
Abstract
Objectives:
Locally advanced prostate cancer may cause several complications such as haematuria, bladder outlet obstruction, and renal failure due to the ureteral obstruction. Various treatments have been suggested, including radiotherapy, antifibrinolytics, bladder irrigation with alum solution, transurethral surgery and angioembolization, none of which have proven effectiveness. In the last years cryoablation has become a valid therapeutic option for prostate cancer. In our experience we used this ‘new’ technique as haemostatic therapy.
Methods:
We selected four patients with gross haematuria affected by locally advanced hormone refractory prostate cancer, who had already been treated with primary radiotherapy. We used third-generation cryotherapy: under ultrasonographic guidance, we inserted six cryoprobes, two in each of the vascular pedicles reaching at least −60°C, and three thermometers. We then induced two freeze–thaw cycles.
Results:
After the operation the haematuria stopped in all patients and at 9-month follow up we observed a mean of four red cells (range three to five) in the urinary sediment with no evidence of bacteriuria. Prostate volume, prostate-specific antigen and postmicturition residue were significantly reduced. Qmax improved significantly too.
Conclusion:
Our experience has given us good results with minimal intra- and postoperative complications. We think that haemostatic cryotherapy as a palliative approach for locally advanced prostate cancer could represent a valid treatment option and more consideration could be given to its use.
Introduction
Locally advanced prostate cancer (LAPC) may cause several complications such as haematuria, bladder outlet obstruction (BOO), and renal failure due to the ureteral obstruction. These clinical events can cause significant morbidity, an impaired quality of life (QoL) and even mortality. The management of complications of patients with LAPC remains a challenge for urologists but their treatment is still important because it is known that, in the absence of metastases, the chance of survival at 5 years is high. Different treatment options have been suggested, including radiotherapy, antifibrinolytics, bladder irrigation with alum solution, transurethral surgery and angioembolization, none with proven effectiveness [Barrass et al. 2006]. Total pelvic exenteration was also suggested in difficult cases [Leibovici et al. 2005]. In 1996, the American Urological Association (AUA) recognized cryoablation as a therapeutic option for prostate cancer [AUA, 1996]. Considerable technological improvements in cryotherapy, including gas-driven miniaturized equipment, ultrasonographic ice-ball monitoring, and the use of thermal sensors, have allowed more efficient freezing of the prostate gland while reducing collateral damage to surrounding tissues [Babaian et al. 2008]. Contemporary cryotherapy offers the patient a minimally invasive treatment option with low morbidity and shorter hospital stay [Miller, 2012]. We report our experience with focal cryotherapy as a haemostatic treatment of haematuria in four patients with LACP.
Materials and methods
According to standard protocol of the hospitals in which the study was carried out, each patient was informed at admission and signed an informed consent form allowing data collection for research purposes. The study design is in accordance with the Helsinki Declaration and conforms with the Committee on Publication Ethics guidelines. Study design, analysis, interpretation of data, drafting and revisions followed the Strengthening the Reporting of Observational Studies in Epidemiology Statement: guidelines for reporting observational studies, available through the EQUATOR (Enhancing the Quality and Transparency of Health Research) network.
We selected four patients with LACP already treated with primary radiotherapy and affected by hormone refractory disease. All patients had grade 3 haematuria due to invasion of the tumour into the bladder. Two patients were also affected by BOO. All patients underwent abdominal and pelvic computed tomography (CT). Diagnostic cystoscopy showed no macroscopic signs of actinic cystitis, but spontaneous bleeding of the prostatic urethra was observed in all patients. Endoscopic haemostatic treatment was attempted in all patients but was ineffective.
In two patients with prostate-specific antigen (PSA) greater than 10 ng/ml, a bone scan was performed to exclude metastases. Patient characteristics are shown in Table 1. Mean and median patient age were both 76 years (range 70–83 years), mean and median prostate volume were 56.5 and 50 ml, respectively (range 40–86 ml), mean and median PSA were 15.47 and 9.33 ng/ml, respectively (range 8.9–26 ng/ml), and mean and median Qmax at uroflowmetry were 10.4 and 10.75 ml/min, respectively (range 7.1–13.1 ml/min). Mean and median postmicturition residue were 83.5 and 73 ml (range 54–145 ml), and mean and median preoperative haemoglobin were 9.5 and 9.6 gr%, respectively (range 8.4–10.2 gr%). All patients were within the class of high risk of D’Amico’s nomogram.
Pretreatment patient characteristics.

Gr%, granulocytes %; PSA, prostate-specific antigen.
Technique
Cryotherapy was performed, always by the same surgeon, using the Cryo-Care system (Endocare Inc., Irvine, CA, USA). The Cryo-Care system is an argon gas based system that works via pressurized gas expansion at the tip of the cryoneedle. The technique used was described by Onik and colleagues [Onik et al. 1993]. All patients underwent a light bowel preparation the evening before surgery with the administration of oral magnesium citrate and with a Fleet enema (C.B. Fleet Company, Inc., Lynchburg, VA, USA) on the morning of treatment. Bowel preparation was performed in order to reduce faecal contents and air in the rectum to enhance transrectal ultrasonographic imaging of the prostate. All patients underwent antibiotic profilaxis with cefazolin 2 g intravenous (IV). The procedure was performed under general anaesthesia and with the patient in the dorsal lithotomy position. Under ultrasonographic guidance, six cryoprobes were inserted; the position of two probes was changed from standard toward a posterolateral allocation in order to concentrate the freezing action in the pedicles (Figure 1). Three thermocouples were positioned at the left and right neurovascular bundles and midline apex. Denonvilliers trail hydrodissection was not performed due to actinic adhesions. Urethral warming was achieved using a Cook urethral warming catheter (Cook Medical, Bloomington, IN, USA). The entire procedure was conducted under transrectal ultrasound control and ice balls forming were constantly monitored, reaching at least −60°C in both neurovascular bundles (Figure 2). A double freeze–thaw cycle was performed. At the end of the procedure a 18 Ch Foley catheter was placed and maintained for 7 days.
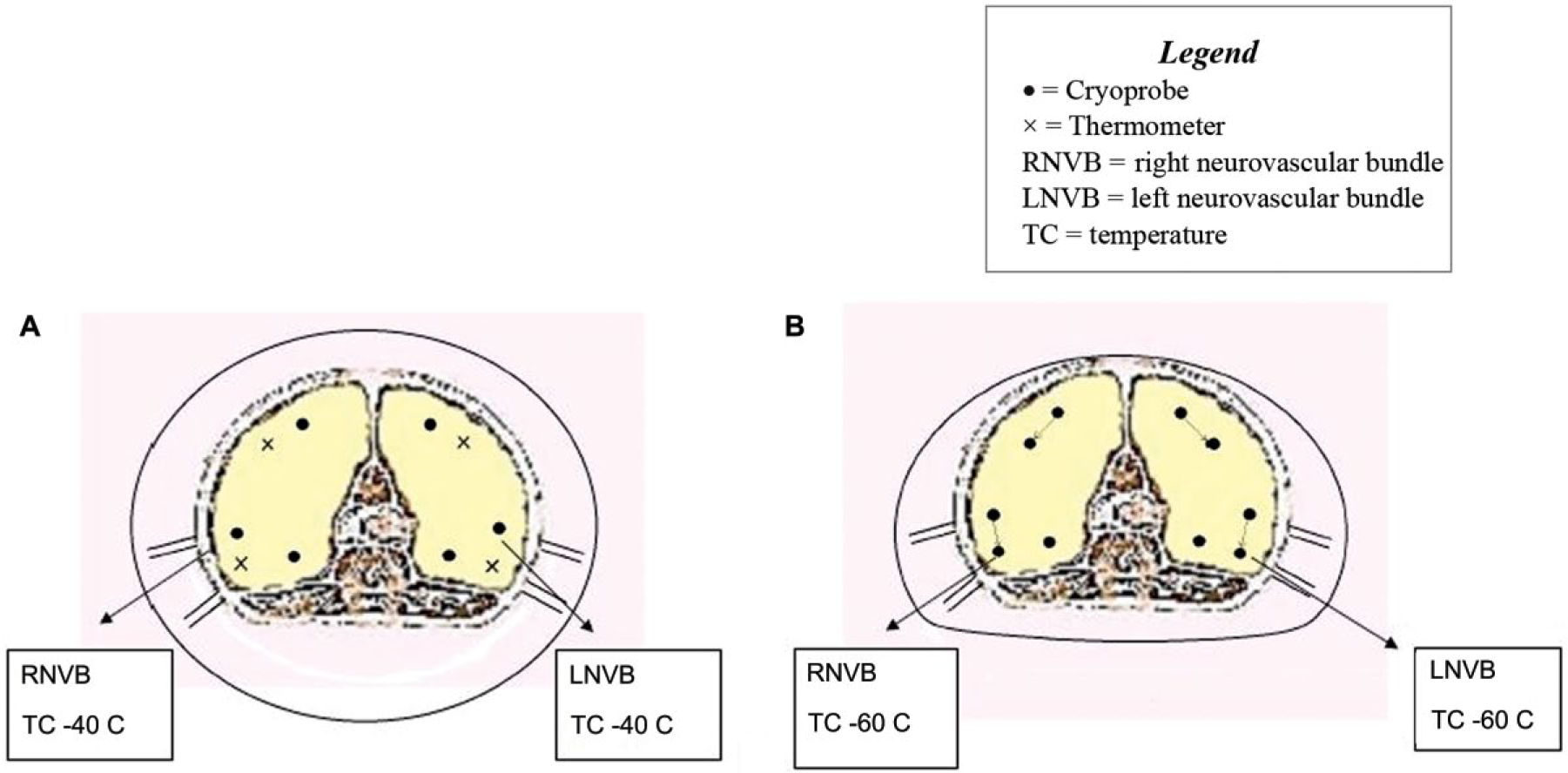
(A) Standard position of the cryoprobes and the thermocouples in a normal prostate cryoablation. In this case the temperature in the neurovascular bundles is −40°C. (B) Changed position of the cryoprobes and the relative freezing area. In this way the temperature in the neurovascular bundles is at least −60° C, with hemostatic effect. LNVB, left neurovascular bundle; RNVB, right neurovascular bundle.

Ultrasonographic appearance. It is possible to see the position of the cryoprobes and the temperature that was reached.
Results
No major complications were recorded in the postoperative period except for a slight perineal haematoma in a patient without any clinical relevance. In one patient it was necessary to give a blood transfusion of 1 unit, but this was the patient who had marked anaemia preoperatively. All patients were discharged after 1 day with a 18 Ch Foley catheter with normochromic urine. The catheter was removed 7 days after surgery. Patients were followed up at our institution at 3, 6 and 9 months with PSA determination, blood and urine tests, uroflowmetry and ultrasonography. Follow-up results are reported in Table 2. In the urinary sediment a mean of four red cells (range three to five) was observed with no evidence of bacteriuria. Prostate volume, PSA and postmicturition residue were significantly reduced. Qmax greatly improved too.
Nine-month follow-up parameters.
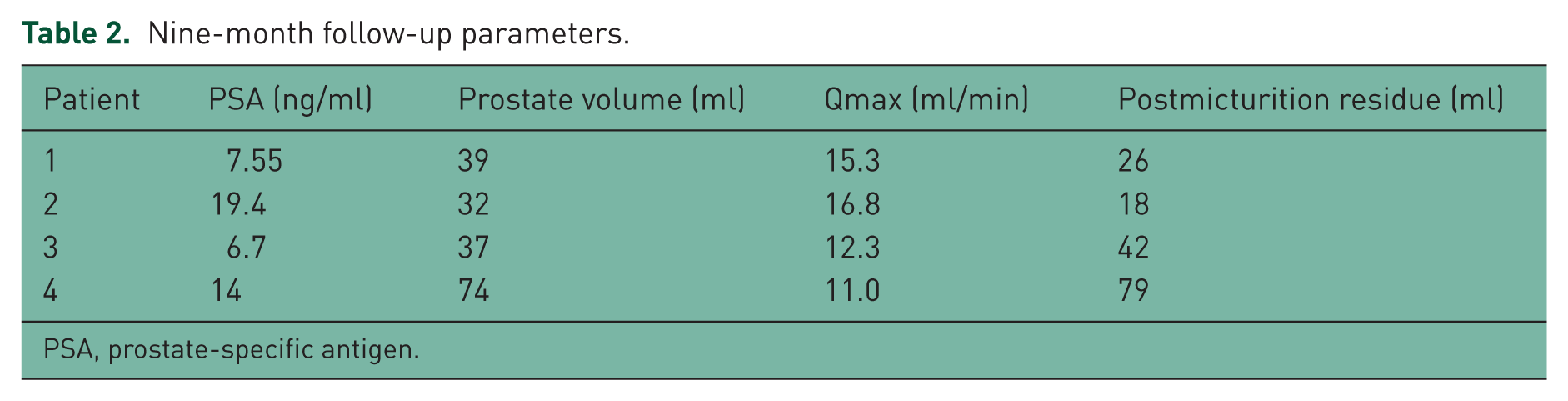
PSA, prostate-specific antigen.
Discussion
The management of intractable haematuria remains a challenge for urologists. Haematuria is graded into four levels of severity: grade 1, microscopic haematuria; grade 2, macroscopic haematuria; grade 3, haematuria with clots, requiring transfusion support; and grade 4, macroscopic haematuria with clots and impaired renal function. Haematuria grades 1 and 2 can be managed medically. The management of haematuria grade 3 and higher requires surgical intervention.
Patients with LACP frequently develop prostatic bleeding that can significantly increase morbidity. Actually there is relatively little evidence for a definitive solution of such a complication. Several therapeutic strategies have been proposed and used but with inconstant and nondurable results. Cystoscopy is useful in the initial management for diagnostic purposes, for clot evacuation, and for fulguration if the bleeding is excessive. In severe cases, local treatment is administered in the form of intravesical agents, such as 1% alum (potassium aluminium sulfate), 1–10% formalin, ε-aminocaproic acid, prostaglandins, silver nitrate and hyperbaric oxygen [Likourinas et al. 1979; Singh and Laungani, 1992]. Radiotherapy and TURP are the most common procedures used. Other treatment options include intravesical fibrin-glue instillation, laser coagulation, percutaneous nephrostomy tube insertion, internal iliac artery embolization, surgical diversion and cystectomy [Choong et al. 2000].
Radiotherapy is well known to be very effective in reducing haematuria in bladder cancer, with acceptable morbidity [Duchesne et al. 2000]. Radiotherapy is also occasionally used to palliate haematuria in prostate cancer, but actually few studies have reported its efficacy [Gibbons et al. 1979].
A palliative TURP is sometimes used to face haematuria in prostate cancer, but its efficacy in controlling bleeding from either benign prostatic enlargement or cancer is not well documented [Crain et al. 2004].
With radiological embolization of the internal iliac arteries, control of haematuria was achieved in 90% of patients [Jenkins and McIvor, 1996] with surprisingly little morbidity (principally gluteal pain in 30%, which is usually self-limiting) that can be further minimized by super-selective embolization of the prostatic branches [Barbieri et al. 2002].
Intravescical treatment with alum (1%) reduces vascular permeability and has been shown to control haematuria effectively in 80–100% of patients, including those with prostate cancer [Thompson et al. 1987].
Our report presents a two-institution study of four consecutive patients affected by LACP complicated with haematuria, who underwent third-generation whole gland salvage cryotherapy in order to control bleeding complications. At 9-month follow up good results were observed regarding the resolution of haematuria, the improvement of BOO, the low rate of complications and the considerable improvement in QoL.
Salvage prostate cryoablation can be performed as a focal (SFC) or a total (STC) treatment, and the choice is related to appropriate patient selection with a biopsy-proven unilateral recurrence. The rate of rectourethral fistula after STC is reported to be between 1% and 3.4% [de Castro et al. 2013; Wenske et al. 2013], and 0 and 5.5% after SFC [Eisenberg and Shinohara, 2008; de Castro et al. 2013; Wenske et al. 2013]. Recently Li and colleagues reported that rectourethral fistula post SFC is not clearly lower than for patients with whole gland salvage cryoablation [Li et al. 2015].
In our experience, the choice of a STC was dictated by the need to treat haematuria after the failure of endoscopic haemostatic treatment, avoiding all the alternative procedures reported in the literature that showed inconsistent results. In our case series no major complications were recorded within the 9-month follow-up period, probably due to the accurate positioning of the cryoprobes under ultrasound guidance.
Although the main intent of our study was to treat the complication of haematuria in patients with LACP, it is interesting to note that the oncological outcomes of the patients treated during the follow up are very encouraging, given the significant reduction in PSA. However, medium- and long-term assessments are necessary in order to confirm the actual advantages from the oncological point of view.
We also believe that the prostate cryotherapy procedure performed on patients with LACP and haematuria does not present important limitations of applicability. It is certainly of great clinical relevance for the easy resolution of haematuria whiles providing considerable improvement in the QoL of patients.
The limitation of our study is the small number of patients treated. Further evaluations are needed in the future with a greater number of patients and longer follow up to confirm our results.
The learning curve of standard prostate cryotherapy is about 20 consecutive cases. Prostate cryotherapy as a palliative treatment for haematuria, given the paucity of cases, should probably be performed in moderate-volume centres by surgeons with proven experience.
Conclusion
Our preliminary results show that focal cryotherapy could represent a simple and safe therapeutic option in patients with LAPC and haematuria, avoiding the use of inconclusive or more complex procedures. Further evaluations with a more consistent number of patients and with longer follow up are still needed before solid conclusions can be drawn.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.