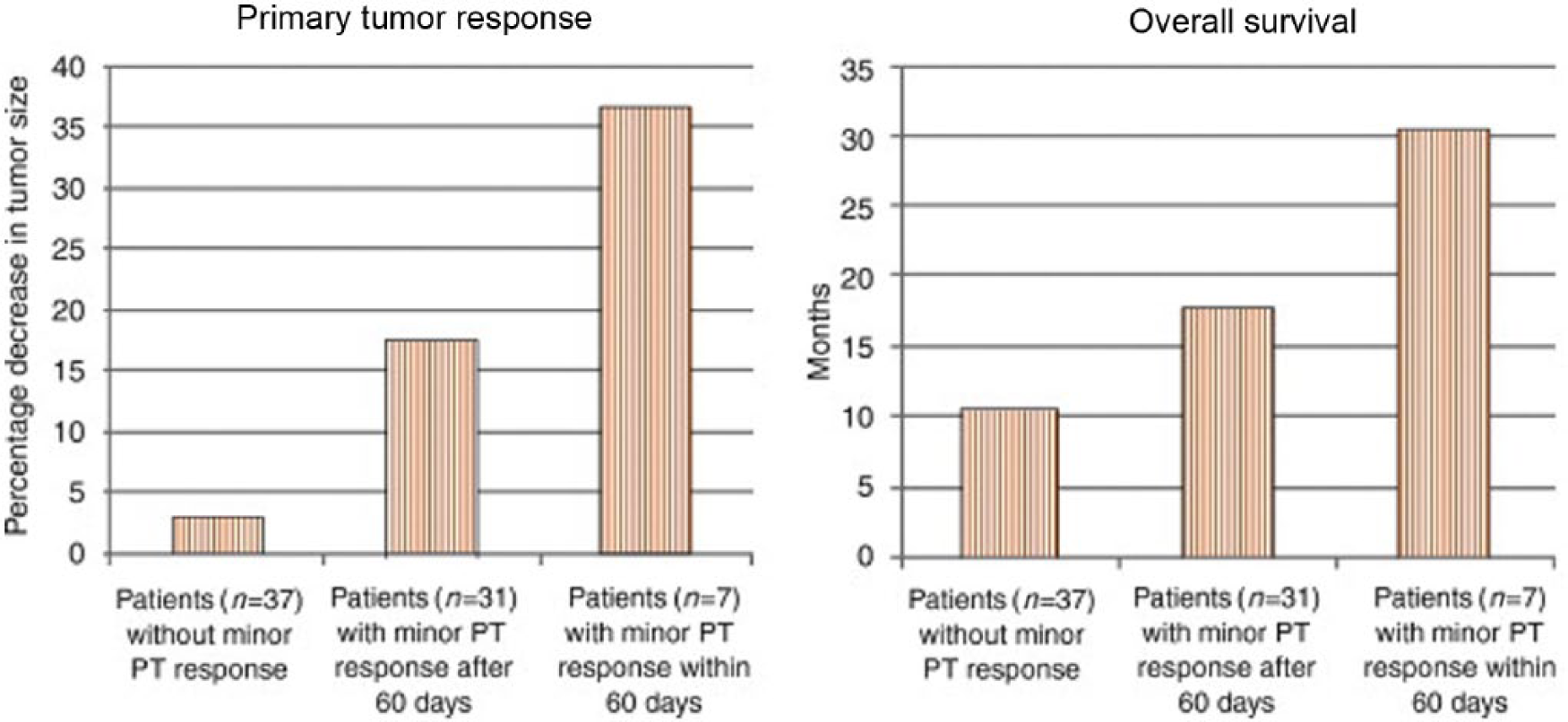
Maximal response of primary tumor to drug and median overall survival based on level of primary tumor response in patients with metastatic renal cell carcinoma treated with sunitinib [Abel et al. 2011b]. PT, primary tumor.
In addition to potentially decreasing primary tumor size, targeted therapy may also decrease the level of a vena caval tumor thrombus. In patients with a tumor thrombus in the inferior vena cava (IVC), surgical morbidity as well as mortality correlates with the level of the tumor thrombus. Therefore, the ability to lessen the tumor burden of a venous tumor thrombus may improve resectability and decrease morbidity. In the largest series to date, Cost and colleagues retrospectively reviewed 25 patients with IVC tumor thrombus (level 2 or higher) treated with targeted therapy [Cost et al. 2011]. After a median treatment of two cycles (range one to six), the majority of patients (21% or 84%) had stable thrombi whereas three (12%) and one (4%) patients showed a decrease and increase in thrombus level, respectively. Importantly, a potential change in surgical approach was seen in only one patient in whom the thrombus level went from IV to III [Cost et al. 2011].
The safety of administering targeted therapy prior to CN was evaluated by Chapin and colleagues [Chapin et al. 2011]. In a retrospective review of 70 patients who underwent pre-CN systemic therapy compared with 103 patients undergoing immediate CN, the authors found that the overall complication rate as well as that of severe complications (e.g. modified Clavien score ⩾3) was no different between groups. However, the administration of targeted therapy prior to CN was associated with increased risk of complications occurring 90 days or more after surgery (p = 0.002), multiple complications (p = 0.013), and those related to wound healing and infection (p < 0.001), the latter most likely related to the fact that the majority of patients underwent systemic treatment with bevacizumab [Chapin et al. 2011]. In a separate report from the same institution comparing 44 patients receiving targeted therapy prior to CN with 58 patients who underwent systemic therapy following surgery, no difference in perioperative mortality or morbidity was observed, with median DSS being similar between groups (27.7 versus 31.0 months, respectively) [Wood and Margulis, 2009]. Ideally, results from the prospective EORTC SURTIME trial will help define the role of presurgical targeted therapy in relation to upfront CN.
Conclusion
The introduction of targeted therapy in 2005 changed the landscape in the treatment of patients with mRCC. Despite lack of level 1 evidence supporting its continued use, CN remains an integral component in the management of properly selected patients with mRCC based on prior prospective studies in the immunotherapy era as well as retrospective data in the context of targeted therapy. Prognostic models have been and continue to be developed to help in identifying those patients most likely to derive a benefit from CN. These, in conjunction with results from ongoing prospective trials, will hopefully define the role of CN in obtaining the maximal benefit for patients with mRCC.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author declares that there is no conflict of interest.